Endometriosis
Authors
INTRODUCTION
The reproductive-age woman with endometriosis poses a challenging and frequently frustrating clinical problem for the gynecologist. Since the description of endometriosis by John Sampson in 1921,1 numerous studies have failed to produce a consensus regarding the pathogenesis, mechanism of morbidity, and management of this condition. The complexity of this disease and the shortcomings in our knowledge base conspire to make our approach to the patient more difficult. Endometriosis is typically located in, but not limited to, the pelvis, where it can disrupt the anatomic, hormonal, and immunologic environment. These alterations are responsible for the varied clinical presentations. Treatment objectives are to restore normal anatomy, remove or ablate endometrial implants, and prevent or delay disease recurrence. Although endometriosis is not considered a life-threatening disease, it is a life-altering disease that requires timely diagnosis and treatment to minimize the clinical sequelae.
DEFINITION
Endometriosis is defined as a pathologic condition in which the endometrium, consisting of endometrial glands and stroma, is found in locations outside the endometrial cavity and uterine musculature. The usual location of endometriosis is in the pelvis. However, endometriosis has been described in extrapelvic sites, including anterior abdominal wall, surgical scars, diaphragm, omentum, small intestine, appendix, lung, urinary tract, musculoskeletal, and neural systems.2, 3, 4, 5, 6, 7 An area of endometriosis that is large enough to be described as a tumor is called an endometrioma.8 These areas typically occur as cystic lesions on the ovary.
PREVALENCE AND EPIDEMIOLOGY
The prevalence of endometriosis in the general population has been difficult to determine primarily because of the selection bias of the populations used to make this estimate. Because the definitive diagnosis of endometriosis is surgical, the observed prevalence may be biased by the selection of patients for surgery and by which patients elect to proceed with surgery. Moreover, endometriosis is present in some women who are asymptomatic and do not have surgery. The observed prevalence may also depend on the skill and experience of the surgeon in identifying endometriosis.
The population of women being studied has a significant effect on the prevalence estimates of endometriosis. The estimates range from 1–50%, depending on the surgical series.2 A population of symptomatic women undergoing surgery has a higher prevalence estimate than the general population. In contrast, asymptomatic women undergoing tubal ligations probably have a lower prevalence estimate. In a compilation of several studies categorized by indication for surgery, the prevalence of endometriosis in women with pelvic pain was 24.5%, compared with 19.6% in women with infertility.3 In women undergoing tubal ligation, the prevalence of endometriosis was 4.1%.
In large studies reviewing hospital discharge or surgical records, estimates of the prevalence of endometriosis have varied from 6 to 11% of reproductive-age women.4, 5, 6 Because of the medical, social, and cultural influences on the selection of patients for surgery, attempts have been made to estimate the prevalence of endometriosis in the general population. In one such study, the study population was extended to include surgical patients and women with symptoms and physical findings on examination suggestive of endometriosis.7 The overall incidence of pelvic endometriosis ranged from 108.8 to 246.9 cases per 100,000 person-years, depending on how many diagnostic categories were used. Assuming an average duration of endometriosis of 10 years, the investigators concluded that the prevalence in the population would have been 2.5 and 3.3%. A reasonable assumption of the average duration of endometriosis from diagnosis until menopause is 25 years, which would increase the prevalence to 6.2–8.2%.
Endometriosis is a disease of reproductive-age women. The typical age at diagnosis is between 25 and 29 years,8 but endometriosis occurring in premenarchal girls and postmenopausal women has been reported.9, 10, 11 Among adolescents, the occurrence of endometriosis is not uncommon. A disproportionate number of adolescents with endometriosis have associated müllerian anomalies and outflow tract obstruction.12, 13
Attempts by several studies have been made to identify the risk factors for the development of endometriosis.3 The various factors that have been examined include age, race, socioeconomic status, marital status, education, contraceptive use, menstrual cycle characteristics, reproductive history, physical characteristics, and personal habits. Results from these studies have been inconsistent with respect to the significance of the risk factor examined. This inconsistency probably stems from differences in the population groups used, differences in the criteria for diagnosis, lack of a well-defined comparison group in some studies, or not controlling for potential confounding variables.
Among the demographic factors, only age had a consistent relationship. In general, increasing age correlated positively with endometriosis.14, 15 A racial tendency for higher rates of endometriosis in white women originally was believed to exist.16 The differences observed, however, were caused by socioeconomic factors such as access to health care and contraception. When these confounding variables are controlled, similar rates of endometriosis are observed among women of different races.17, 18, 19 In women affected by endometriosis, an increased frequency of certain personality traits (e.g. intelligent, perfectionist, overachiever, anxious) has been reported, presumably because of the assumption that women with these traits are more likely to delay marriage and childbearing. These observations, however, have not been validated.20 Other factors that may affect the risk of endometriosis relate to menstrual characteristics. In three case-control studies, greater exposure to menstruation because of longer flows, shorter cycles, or lower parity appears to increase the risk of endometriosis.21, 22, 23 Greater peripheral body fat is associated with a greater risk of endometriosis, possibly because of elevated endogenous estrogen levels.24 Direct measurement of body fat, however, was not determined. This hypothesis is also inconsistent with the observation that anovulatory women with persistently elevated estrogen levels do not have a higher reported incidence of endometriosis. Factors such as smoking that reduce endogenous estrogen levels may have an inverse association with the risk of endometriosis.21, 22 Other studies have reported no association between smoking and endometriosis.14, 15 The data are inconclusive regarding the association of lifestyle factors and physical characteristics with endometriosis.
The use of oral contraceptives appears to reduce the risk of endometriosis in current or recent users.14, 15 In another study, however, no association with current oral contraceptive use and endometriosis risk was observed.25 All three studies did not find an association between duration of oral contraceptive use and endometriosis.
