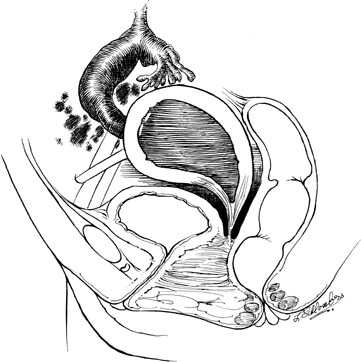
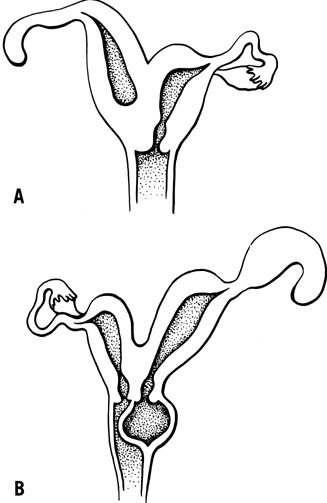
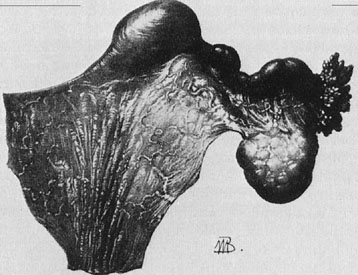
A patient with congenital absence of the müllerian ducts lacks a vagina and uterus. Aplasia or dysplasia of the müllerian ducts is a more accurate term because usually a normal lower vagina has developed, with absence of the middle and upper thirds of the vagina and the uterus. Although the uterus is not present, rudimentary uterine anlagen are often palpable. The tube and ovary are essentially normal (Fig. 1). Although some reported series of congenital absence of the vagina have included patients with the uterus and with absence of various lengths of vagina, these are not generally considered under the heading Rokitansky’s syndrome. There is a homogeneity and specificity of this syndrome (i.e. the absence of a vagina and uterus with a high incidence of urinary tract anomalies), whereas patients with partial agenesis of the vagina or a transverse vaginal septum are considered in the section on disorders of vertical fusion. Patients with disorders of vertical fusion have a low incidence of urinary tract anomalies.
|
Diagnosis
The growth and development of patients with congenital absence of the müllerian ducts is normal, including secondary sex characteristics. The external genitalia are normal in appearance; however, the vagina is absent or there may be only a shallow vaginal pouch of 3 cm in depth. Prior to menarche, the differential diagnosis between an imperforate hymen and Rokitansky’s syndrome may be difficult. Diagnosis may depend on the ability to determine the presence or absence of a uterus. This often may be accomplished by examining the patient under anesthesia. Laparoscopy is rarely necessary. On occasion, however, these patients may have persistent pelvic pain associated with an active rudimentary uterine anlagen. The patient usually complains of cyclic abdominal pain, and at the time of surgery, retention of a small amount of blood is noted in the rudimentary structure.1 On occasion, functioning endometrium may result in considerable unilateral enlargement of the uterine anlage. In either case, excision of the rudimentary horn results in complete relief of symptoms.
The exact nature of the underlying genetic abnormality responsible for Rokitansky’s syndrome is unknown. However, it is possible to deduce the embryologic abnormality most likely to result in defects of the vagina, kidney, and skeleton. The müllerian duct has two components, a cephalic or anterior portion, which is derived from coelomic epithelium, and a caudal end, which is derived from a wolffian or mesonephric duct. The cephalic end of the müllerian duct is the anlagen of the fallopian tubes, and the caudal portions fuse to form the uterus and attach to the urogenital sinus to induce the development of the vagina. As previously noted, these patients have normal ovaries and fallopian tubes, only solid rudimentary uterine horns, and no vagina. This is a precise lesion that would be predicted if the initial phase of müllerian duct development were normal but subsequent development along the wolffian duct was impaired. Thus, the uterine and vaginal segments of the müllerian duct are dysplastic or absent. The urinary tract abnormalities frequently associated with this disorder (i.e. renal absence or ectopia) and the defects of the müllerian duct could result from a common abnormality of the wolffian duct. Skeleton is also derived from the mesoderm at approximately the same stage of development that has been identified for the defect in the urogenital tract (10 to 11 mm). The vertebrae develop from adjacent mesodermal cell concentrations at the same somite level as those of the mesonephros. Thus, a defect in the organization of the mesoderm in these somites could cause skeletal abnormalities, as well as defective mesonephric development and subsequent abnormalities in the kidney, uterus, and vagina.
