Variants of endometrioid adenocarcinoma include villoglandular, secretory, ciliated
cell, and adenocarcinoma with squamous differentiation. Overall, the
epidemiologic characteristics of the subtypes are similar
to those of typical endometrioid carcinoma; the few exceptions are mentioned
with each section. Because it is not unusual to observe these patterns
in association with the usual form of endometrioid cell type, most
of the lesion must consist of the histologic features of the subtype
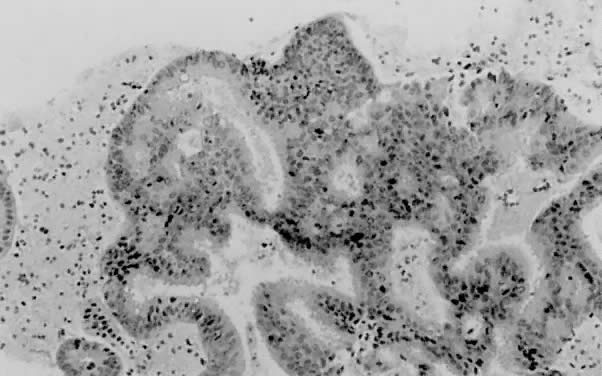
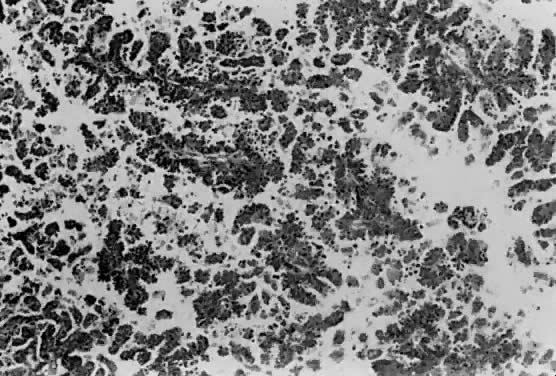
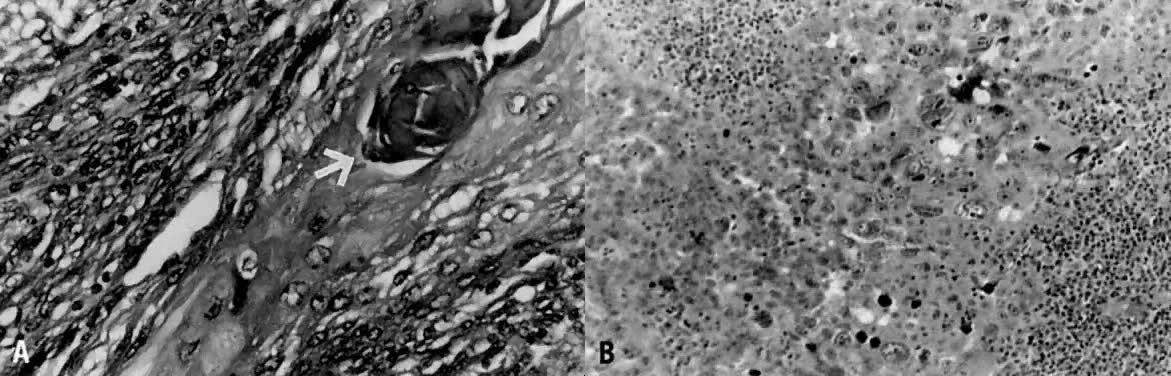
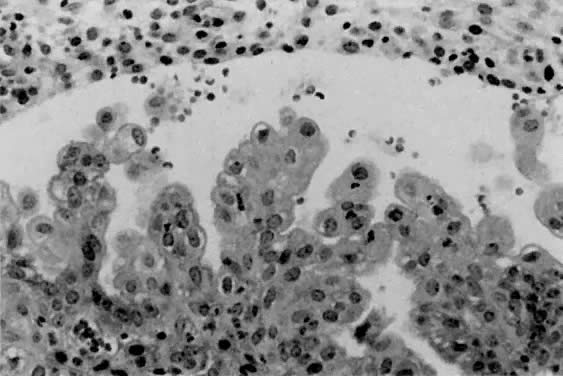
for it to be considered a distinct entity. Villoglandular (Papillary) Adenocarcinoma Villoglandular carcinoma is characterized by a papillary architecture with
delicate fibrovascular stalks lined by cuboidal to columnar cells
with minimal cellular stratification and mild nuclear pleomorphism (Fig. 5). Nucleoli are indistinct. It is important to distinguish this well-differentiated
papillary variant of endometrial carcinoma from serous carcinoma, which
is often papillary but displays grade 3 nuclear atypia
with vesicular nuclei, prominent nucleoli, and necrosis.21,29 Serous carcinoma often forms papillary tufts, small clusters of cells