A genetic susceptibility for endometriosis appears probable in light of the familial tendency that has been described in several studies. Early reports of familial clustering suggested a possible genetic basis for endometriosis.19, 26, 27, 28 Stronger evidence for a genetic basis is seen in two small studies of monozygotic twins. Concordance for endometriosis was found in 6 of 8 twins in one study29 and 14 of 16 twins in the other.30 Perhaps the strongest evidence in support of the involvement of genetic factors is the increased prevalence of endometriosis among relatives compared with the general population.31, 32, 33 The risk of endometriosis was increased sixfold to sevenfold for relatives of an affected person compared with controls, which is similar to that seen for other multifactorial diseases. The Oxford Endometriosis Gene (OXEGENE) study, a worldwide collaborative project, is studying affected sib pairs with linkage analysis and attempting to identify susceptibility loci and genes for endometriosis.
PATHOGENESIS
Since the first description of endometriosis more than a century ago, several theories have been advanced to explain the histogenesis of endometriosis. The extensive investigative effort of basic and clinical researchers, however, has yet to clearly define the mechanism responsible for the development of endometriosis. Current research has focused on alterations in the immune response and other regulatory factors that could mediate the histogenesis of endometriosis.
The theories of histogenesis can be categorized according to three predominant mechanisms: transplantation, celomic metaplasia, and induction (Table 1). In addition to these theories, others have been put forth to explain the histogenesis of endometriosis such as embryonic cell rests that are activated to form endometriosis,34, 35 direct extension of endometrium through the uterine wall,36 and uterotubal extension.37 These mechanisms may explain some cases of endometriosis but are unlikely to be the major cause.
Table 1. Histogenesis theories of endometriosis
Transplantation
Retrograde menstruation
Hematogenous dissemination
Lymphatic dissemination
Iatrogenic
Celomic metaplasia
Induction
Combination of transplantation and metaplasia
Embryonic cell rests
Direct extension
Uterotubal extension
Transplantation
The theory of transplantation was proposed in a series of publications by Sampson,1, 38, 39 who hypothesized that endometriosis was the result of viable endometrial tissue from the uterus that could be transported to ectopic sites where it would implant and grow. These implants then could become additional foci for further spread. The primary mechanism of transport is retrograde menstruation of endometrial cells through the fallopian tubes into the peritoneal cavity. Several studies have confirmed the occurrence of retrograde menstruation and have shown it to be a common phenomenon (76–90% of women).40, 41, 42, 43
Although retrograde menstruation is an explanation for the most frequent forms of endometriosis in the pelvis, it does not account for the unusual finding of implants in the pelvic lymph nodes or other sites outside of the pelvis such as lung, nose, vertebral space, extremities, kidney, and umbilicus. Dissemination of endometrial cells through the lymphatic44, 45, 46 and vascular46, 47, 48 system has been demonstrated and has been used to explain the presence of endometriosis at these various locations. Given the usual anatomic distribution of endometriosis, however, these routes of endometrial cell dissemination are not thought to be common.
The iatrogenic introduction of endometrium to ectopic sites by mechanical transplantation has been suggested as another mechanism of endometriosis development. Findings of endometriosis in episiotomy and laparotomy scars after gynecologic procedures support this theory.49, 50 The viability of surgically transplanted endometrium has been demonstrated in animals and humans.51, 52 In women undergoing hysterectomy, cyclic bleeding occurred from excised endometrium that was intentionally implanted at the vaginal apex for psychologic reasons. The iatrogenic transplantation of endometrial tissue cannot account for most women with endometriosis.
For retrograde menstruation to be considered the major mechanism for the histogenesis of endometriosis, endometrial cells in the menstrual effluent must be viable and capable of implantation. Early evidence of viability was demonstrated by supravital staining of endometrial cells in the menstrual flow40 and by in vitro growth of menstrual endometrium.53 In an experiment to determine the viability of discharged endometrial tissue, menstrual effluent from the second day of menstruation was injected into subcutaneous abdominal fat. After 90–180 days, the injection site was excised for histologic examination and found to have endometriosis.54 In another experiment using a monkey model, extensive endometriosis developed in the peritoneal cavity in one half of the monkeys after diversion of menstruation into the peritoneal cavity.55
Other observations providing circumstantial evidence in support of retrograde menstruation include the anatomic distribution of endometriosis. The most frequent sites of implantation are the dependent areas of the pelvis (i.e. ovary, posterior and anterior cul-de-sac, and uterosacral ligaments), which are most likely to be affected by menstrual reflux from the fallopian tubes.56 In women with obstructions to the normal outflow of menstrual fluid, a higher incidence of endometriosis is observed.12, 57
Celomic Metaplasia
One of the first theories of histogenesis proposed by Robert Meyer was the celomic metaplasia theory, which asserts that endometriosis is derived from metaplasia of cells lining the pelvic peritoneum. The basis of this theory is the observation from embryologic studies that peritoneal mesothelium, the müllerian ducts, and the germinal epithelium of the ovary are all derived from celomic wall epithelium.58 The assumption is that these tissues retain the capacity for further differentiation or that the peritoneal mesothelium and germinal epithelium contain undifferentiated cells capable of developing into functioning endometrium. Celomic epithelium can be found in the thoracic cavity, umbilicus, and limb buds, which can explain the occurrence of endometriosis in these unusual ectopic sites. However, experimental proof that differentiated peritoneal cells can undergo further differentiation to produce endometriosis spontaneously or by being induced is lacking.
Clinical observations have cast further doubt on the validity of this theory. Endometriosis would be expected to occur in males as well as females if peritoneal epithelium could undergo metaplasia. The occurrence of endometriosis in males, however, has been reported in only a few cases of men receiving high-dose estrogen therapy for prostatic carcinoma.59, 60, 61 Despite the contribution of celomic tissue to the development of peritoneum and pleura, endometriosis is located primarily in the pelvis and not uniformly distributed in other sites where the celomic membrane is present. In light of these observations and the lack of experimental evidence supporting the de novo formation of endometriosis by metaplasia, this theory is unlikely to be an explanation for the histogenesis of endometriosis in most women.