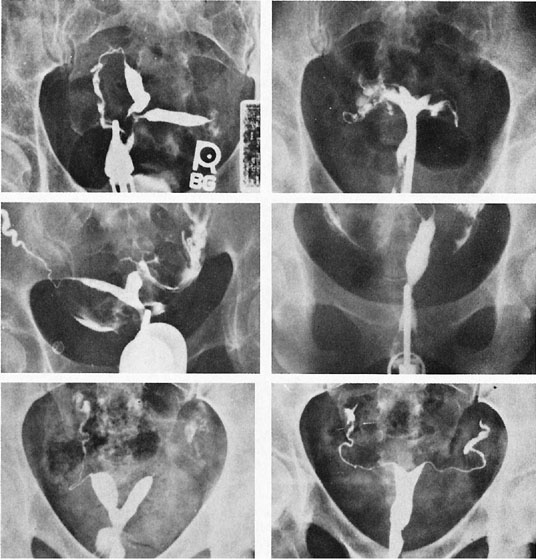
Major defects in the urinary tract system, such as congenital unilateral absence of a kidney or the presence of a pelvic kidney, occur in approximately 15% of patients with congenital absence of the müllerian ducts. However, if trivial anomalies are included, such as malrotation of the kidney, a partial double collection system on one side, or malposition of the kidney, the percentage of abnormalities rises to approximately 40%. Thus, an intravenous pyelogram should be part of a routine evaluation of all patients with congenital absence of the uterus and vagina.
Anomalies of the bony structures are also common. It is generally believed that these anomalies occur in about 5% of patients. Abnormalities in the lumbar spine, such as sacralization of L5 or the presence of six lumbar vertebrae, are observed. Fusion of the cervical vertebrae can also occur. Of interest is the Klippel-Feil syndrome (congenital fusion of the cervical spine, short neck, low posterior hairline), which has been reported in a few patients with congenital absence of the vagina. A variety of other abnormalities, including abnormalities of the hand, inguinal and femoral hernias, and congenital heart lesions, have also been described.
The karyotype of affected patients is characteristically 46XX. Jones and Mermut recorded five examples of sisters with this disorder.2 This raised the possibility of a very rare autosomal recessive disorder; however, evidence of this has not been persuasive. Familial aggregates seem best explained on the basis of polygenic or multifactorial inheritance. Single mutant genes are responsible for the McKusick-Kaufman syndrome and the hand-foot-genital syndrome.3 Hand-foot-genital syndrome is a rare, dominantly inherited condition that affects both the distal limbs and the genitourinary tract. A nonsense mutation of the HOXA13 gene has been identified in several families.4,5 At present, it is not clear whether sporadic cases represent new mutations of a single gene defect that is responsible for the familial disorder or are due instead to multifactorial etiologies.
Clinical Management
PSYCHOLOGICAL COUNSELING.
Various therapies have been suggested for the treatment of patients with Rokitansky’s syndrome. There is, however, complete agreement that all patients should initially have family counseling instituted by the attending physician or a psychologist. Interaction with other affected young women may also be helpful. Weijenborg and terKuile described the use of a group program for women with Rokitansky’s syndrome. They demonstrated that patients felt less anxious, less depressed, and less sensitive to interpersonal contact after participation in the program.6 Continuity of care should be maintained throughout the hospitalization or dilation program, often continuing several years after initial therapy. Most surgeons agree that the single most important factor in determining the success of vaginoplasty is the psychosocial adjustment of the patient to her anomaly; thus, an intensive-counseling program should definitely be addressed before considering any therapeutic modality.
VAGINOPLASTY.