that are detached from the papillary fronds. Psammoma bodies may be observed
in either tumor type27 and are therefore not reliable distinguishing features. Villoglandular
carcinoma only superficially invades the myometrium, being diagnosed
at an early stage and thereby having a better prognosis than typical endometrioid
carcinoma. To avoid confusion with papillary serous carcinoma, some
authors refer to this entity as endometrioid adenocarcinoma
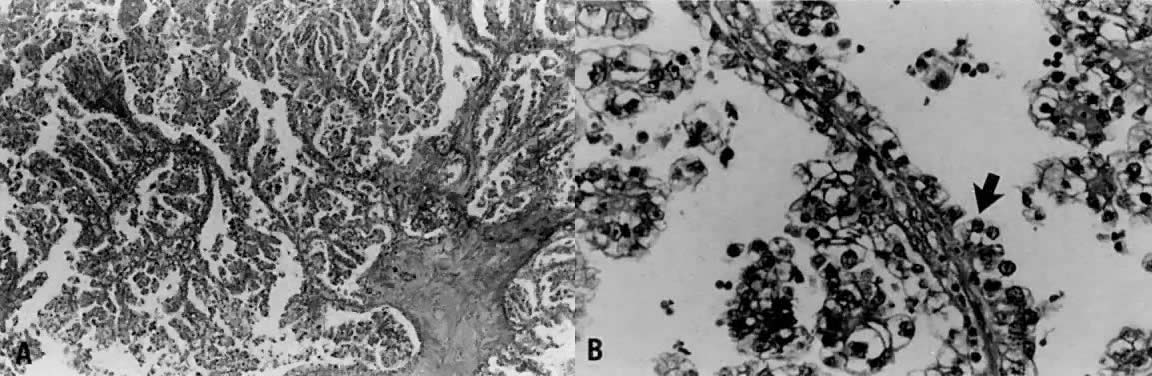
with papillary architecture. 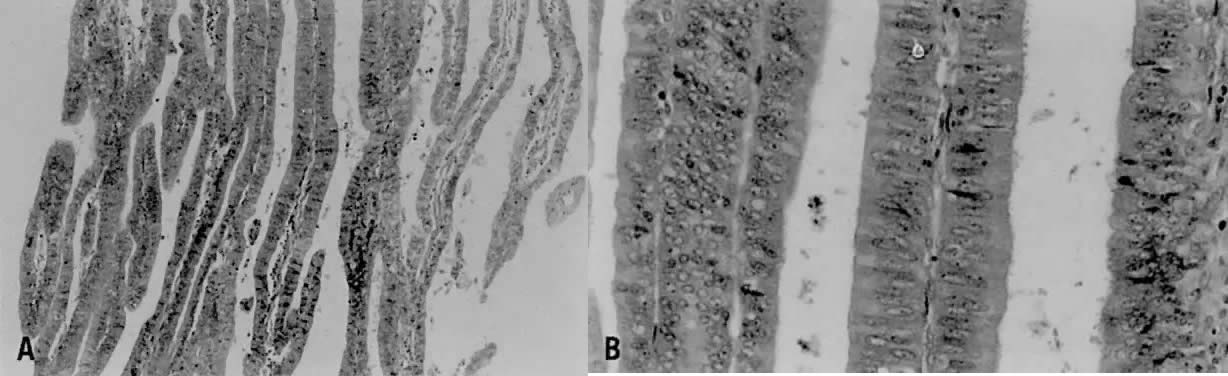 Fig. 5. ( A) Long papillary stalks lined by endometrioid-type cells are characteristic
of the villoglandular or papillary variant of endometrial adenocarcinoma. ( B) The papillae are lined by stratified cells demonstrating mild nuclear
atypia. Cellular budding and high-grade nuclear features are absent, aiding
in distinguishing this lesion from serous carcinoma. Fig. 5. ( A) Long papillary stalks lined by endometrioid-type cells are characteristic
of the villoglandular or papillary variant of endometrial adenocarcinoma. ( B) The papillae are lined by stratified cells demonstrating mild nuclear
atypia. Cellular budding and high-grade nuclear features are absent, aiding
in distinguishing this lesion from serous carcinoma.