Induction
The induction theory of endometriosis is a combination of the transplantation and celomic metaplasia theories. This theory proposes that specific agents released from shed endometrium induce undifferentiated mesenchyme to develop into endometriosis. The results of studies using rabbits have supported this theory. In one study, fresh and denatured endometrium was implanted into the subcutaneous tissue of female rabbits.62 After 7 days, the fresh and denatured endometrium resulted in cyst formation and differentiation characteristic of endometrium. A more pronounced tissue reaction with denatured endometrium and the absence of stromal cells in the cysts were observed. In another study, Millipore filters containing endometrium, myometrium, or fat were implanted into rabbits.63 The tissue surrounding the diffusion chambers containing endometrium were excised and found to have cysts lined with cells resembling endometrial epithelium and endometrium-like glands. This finding was not observed in the tissue surrounding the myometrium or fat chambers. None of the histologic sections of surrounding tissue contained endometrial stroma. Further evidence supporting this theory in nonhuman primates and women has yet to be obtained.
Embryonic Cell Rests
The embryonic cell rests theory suggests that functioning endometrium can be formed by the activation of cell rests. These rests of müllerian origin, which are common in the ovary, would be induced to form endometriosis under the appropriate stimulus. The development of endometriosis from cell rests, however, has not been demonstrated.
Direct Extension
The direct extension theory proposes that endometriosis arises from the invasion of endometrium through the uterine musculature. This theory was based on the observation that glandular structures of adenomyosis were in direct contact with eutopic endometrium.36 No conclusive evidence of the progression of endometrial invasion through the myometrium into the pelvis to present as endometriotic implants has been reported.
Uterotubal Extension
The theory of uterotubal extension is a combination of the direct extension and transplantation theories, which suggests that endometriosis is a consequence of direct extension through the tubal wall. A few studies have reported the presence of tubal endometriosis but did not determine whether ectopic endometrial implants were contiguous.64, 65 Although this mechanism is plausible, most cases of endometriosis are unlikely to be a result of endometrial extension through the tubal wall.
Immunologic Factors
The occurrence of retrograde menstruation has been demonstrated to be a near universal phenomenon consistent with the transplantation and induction theories of endometriosis. In women who develop endometriosis, the endometrial cells appear to have a tendency to adhere and grow outside of the uterus.66 The difference in the observed prevalence of endometriosis and the occurrence of retrograde menstruation are probably caused by additional factors that are responsible for the variable development and expression of endometriosis after initiation of the implants. The immune response has been suggested as one of the factors that is involved with the attachment or clearance of refluxed endometrial tissue fragments.67 Alterations in the immune response may prevent adequate disposal of menstrual debris, possibly increasing the chances of endometriosis development. The nature and degree of impairment could account for the variable presentation of endometriosis. Alternatively, excessive menstrual reflux may overwhelm the capacity of an intact immune system to remove endometrial tissue or suppress its growth.
Several studies have suggested an association between endometriosis and alterations in cell-mediated and humoral immunity. It is unclear, however, whether abnormalities in the immune response are a causative factor for endometriosis or endometriosis induces the observed abnormalities in the immune response. In general, the primary alterations observed are decreased natural killer (NK) cell and T-lymphocyte activity, increased circulating auto-antibodies, and increased peritoneal macrophage numbers and activity.
CELL-MEDIATED IMMUNITY.
Impairment of the cell-mediated immune response is thought to have a permissive effect on the implantation of refluxed endometrial cells, thereby increasing the chance of endometriosis development. This impairment may be mediated by decreased NK cell activity in peripheral blood mononuclear cells.68, 69 NK cells are large granular lymphocytes that are cytotoxic to cells with an undefined target molecule and cells coated with antibody. Assuming NK cells target endometrial cells, abnormal NK cell function may result in inadequate clearance of refluxed endometrium from the peritoneal cavity.70
In women with endometriosis, the observed decrease in NK activity appears to be a qualitative defect rather than a result of reduced numbers.68 The decrease in NK activity has been reported to correlate with increasing estradiol concentrations.71, 72 In contrast, women with advanced endometriosis treated with gonadotropin-releasing hormone (GnRH) agonists had an increase in NK-cell activity in peripheral blood mononuclear cells.73 The cause of reduced NK activity is unknown. Increased concentrations of transforming growth factor-β (TGF-β), IL-1, and tumor necrosis factor-α (TNF-α) in the peritoneal fluid of women with endometriosis have been reported.74, 75, 76 TGF-β, however, inhibits NK activity, whereas IL-1 and TNF-α are expected to increase NK activity.
Despite several studies reporting abnormal NK-cell activity in women with endometriosis, the clinical relevance of these results in relation to the development of endometriosis has been challenged.70 In the baboon model for endometriosis, no differences in NK-cell activity or lymphocyte-mediated cytotoxicity were observed between baboons with and without endometriosis.77 Moreover, immunosuppressed baboons with and without endometriosis did not have progression or development of endometriosis.78 More conclusive data are required to attribute a role to NK-cell activity in the development of endometriosis.
The possibility of a regulatory role for T cells in the development of endometriosis has been suggested.79 In women with mild endometriosis, quantification of T-cell subsets revealed a decrease in suppressor T-cell activity. In women with severe endometriosis, the decrease in suppressor T-cell activity was accompanied by an increase in helper T-cell activity. These changes in the regulatory T cells were suspected to have a role in the transition from mild to severe endometriosis. Other conflicting results, however, show no change in the total number of peripheral lymphocytes or the percentage of T-cell subsets.80 When interpreting the results of these functional studies using peripheral lymphocytes, consideration must be given to the possibility that the biologic activity of peripheral lymphocytes may differ from the activity of lymphocytes in other tissue sites.81 Other reported alterations in T-cell function include defects in T-cell-mediated cytotoxicity in women with endometriosis.67, 82 As shown in baboon studies, however, lymphocyte-mediated cytotoxicity was not altered whether endometriosis was present or absent. It is premature to conclude that altered T-cell responses in women with endometriosis are a causative factor until more rigorous data from well-designed human studies are available.
HUMORAL IMMUNITY.