In our institution, three major forms of therapy have been used: the split-thickness graft technique of McIndoe, the Frank technique of vaginal dilation, and the Ingram passive dilation technique. It has been our practice to suggest vaginal dilation as an initial form of therapy. This is quite useful in the motivated patient in whom previous vaginal exploration has not been attempted.7
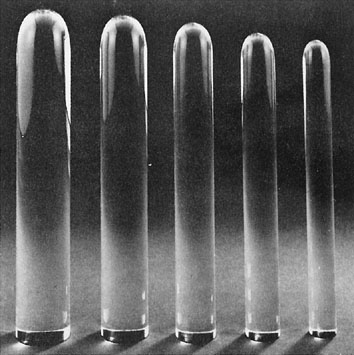
The Ingram technique for passive dilation has several advantages.8 The patient is not required to press the dilator against the vaginal pouch. A series of graduated lucite dilators (Fig. 2) slowly and evenly dilate the neovaginal space. The patient should be carefully instructed in the use of dilators, as recommended by Ingram, beginning with the smallest dilator. The patient is shown and instructed with the use of a mirror how to place a dilator against the introital dimple. The dilator may be held in place with a supportive undergarment and regular clothing worn over this.
|
The patient is shown how to sit on a racing-type bicycle seat, which is placed on a stool 24 inches above the floor. She is instructed to sit leaning slightly forward with the dilator in place for at least 2 hours per day at intervals of 15 to 30 minutes. The patient is followed usually at monthly intervals and can be expected to graduate to the next larger size dilator approximately every month. An attempt at sexual intercourse may be suggested after the use of the largest dilator for 1 or 2 months. Continued dilation is recommended if intercourse is infrequent. In our experience, functional success rates are excellent. Our group recently reported the largest series of vaginal agenesis patients who utilized the Ingram method of dilation to create a neovagina.9 The records of 51 patients with müllerian agenesis were reviewed: 37 patients attempted vaginal dilation and 14 young women underwent a surgical intervention. Functional success was described as satisfactorily achieving intercourse or accepting the largest dilator without discomfort during the clinic visit. All patients were followed for at least 2 years and for an average of 9.25 years. Functional success was achieved in 91.9% of those who attempted dilation (Table 3). Robson and Oliver also reported excellent success with dilation using the Frank method, with only 1 patient of 25 with müllerian agenesis undergoing surgical management.10 All those women who were sexually active reported satisfactory sexual relations. Thus, passive dilation should be suggested as an initial therapy for vaginal creation. If unsuccessful, operative vaginoplasty is indicated.
TABLE 3. Dilation Success and Failure Rates
Group | Total (n) | % |
Successful dilation | 34/37 | 91.9 |
Failed dilation | 3/37 | 8.1 |
Adapted from Roberts CP, Haber MJ, Rock JA: Vaginal creation for müllerian agenesis. Am J Obstet Gynecol 185:1349, 2001
Over the past 25 years, the senior author has had experience with the split-thickness graft technique described by McIndoe to line the neovaginal space. Indications for this procedure include failure of vaginal dilation or patient preference.
The Counsellor-Flor modification of the McIndoe technique uses a rolled foam rubber mold covered with a condom in place of a rigid form.11,12 The initial and important step in this operation is to obtain a satisfactory split-thickness graft. This can be easily obtained with the Padgett electrodermatome, which secures a graft 0.017 to 0.018 inch thick. The graft is also 10 cm wide and long enough to be twice the vaginal depth. The graft is taken from the buttock to render the donor site invisible, that is, within the lower limits of most bathing suits. Either buttock may be used.