|
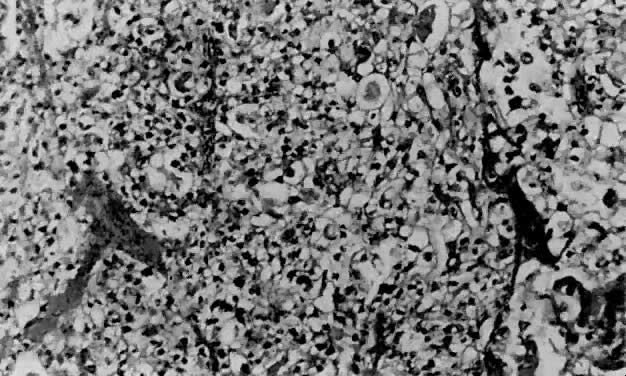
Secretory Carcinoma Less than 1% of endometrial adenocarcinomas are classified as secretory
carcinomas.20 The well-differentiated glands of this variant appear histologically similar
to secretory phase endometrium (postovulatory days 3 to 6), with
abundantly vacuolated columnar cytoplasm, either subnuclear or supranuclear20,30,31,32,33,34,35 (Fig. 6). Cellular atypia is minimal. Squamous and tubal metaplasia frequently
accompany this cell type.20 The adjacent nonmalignant endometrium typically shows changes consistent
with prolonged or unopposed estrogen effect (e.g., hyperplasia, stromal breakdown, and thrombosis of vessels). The excellent
prognosis seen in these patients is due to the fact that most have
surgical stage I disease, and invariably the neoplasm is of low grade
both architecturally and cytologically. Distinction from clear cell
carcinoma is important due to the marked differences in prognosis. Although
both types have intracytoplasmic glycogen, secretory carcinoma does
not demonstrate papillary or cystic architecture, nor does it show
grade 3 nuclear atypia or the hobnail pattern commonly seen in clear
cell carcinoma. Separation of secretory carcinoma from secretory changes
in atypical hyperplasia is based on the presence of stromal invasion
and back-to-back glands found in carcinoma. 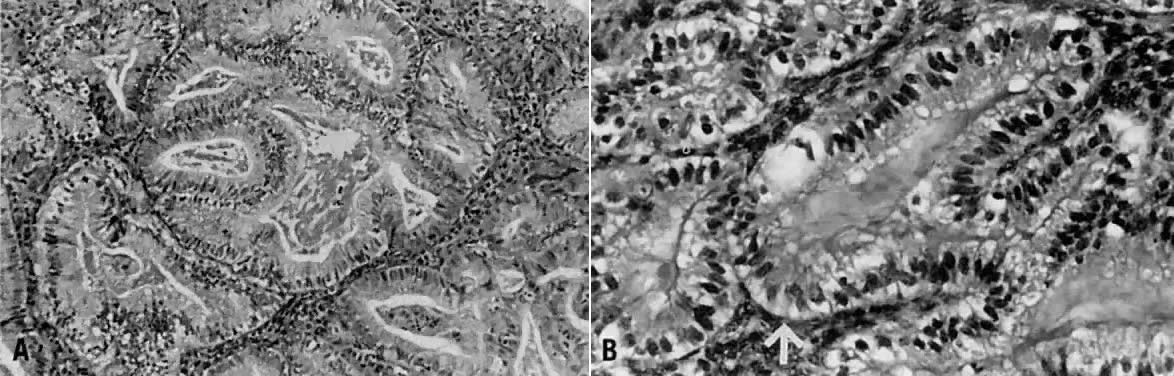 Fig. 6. ( A) Secretory carcinoma is characterized by prominent cytoplasmic vacuoles
and intraluminal secretions. ( B) The arrow denotes the uniform subnuclear vacuoles. Fig. 6. ( A) Secretory carcinoma is characterized by prominent cytoplasmic vacuoles
and intraluminal secretions. ( B) The arrow denotes the uniform subnuclear vacuoles.