Abnormalities in B-cell function and a high incidence of abnormal autoantibodies in women with endometriosis have been reported in several studies. Antibodies to endometrial tissue may facilitate the growth of endometriosis by blocking the recognition sites required for T-cell-mediated destruction. Despite the detection of high levels of anti-endometrial antibodies in sera, peritoneal fluid, and endometrial tissue of women with endometriosis, no correlation between antibody titers and disease severity was observed.83 The suggestion of endometriosis as an autoimmune disease or part of a more generalized autoimmune syndrome has yet to be proved.
PERITONEAL FACTORS.
In the pelvic cavity, macrophages are the predominant cell type among desquamated mesothelium and lymphocytes.84, 85 Macrophages are thought to have a major role in the local immune process. In addition to removing red blood cells, tissue debris, and possibly endometrial cells, macrophages may contribute to the development of endometriosis by secreting cytokines and growth factors. The total number, concentration, and activational status of peritoneal macrophages are increased in women with endometriosis.86, 87 Similarly, an increase has been observed in the production of TGF-β,74 macrophage-derived growth factor,88 vascular endothelial growth factor,89 interleukin-1,75 interleukin-6,90 interleukin-8,91, 92 TNF-α,93 monocyte chemoattractant protein-1,94 growth-regulated α,95 and RANTES (“regulated on activation, normally T-cell expressed and secreted”).96
The interaction of cytokines, growth factors, and angiogenic factors may be responsible for the maintenance, cellular differentiation, and growth of endometriosis implants in the pelvis. Peritoneal fluid from women with endometriosis was shown to enhance the proliferation of endometrial stromal cells in culture97 and to contain angiogenic activity.98 Epidermal growth factor, insulin-like growth factor I, growth hormone, platelet-derived growth factor, and macrophage-derived growth factor also stimulate endometrial stromal cell proliferation in vitro.99, 100, 101 Although substantial data exist to support the role of these various peritoneal factors in the development of endometriosis, it is still unclear whether the changes observed precede or follow the onset of endometriosis.
Endometriotic Disease Theory
A concept called the endometriotic disease theory has been proposed to explain the variable growth, development, and expression of endometriosis lesions.102 The development of endometriosis is considered to be similar to the onset and growth of a benign tumor, with the primary focus on cellular changes or mutations that cause altered behavior. According to this theory, these cellular changes occur more frequently in genetically predisposed individuals and in individuals who are exposed to other factors such as total-body irradiation or chemical pollutants that can cause mutations. The highly variable expression of endometriosis primarily reflects the differences in genomic mutations. The type and severity of lesions that develop are influenced also by the peritoneal fluid, which is important for local modulation of growth, and possibly by tumor mechanisms such as extracellular matrix breakdown, critical mass, and local shielding from immunologic attack.103 The endometriotic disease theory provides an explanation for the various manifestations of endometriosis. As more data are accumulated, the validity of this theory will be better determined.
Other Factors
In an attempt to explain why the growth of endometriosis occurs in some women but not others, investigators have examined the role of cell adhesion molecules and their extracellular matrix ligands in the attachment and invasion of endometriotic cells.104 It is suspected that modulation of adhesion molecules or their ligands may be responsible for the observed alterations in cellular behavior of the endometriosis implants.105 Studies have shown the presence of cell adhesion molecules on implants and suggest a possible role in the development of endometriosis. In this relatively nascent field of investigation, the extent of the contribution to the cause of endometriosis and the interaction with other modulating factors has yet to be determined.
The role of environmental toxins in stimulating endometriosis development is another area of increasing interest.106 In particular, dioxin and dioxin-like compounds, which have several biologic effects, are suspected to contribute to the genesis of endometriosis. In rhesus monkeys, rats, and mice, a positive correlation between dioxin exposure and the development of endometriosis was demonstrated.107, 108 The effects of dioxin on endometriosis, however, are heterogeneous, depending on the species and experimental model used. The reliability of animal data to predict outcomes in humans is uncertain. More research is required to determine the effects of dioxin on endometriosis development in humans.
PATHOLOGY
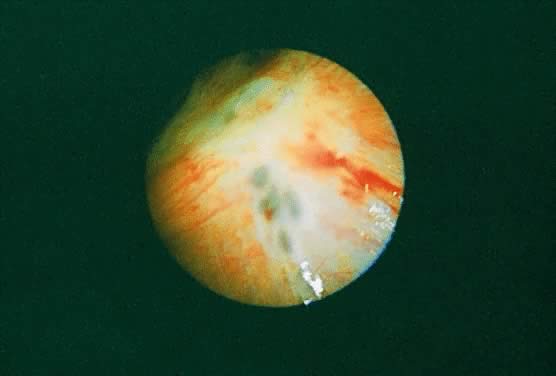
The gross appearance of endometriotic implants typically has been described as bluish gray, dark brown, or black “powder burn” lesions (Fig. 1). The color is attributed to hemolyzed blood from ectopic endometrium that is encapsulated by adhesions or fibrotic tissue. These peritoneal surface lesions usually range in size from a few millimeters to 2 cm in diameter and often are surrounded by various degrees of fibrosis that may confer a puckered appearance. Endometriosis implants may vary considerably in appearance. Smaller fresh lesions may be found as clusters of nodules resembling hemorrhagic vesicles, which have been described as “raspberry” spots (Fig. 2). Other implants may appear as clear, nonpigmented, or slightly brown vesicles, reddish polyps, white scar tissue or plaques, petechiae, or flamelike lesions. In the natural evolution of endometriosis, white, scarred peritoneum or the typical pigmented lesion is considered a late-stage manifestation of endometriosis. All types of implants may coexist within the same patient. Occasionally, foci of endometriosis may be found at the base of adhesions formed in response to chronic peritoneal surface irritation by the implants. Peritoneal pockets may also be associated with endometriosis.109 Two-thirds of these pockets have been reported to contain endometriosis around the rim or inside the defect.110 Occasionally, subtle endometriosis lesions can be missed even by experienced laparoscopists.111
|
|

Diffuse infiltration of the broad ligament may occur in some patients. Endometriosis and red adhesions may involve the entire area from the uterosacral ligaments to the ovary and fallopian tube. Black and red areas of disease, sometimes associated with scarring, are usually readily apparent.