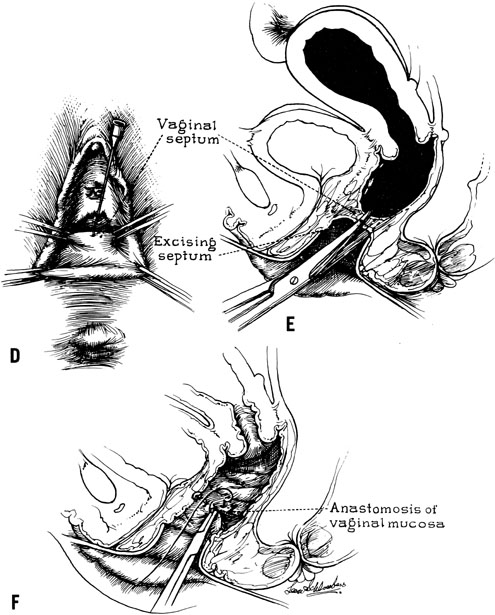
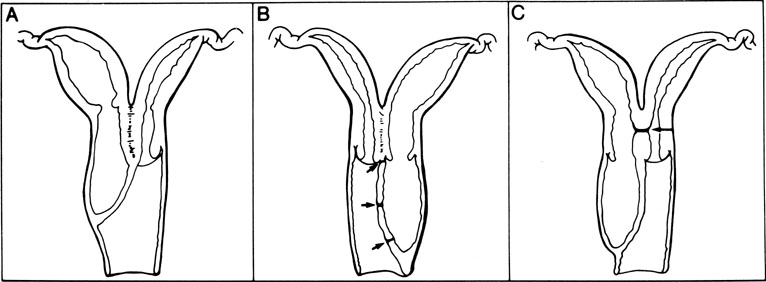
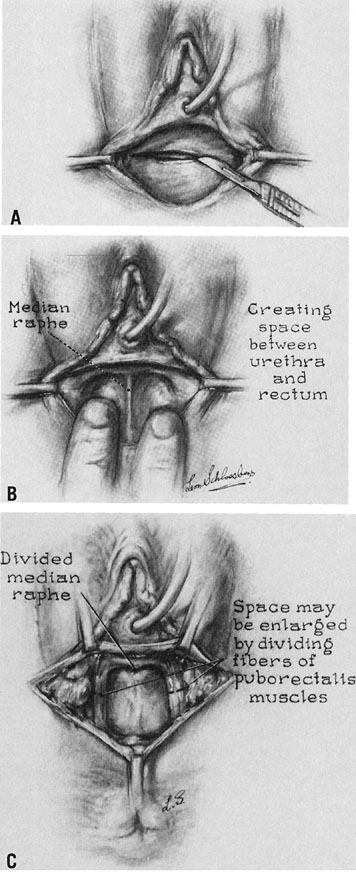
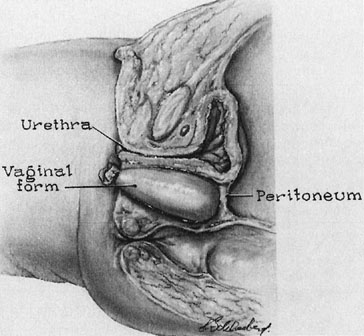
A transverse incision is made at the site of the vaginal orifice. The neovaginal space is developed with digital manipulation. The dissection is easily developed on one or both sides of the median raphe, where the tissue between the bladder and the rectum seems to be condensed almost enough to warrant a designation of a rectourethralis ligament (Fig. 3). The raphe is cut. This dissection should be carried to the peritoneum. However, care must be exercised not to expose too large an area of peritoneum lest an enterocele develop after the procedure.
|
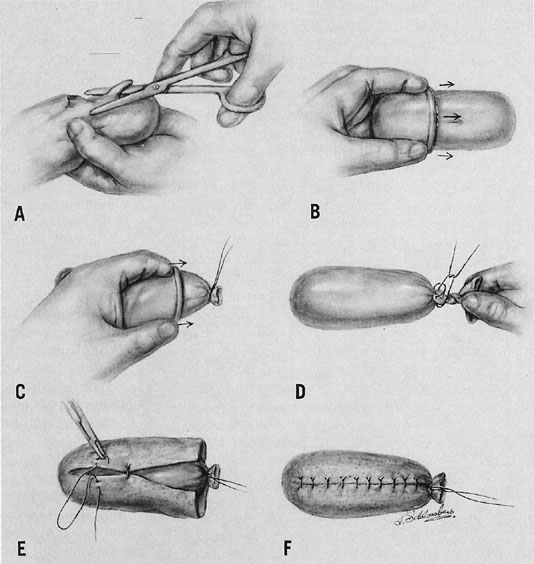
A prosthesis is then developed using foam rubber such as may be obtained from an upholstery shop. This is readily sterilized in blocks about 10 x × 10 x × 20 cm. The foam rubber may be cut to a suitable size using scissors. The form should be cut about twice the desired size and further compressed by covering with two rubber sheaths, which are ordinary condoms. Once compressed, the form is placed into the neovagina and allowed to assume the shape of the space. The end of the condom is then tied so that the proper amount of air is trapped within the foam rubber to conform to the vaginal space. The skin graft is sewn to the form with interrupted, vertical mattress sutures of fine, nonreactive suture so that the exteriorized undersurface of the graft is approximated to exteriorize the undersurface of the sutured edges (Fig. 4).