|
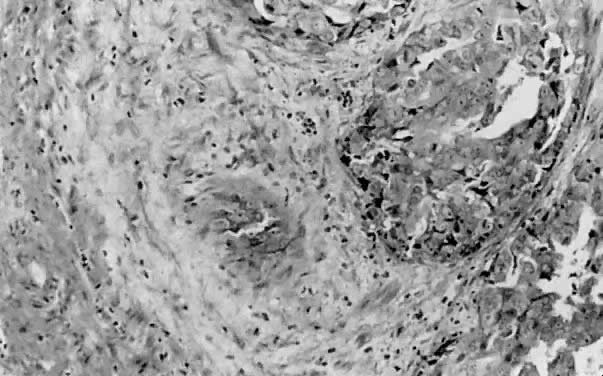
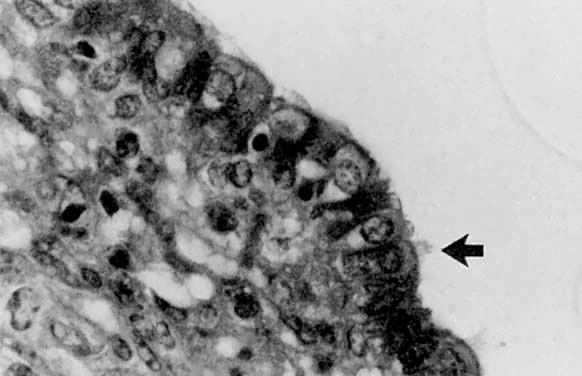
Ciliated Cell Carcinoma The ciliated cell variant of endometrial carcinoma is exceedingly rare, with
only a few reported cases in the literature. Although most endometrial
lesions with ciliated cells represent metaplasia, it is important
to be cognizant of this subtype, which meets the architectural criteria
for carcinoma, usually in the form of cribriforming. Ciliated cell
carcinoma is well differentiated and consists of glands lined predominately
by ciliated cells with abundant eosinophilic cytoplasm (Fig. 7). There is usually minimal nuclear atypia, with mildly irregular nuclear
contours and prominent nucleoli. Association with exogenous estrogen
use is typical,36 correlating with the observation that normal endometrium forms cilia with
estrogen stimulation. Thus far, no reports of recurrence or death
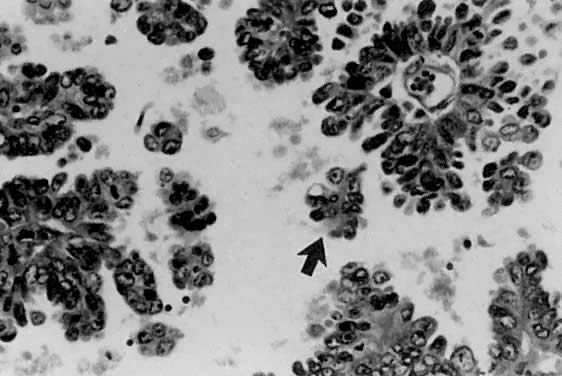
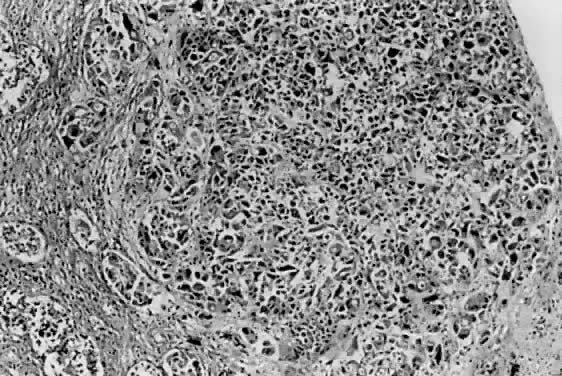
due to disease have been described. 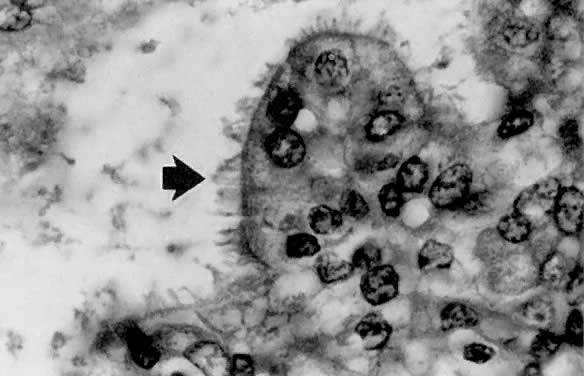 Fig. 7. Ciliated cell carcinoma. Most of the neoplastic glands are lined by ciliated
cells ( arrow) showing mild to moderate nuclear atypia. Fig. 7. Ciliated cell carcinoma. Most of the neoplastic glands are lined by ciliated
cells ( arrow) showing mild to moderate nuclear atypia.