Endometriosis implants may infiltrate subserosally and become deeply invasive and nodular. This invasion usually results in a reactive inflammatory response and fibrosis in surrounding tissues, resulting in the development of more extensive and dense adhesions over time. Complete cul-de-sac obliteration can eventually result from longstanding invasive and adhesive disease. Nodular induration that is typically discovered during pelvic examination may also occur.
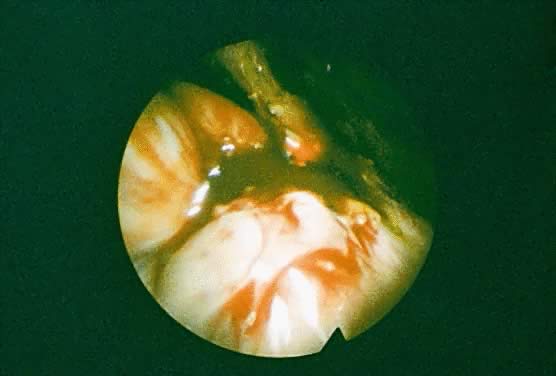
Endometriotic cysts typically are encountered in the ovary. Superficial ovarian implants are usually found on the lateral and inferior surfaces of the ovary and occur as irregular, variously pigmented lesions. After a cyst forms, cyclic hemorrhage within the cyst adds to the contents, causing cyst growth because of the slow reabsorption of debris. These endometriomas have been described as chocolate cysts because of the thick, tarry, dark brown fluid composed of blood and blood pigment that fills these cysts (Fig. 3). As intracystic pressure increases, the tendency for endometriomas is to perforate. This permits leakage of the highly irritating cyst contents that precipitates dense adhesion formation to adjacent organs. The site of perforation is typically involved in the adhesive process, rendering surgical removal of the cyst more difficult.
|
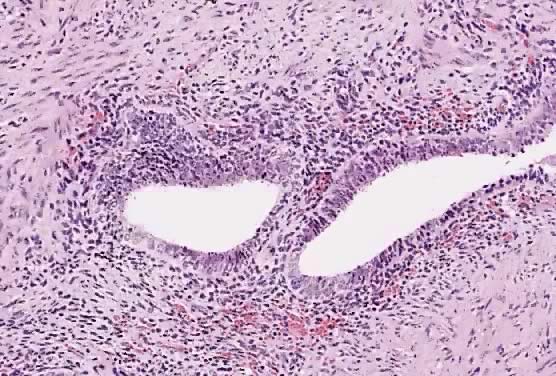
The microscopic appearance of endometriosis consists of endometrial glands, endometrial stroma, fibrosis, and hemorrhage (Fig. 4). Ideally, at least two of these components should be present to classify a lesion as endometriosis. Endometriosis implants are thought to respond to the cyclic hormonal changes during the menstrual cycle with corresponding cyclic histologic changes in synchrony with the endometrium. Most implants, however, do not exhibit the typical cyclic histology seen in normal endometrium.112 In endometriomas, the cyst wall is often lined with fibrous tissue and varies in thickness. The wall contains simple cuboidal epithelium with little evidence of menstrual cyclicity. Hemorrhage into surrounding tissue may result in a zone of hemosiderin-laden macrophages or pseudoxanthoma cells in addition to fibrosis. Often, histologic confirmation of endometriosis is not achieved after surgical excision. In some cases, this is the result of a loss of histologic detail from repetitive intraluminal hemorrhages. A presumptive diagnosis can be made based on the gross findings in combination with hemosiderin-laden macrophages and fibrous tissue around a hemorrhagic cyst.
|
CLINICAL PRESENTATION
Endometriosis can cause a wide variety of symptoms, none of which are pathognomonic for the disease. Some symptoms are strongly suggestive of the presence of endometriosis, whereas many affected patients are asymptomatic. The most common symptoms associated with endometriosis are pelvic pain, infertility, and dysfunctional uterine bleeding. Other, less common symptoms may occur from endometriosis implants in unusual sites.
Pelvic Pain
Pelvic pain may be the most common presenting symptom of endometriosis, occurring to some degree in up to 80% of patients.113, 114 Pain may occur at any time in the menstrual cycle and is often poorly localized. This symptom has many different manifestations with descriptions from patients of backaches, rectal pressure, constant lower abdominal aches, and severe cramps. Many mechanisms to explain pain symptoms have been proposed but remain speculative. It is reasonable to assume that the scarring and retraction from fibrosis resulting in anatomic distortion and fixation of pelvic structures may contribute to the development of pain. Fibrosis and adhesions may cause nerve damage, tissue destruction, and devitalization of tissues from the disruption of blood supply. Prostaglandin and histamine release also may exacerbate pain symptoms. In the absence of anatomic distortion, irritation from small implants in critical locations or deeply infiltrating implants115 may cause disabling pain. In contrast, large endometriomas occasionally are asymptomatic.
Dysmenorrhea is a classic symptom of endometriosis. Menstrual cramps that begin and progressively worsen in previously asymptomatic women or differ in character and severity from other cramps may be an indicator of endometriosis. Occasionally, pain may radiate into the vagina, thighs, or perineum. The onset of symptoms generally occurs before the onset of menstruation and gradually improves over several days after initiation of flow. The severity and duration of dysmenorrhea can vary from cycle to cycle. Although the role of prostaglandins is unclear, antiprostaglandin therapy may be effective in reducing dysmenorrhea symptoms.
Dyspareunia is also a common symptom in women with endometriosis. This symptom is usually associated with implants involving the uterosacral ligament, rectovaginal septum, upper vagina, or posterior cul-de-sac and is usually exacerbated during menstruation. A fixed, retroverted uterus associated with significant pelvic adhesions may cause pain with deep penetration. In one study, however, the severity of deep dyspareunia was reported to be inversely related to the stage of endometriosis.116 In another study, dyspareunia was found to be a more common symptom leading to diagnosis in stage I–II endometriosis compared to stage III–IV endometriosis.114
Dyschezia may result from endometriosis implants on or near the rectum or from adhesions. Because of the generally diffuse nature of pelvic discomfort, patients may overlook this symptom. Specific inquiry with regard to the cyclic occurrence of painful bowel movements may be necessary.