|
After the graft has been inserted into the cavity, the edges of the graft may be sutured to the cut edges of the vaginal epithelium (Fig. 5). Only a few sutures should be placed, however, to allow drainage of any serum that may collect under the graft. Rather, large braided sutures may be placed through the labia to prevent the extrusion of the form. A suprapubic catheter is recommended to prevent urethral pressure. Postoperatively, the patient should be kept on a low-residue diet, given antibiotics, and kept at bed rest. The labial sutures may be removed in approximately 4 days, while the patient is at bed rest. Seven days after the procedure, the patient is again returned to the operating room; the suprapubic catheter is removed, and the vaginal cavity is irrigated. A second vaginal form may be molded so that the patient has two forms to use at home while the healing process is completed. Twenty-four hours after removal of the original mold, the patient is instructed in self-removal and the use of a low-pressure, clear, warm water douche. After approximately 6 weeks, the soft form is replaced with a Silastic form, which is inserted after it is moistened with tap water.
|
In our series, there have been no serious complications following vaginal creation with the split-thickness graft technique. There have been no fistulas. Abandonment of the balsa wood form, the use of a suprapubic catheter, and careful operative technique are believed to be responsible for the anatomic success, which approaches 90%, of this operative vaginoplasty. The artificial vagina is of sufficient depth and width to allow comfortable sexual relations. Minor complications have been noted in 21 of 79 (26%) patients in our series. These include a small vaginal hematoma with secondary infection (n = 2) and the presence of granulation tissue resulting from variable graft loss (n = 19). The graft take was 100% in 60 patients, 80% to 90% in 14 patients, 60% to 70% in 3 patients, and 50% in 2 patients.7
Several investigators have reported successful modifications of alternative methods of vaginoplasty for patients with vaginal agenesis. With the ease of laparoscopy, modifications of procedures previously performed by laparotomy have gained interest. The Vecchietti approach, using a pulley system to pull the vaginal apex superiorly, has been adapted and performed laparoscopically.13 In addition, the Davydov procedure, dissection of thet rectovesical space and mobilization of the peritoneum to the introitus after a vaginal space has been created, has been adapted for use with the laparoscope.14 These modified techniques certainly offer some advantages owing to the acknowledged benefits of minimally invasive surgery, such as shorter hospital stays and less postoperative discomfort. The authors report excellent success over the initial follow-up period; however, it will be important to continue to gather appropriate long-term data regarding functional success.
Vaginal vault prolapse, after both nonsurgical and surgical treatment of müllerian agenesis, has been described. It is proposed that, owing to the lack of müllerian development and appropriate suspension to the bony pelvis, these women are at risk for vault prolapse. The incidence of prolapse in young women with this disorder is still unknown, regardless of the method of creation of the neovaginal space.15,16,17
In summary, the use of the Ingram method of dilation, coupled with careful instruction and counseling, may meet with good success. In fact, in our experience, the most common reason for failure with vaginal dilation has been an attempt at hymenectomy prior to referral. Thus, a high success rate may be expected in women without previous vaginal surgery. Additionally, dilation obviates the need for hospitalization and the inherent risks of surgery. However, vaginal creation using a split-thickness graft is highly successful in skilled hands and should be offered to those patients unwilling or unable to obtain an adequate neovagina with dilation (Table 4). Preoperative counseling is essential to the success of either procedure.
TABLE 4. Success Following Vaginal Creation for Müllerian Agenesis
Procedure | Patients (n) | Functional Success | Anatomic Success |
Split-thickness graft | 80 | 80 (100%) | 73 (91%) |
Rock JA, Reeves LA, Retto H, et al: Success following vagi-nal creation of müllerian agenesis. Fertil Steril 39:809, 1983