|
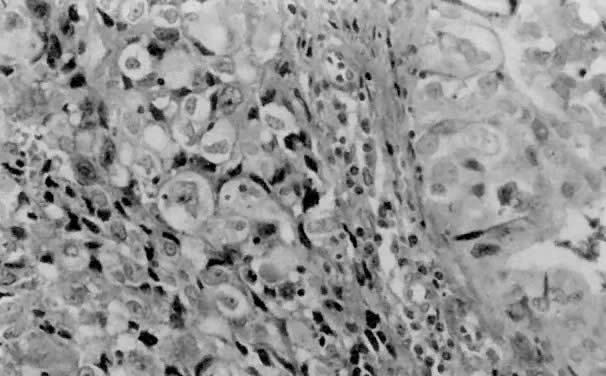
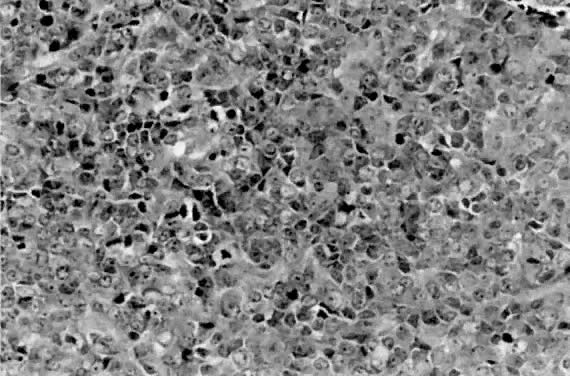
Endometrioid Adenocarcinoma With Squamous Differentiation Squamous differentiation in endometrial carcinoma (Fig. 8) is a frequent finding, noted in about 25% of cases.37,38,39,40,41 To be classified as such, 5% or greater of the carcinoma must exhibit
one or more of the following patterns: keratin pearl formation, defined
intercellular bridges, or morules consisting of ovoid or spindled (glassy) cells.8,37 Although the occurrence of squamous differentiation in endometrial carcinoma
is well accepted, its significance has proven to be quite controversial. Until
recently, most have divided endometrial carcinomas with
squamous differentiation into two categories. Adenoacanthoma38,39,40 was a term previously used to describe lesions that had a benign squamous
component accompanying the invasive adenocarcinoma. Adenosquamous
carcinoma was reserved for adenocarcinomas that also had obvious malignant
squamous features. Silverberg38 defined criteria for distinguishing between adenoacanthoma and adenocarcinoma, proposing
that the presence of malignant squamous elements imparts
a worse prognosis. However, the current terminology used by the
GOG is adenocarcinoma with squamous differentiation, making no distinction
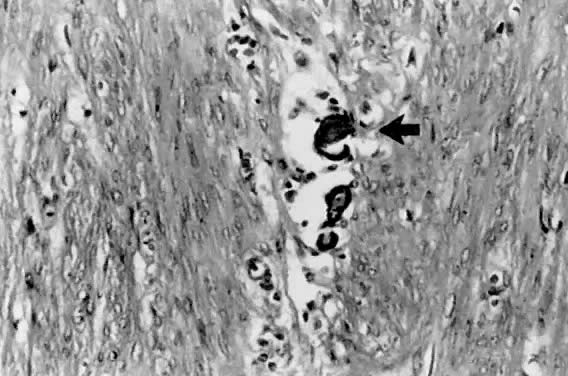
as to the degree of differentiation of the squamous component. 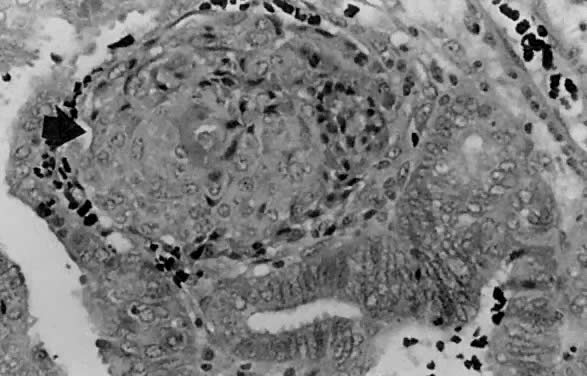 Fig. 8. Squamous differentiation in endometrial adenocarcinoma is frequent. This
is an example of a squamous morule ( arrow ), which is a collection of polygonal cells with abundant eosinophilic
cytoplasm forming a nodular structure between neoplastic endometrial
glands. Fig. 8. Squamous differentiation in endometrial adenocarcinoma is frequent. This
is an example of a squamous morule ( arrow ), which is a collection of polygonal cells with abundant eosinophilic
cytoplasm forming a nodular structure between neoplastic endometrial
glands.