Infertility
Infertility is frequently the only presenting symptom in patients with endometriosis. Because of limitations from selection bias, the incidence of infertility in women with endometriosis is unknown. The incidence of endometriosis in infertile women, however, ranges from 4.5 to 33% (mean, 14%).117 In comparison, the prevalence of endometriosis in women undergoing tubal ligation is 4.1%.3 In one study, the reported incidence of endometriosis in infertile women was 21%, compared with a 2% incidence in fertile controls.118
In the presence of adhesions or significant anatomic distortion, infertility may be reasonably explained by mechanical interference, with oocyte pickup and transport and altered tubal peristalsis. In the absence of anatomic distortion of the pelvis, the mechanism of subfertility associated with endometriosis implants alone is poorly understood. Several theories have been proposed to explain the decreased fecundity. Some of these include altered folliculogenesis, ovulatory dysfunction, sperm phagocytosis, impaired fertilization, defective implantation, inhibition of early embryo development, luteal phase defects, and immunologic alterations.75, 119, 120, 121, 122, 123, 124, 125, 126, 127, 128 Chronic inflammatory changes in the peritoneal cavity of women with endometriosis are associated with increased peritoneal fluid volume and increased number, concentration, and activity of macrophages.129, 130, 131, 132 The peritoneal fluid leukocytes are thought to interfere with fertility by exerting direct cytotoxic effects or by releasing cytokines and proteolytic enzymes into the pelvic milieu that can affect gamete function or embryo growth.
The results of other studies suggest that endometriosis implants alone may not be a cause of infertility. In animal studies, transplanted endometrium reduced fertility only in the presence of adhesions.133, 134, 135 Fertility was not adversely affected in the absence of pelvic distortion.136 In women undergoing donor insemination, no difference in monthly fecundity was observed between women with endometriosis and those without the disease.137 A multivariate study of potential infertility factors in a large cohort of infertile women revealed no change in the cumulative conception rate from endometriosis in the absence of adhesions.138 Other investigators, however, have found lower fecundity in women with endometriosis undergoing donor insemination.139 The association between the presence of endometriosis implants alone and subfertility is still debated.
Dysfunctional Uterine Bleeding
Abnormal uterine bleeding frequently has been associated with endometriosis.17 Most cases of bleeding, however, were attributed to coexistent pathology rather than true dysfunctional uterine bleeding. In one study, anovulation was reported in 17% of women with endometriosis.140 This uncontrolled, retrospective review, however, only showed an association between anovulation and endometriosis, rather than a causal relation that would eventually result in irregular bleeding. In another study, menstrual irregularities were reported in 12–14% of patients, depending on the stage of endometriosis, which was similar to the incidence in the general population.141 The available data are insufficient to conclude that endometriosis causes dysfunctional uterine bleeding.
Other Symptoms
Uncommon symptoms are usually attributable to endometriosis involvement of atypical locations. In addition to bowel implants that can cause rectal bleeding or obstruction, endometriosis can be located in the bladder, causing suprapubic pain, frequency, urgency, dysuria, and hematuria. Ureteral involvement may cause upper urinary tract symptoms such as flank pain or backaches. Pulmonary involvement can result in pleuritic pain, pleural effusion, cough, hemoptysis, or pneumothorax.142 In patients with upper abdominal or shoulder pain, diaphragmatic endometriosis should be considered.143 Cyclic headaches or seizures may indicate brain lesions.144 Sciatica has been reported from endometriosis in the retroperitoneal space.145 Some symptoms such as pain or bowel obstruction may persist despite castration or menopause, usually from scarring or adhesions.
PHYSICAL FINDINGS
The most characteristic physical findings associated with endometriosis are tenderness and nodular thickening of the uterosacral ligaments, posterior uterus, and cul-de-sac. A fixed, retroverted uterus and thickened parametrial areas may indicate more advanced disease. Significant cystic formation may be detected as adnexal enlargement or tenderness. Endometriosis of the vagina, perineum, umbilicus, inguinal area, or surgical scars may be visible as pigmented lesions that have cyclic pain and swelling.
Examination during menstruation may be more revealing because of the more pronounced disease manifestations at this time in the menstrual cycle. Rectovaginal examination is particularly helpful in evaluating the posterior cul-de-sac structures. Often, physical findings are absent or minimal even in women with significant disease.
DIAGNOSIS
Clinical suspicion of endometriosis usually is a product of the history and physical examination. Confirmation of endometriosis, however, requires direct visualization and occasionally biopsy if the surgeon is uncertain of the diagnosis. The initial clinical assessment identifies patients at risk for endometriosis who should undergo further evaluation by laboratory tests, diagnostic imaging, and laparoscopy.
Laparoscopy
Laparoscopy is the gold standard for the diagnosis of endometriosis. Because of the heterogeneous and sometimes subtle appearance of implants, however, the accuracy of diagnosis depends on the ability of the surgeon to identify the disease. Endometriosis may be found anywhere in the abdominal and pelvic cavities. A thorough and systematic examination of the pelvis and abdomen is essential in all patients to identify and document all endometriotic lesions. Care should be taken not to overlook peritoneal pockets and areas hidden from view such as the ovarian fossa. Techniques such as the bubble test, which involves the infusion of short bursts of crystalloid into the cul-de-sac and the observation of excessive soaplike bubbling or coating the peritoneal surfaces with bloody peritoneal fluid, may improve the detection of implants.146, 147
Some endometriosis lesions may be retroperitoneal with no surface involvement. Deep, invasive lesions may not be identified by visual inspection alone. Careful palpation of all surfaces using a probe may be necessary to detect these implants. A history of localized pain in conjunction with the preoperative examination may help to focus attention on a particular area. The depth of invasion can be determined only at the time of excision. Contraction and scarring can be identified by tethering of the surrounding tissue to nonpliable tissue. The surgical findings should be carefully documented even though current staging systems do not always accurately predict postoperative pain relief or pregnancy rate.148
Imaging Techniques
Imaging studies may be a useful adjunct in the identification of patients with endometriosis. Among the various techniques available, ultrasonography and magnetic resonance imaging (MRI) are the most useful. Techniques such as standard radiography and computed tomography are rarely useful in the diagnosis of endometriosis.
ULTRASONOGRAPHY.
Ultrasound examination is primarily used to detect endometriosis. The usefulness of ultrasonography in detecting focal implants is poor with a reported sensitivity of as low as 11%.149 In contrast, the sensitivity and specificity in relation to the detection of endometriomas is 83% and 98%, respectively.150, 151 Examination is best performed using the transvaginal approach with high-frequency probes. Serial ultrasonography may be helpful for following patients during the course of medical therapy or after surgery to detect recurrences.
Endometriomas have several different ultrasonographic appearances.152 They usually appear as cystic masses with thick walls and scattered internal echoes. Some endometriomas contain septations, a combination of cystic and solid elements, or primarily solid components and may be indistinguishable from an ovarian abscess or neoplasm. The diagnostic accuracy can be improved by Doppler flow studies. A scoring system based on clinical parameters, CA-125 levels, ultrasound findings, and color Doppler flow had a sensitivity and specificity above 99%.153
MAGNETIC RESONANCE IMAGING.
Ultrasonography remains as the initial choice of imaging modalities for evaluation of adnexal masses. MRI, however, is useful when further characterization of the adnexa is required. The diagnostic sensitivity, specificity, and predictive accuracy for MRI diagnosis of endometriomas are 90%, 98%, and 96%, respectively.154 MRI is the superior method for differentiating an endometrioma from other gynecologic masses. This imaging method also may detect ovarian adhesions and extraperitoneal endometriotic masses.155 The age of hemorrhage may be distinguished by using T1- and T2-weighted images because the signal characteristics vary. Although MRI may detect diffuse pelvic lesions such as endometriosis better than ultrasonography, the sensitivity is low.155 As with ultrasound, MRI may be useful in monitoring therapeutic response to treatment of endometriomas.
Laboratory Tests
Serum CA-125 levels have been assessed in several studies as a diagnostic test for the detection of endometriosis. Although elevations in CA-125 concentration have been associated with endometriosis, the performance of CA-125 testing as a reliable screening test for endometriosis has been poor because of low sensitivity in detecting the disease.156 For selected uses, however, some studies have suggested that CA-125 testing may be helpful. In women with documented endometriosis and in selected populations such as women with infertility, CA-125 levels were reported to correlate with responses to surgical treatment and predict poor outcome.157, 158 In contrast, the value of following CA-125 levels to monitor treatment effect after medical or surgical treatment has been questioned by others.159 The routine use of CA-125 in subfertile patients has been proposed as an inexpensive test to identify a subgroup of patients who are more likely to benefit from early laparoscopy.156 An elevated CA-125 level combined with positive clinical findings was reported to have better results in detecting pelvic endometriosis with a sensitivity and specificity of 87% and 83%, respectively.160 Another potential application of CA-125 testing is differentiation of an endometrioma from a hemorrhagic corpus luteum cyst.161
Another serum protein, PP14, has been evaluated as a marker for endometriosis. PP14 levels correlate with the severity of endometriosis and decrease during suppressive medical treatment of endometriosis.162, 163 The sensitivity and specificity of PP14 in the diagnosis of endometriosis was 59% and 96%, respectively.163
Serum anti-endometrial antibodies also have been evaluated as a test for endometriosis. Elevation of anti-endometrial antibodies is usually observed in the presence of endometriosis. The reported sensitivity and specificity of anti-endometrial antibodies are 83% and 79%, respectively.164 In the same population, CA-125 testing resulted in a lower sensitivity and comparable specificity. In another study, anti-endometrial antibodies could not be found using several different detection methods used previously in other studies.165 The clinical applicability of testing anti-endometrial antibodies remains to be determined.
CLASSIFICATION
Several classification systems for endometriosis have been proposed to allow clear communication among those who study and treat this disease. Classification systems before 1978 lacked widespread acceptance and use. In 1979, a committee of experts, convened by the American Fertility Society (AFS) to develop a classification system, published a scalar scoring system with arbitrary values assigned to each disease locus.166 The cumulative score determined the stage of disease. In 1985, the scheme was revised to better account for adnexal adhesions and invasive disease167 (Fig. 5). The ideal classification system should enable accurate assessment of the extent and location of disease, be useful in predicting outcome based on the stage of disease, allow predictable outcomes from similar stages of disease in response to treatment, and provide guidance in selecting the appropriate treatment.168 Unfortunately, all attempts to develop a classification scheme for endometriosis that fulfills these criteria have failed. The current classification system is partially hindered by the limited extent of our knowledge about the natural course of the disease. Moreover, the system is based on clinical opinion rather than empiric data and relies on a scoring system with arbitrary point assignments to disease sites that may not reflect the true relative risk. The thresholds that define the stages of disease severity are arbitrary and lack the necessary testing to determine its accuracy.
|
Studies comparing stage-specific treatment outcomes are hindered by the limited ability of the AFS classification system to correlate the anatomic abnormalities with the degree of infertility and pelvic pain. For example, mild endometriosis can include deeply invasive, nodular lesions that may have profound adverse effects on fertility and cause significant pain. The AFS classification scheme was designed primarily for women with endometriosis and infertility, which may not be applicable to women with endometriosis and pelvic pain. Although a classification system is necessary to allow comparisons of treatment efficacy in different studies, it is of limited utility because of the lack of correlation with prognosis.