|
A study by Zaino and associates37 based on 600 women with stage 1 or 2 disease addressed this issue. They
found that histologic grade and depth of myometrial invasion more accurately
predicted which patients were at risk for developing nodal metastases
than did designating tumors as adenoacanthoma or adenosquamous
carcinoma. There was no statistically significant difference in the
occurrence of lymph node metastasis between the two types. Another important
finding confirmed by this study was that the differentiation of
the squamous component parallels the degree of glandular differentiation
in the vast majority of cases. In other words, frank malignant features
present within the squamous component are observed in high-grade
adenocarcinomas24,37 as determined by the glandular portion. Therefore, the observation that “adenosquamous
carcinomas” had a worse prognosis was essentially
correct. Although the biologic behavior of adenocarcinomas with
squamous differentiation is similar to that of adenocarcinomas lacking
this component, the presence of squamous elements is associated with
an increased probability of survival.37,41 Mucinous Carcinoma Mucinous carcinoma is typically of low grade and is the least common type
of endometrial adenocarcinoma. Intracytoplasmic mucin must be present
for a neoplasm to be placed in this category.8 Although polypoid lesions are more commonly identified in this type of
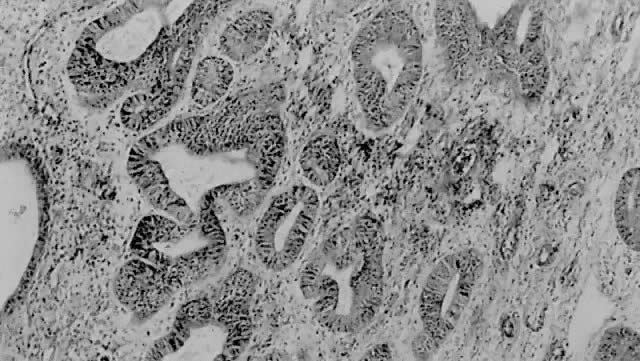
carcinoma,42 other macroscopic features are similar to typical endometrial carcinoma. Histologically, the
neoplastic glands, often forming papillary structures, are
lined by mucin-secreting columnar cells resembling either
endocervical (Fig. 9) or gastrointestinal epithelium. Often present are cystically dilated
glands with abundant intraluminal mucin. The nuclei generally demonstrate
only mild atypia, and mitoses are uncommon. 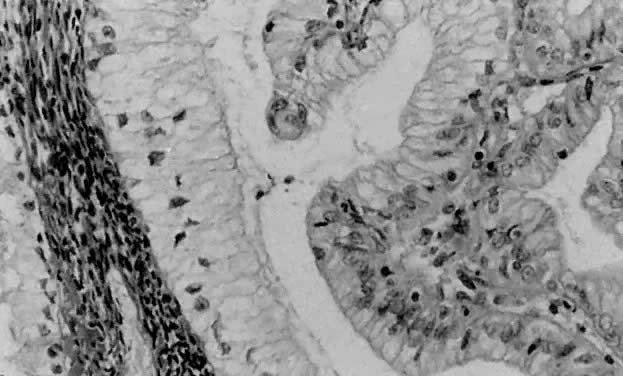 Fig. 9. Mucinous carcinoma is generally well differentiated and is characterized
by columnar cells with basally located nuclei and mucin-rich cytoplasm. Fig. 9. Mucinous carcinoma is generally well differentiated and is characterized
by columnar cells with basally located nuclei and mucin-rich cytoplasm.
|
On rare occasions, one encounters an endometrial lesion that appears histologically
similar to microglandular hyperplasia of the cervix.43,44 This distinctive pattern consists of small glands (microcysts) lined by
flattened cuboidal cells with mild nuclear atypia. Groups of polygonal
cells with eosinophilic cytoplasm are present between the glands. Abundant
amounts of inflammation in the form of neutrophils are present
within the luminal spaces and among the epithelial cells. When this pattern
is observed, it is important to exclude microglandular hyperplasia
of the cervix, especially if the diagnosis is made on a curettage
specimen. |