TREATMENT
In the treatment of endometriosis, diverse therapeutic approaches, including no treatment, medical treatment, surgical treatment, and a combination of medical and surgical treatment, have been used to address the clinical consequences (i.e. pain, infertility, and pelvic masses). The use of analgesia (e.g. nonsteroidal antiinflammatory drugs) may also be considered in patients with pain. Despite shortcomings in the classification system on which the studies evaluating treatment outcome are based, sound clinical decisions regarding treatment must be made with the available data. Initial assessment of the reproductive goals of the patient is essential before initiating treatment. Moreover, a clear understanding of the treatment options and the desired end point can facilitate the formulation of a treatment plan to address the individual needs of each patient.
Evaluation of Outcome Data
From the perspective of the patient, outcomes assessment data are the most relevant. The effectiveness of a particular treatment in reducing pain or increasing the monthly chance of conceiving is the question addressed by numerous clinical studies. Prospective, randomized, controlled trials are required to determine the most effective treatment approach. Unfortunately, most studies are uncontrolled or retrospective, making them prone to selection bias. As a result, these studies are more likely to conclude that a treatment is efficacious when in actuality it is not.
In evaluating the clinical response to infertility treatment, consideration should be given to the method of data reporting and analysis. Crude or simple pregnancy rates are simple to calculate and have been commonly used. Because pregnancy rates increase with longer patient follow-up, crude pregnancy rates are of limited value. Life-table analysis or fecundity rates have been used to account for the time-dependent nature of pregnancy. Although these methods are preferred for use in studies investigating the effectiveness of infertility treatment, they cannot correct for selection bias. Meta-analysis is another useful tool because the data from several studies are pooled together. This method of analysis, however, does not correct for the different lengths of follow-up among the studies. Moreover, the subtleties of the data from each study may be lost in the process.
Another consideration in infertility studies is the background conception rate. In many situations, endometriosis is associated with a relative decrease in fertility rather than absolute infertility. Pregnancies occur at a background rate in these women without any intervention. This rate must be determined to assess the efficacy of a particular treatment.
In assessing therapeutic interventions for endometriosis-associated pain, difficulties are encountered in the objective assessment of the outcome measure of pain because of its subjective and heterogeneous nature. The perception of pain is the manifestation of a complex interaction of physiologic processes, sensory thresholds, personality, culture, mood, psychologic influences, and knowledge regarding pain. Another important factor is the proper accounting for the significant placebo effect associated with pain treatment. A partial response to placebo treatment has been reported in up to 55% of patients with endometriosis-associated pain.169 For treatments that are effective in relieving pain, a recurrence of symptoms can be expected in a number of patients. Investigation of the recurrence rate is important for a more complete evaluation of a particular therapeutic regimen. Although it is difficult to make definitive conclusions regarding the efficacy of therapeutic interventions, knowledge of the data can assist in making a more rational decision regarding treatment.
Medical Treatment
Medical treatment consists of hormonal therapy that most commonly includes combination oral contraceptives, high-dose progestins, danazol, and GnRH agonists. The basis of pharmacologic therapy is that endometriosis implants are capable of responding to hormones. These medications interrupt the cycle of stimulation and bleeding of ectopic endometrial tissue and induce atrophy of the implants, decreasing pain and the inflammatory response that may cause fibrosis and adhesions. Unfortunately, current medical therapy is not definitive in the treatment of endometriosis because fibrosis and adhesions cannot be removed and recurrence of endometriosis may occur after cessation of treatment.
In the treatment of infertility, medical therapy alone or in combination with surgery does not improve pregnancy rates in women with endometriosis-associated infertility.170 Medical therapy results in additional costs, side-effects, and requisite contraception period, rendering this approach inadvisable in patients whose only symptom is infertility. The combination of medical therapy with surgery, such as the preoperative use of GnRH agonists for severe endometriosis, may be implemented as indicated to control pelvic pain before a delayed surgery or possibly to improve the pelvis before surgery.171 Preoperative medical treatment, however, has not been shown to improve postoperative pregnancy rates.
In contrast, medical treatment for pain is effective in reducing symptoms.172, 173 Uncontrolled trials have shown an improvement in pain symptoms in approximately 80–90% of patients receiving high-dose progestin, danazol, gestrinone, or GnRH agonists.174, 175, 176, 177 Estimates of recurrence rates vary with a positive correlation between the probability of recurrence and severity of disease. A recurrence rate up to approximately 50% per year has been reported.178 As with any medical treatment, the benefits of pain relief must be weighed against the likely occurrence of undesirable side-effects that may limit the use of a medication, potentially rendering it less effective.
ORAL CONTRACEPTIVES.
The goal of estrogen and progestins administered as oral contraceptives is to induce a pseudopregnancy state. These hormones promote decidualization and eventually atrophy of endometrial implants with continued treatment, interfering with the growth of endometriosis.179, 180 Another potential benefit of oral contraceptive use includes reduction of retrograde menstrual flow from the resulting amenorrhea associated with continuous daily use. Because of the initial proliferative response of endometrial implants to treatment, an exacerbation of symptoms may be encountered in the first 2–3 months before improvement is seen. As a result, treatment is usually continued for at least 6–12 months. The more common side-effects are nausea, weight gain, fluid retention, breast tenderness, mood changes, and breakthrough bleeding. No prospective, controlled studies have shown that treatment with oral contraceptives results in resolution of disease or improved pregnancy rates. Many clinicians, however, feel that they are a reasonable, relatively inexpensive, and effective method to control endometriosis.
PROGESTINS.
Progestins are another often considered medication for the treatment of endometriosis that acts in a similar fashion to oral contraceptives by promoting decidualization and atrophy of endometrial tissue. The most commonly used progestin for endometriosis is the progesterone derivative medroxyprogesterone acetate (MPA). Depot MPA, progesterone-derived megestrol acetate, and the 19-nortestosterone derivative norethindrone also have been used. Although menstruation is usually suppressed with these medications, breakthrough bleeding is a common problem, occurring in 38–47% of patients.181 Other common side-effects, which are reversible, include nausea, breast tenderness, fluid retention, and depression.
The typical oral dose of MPA is 30 mg daily for 3–6 months. The use of MPA at this dose and megestrol acetate appear to provide significant pain relief.175, 182 In a prospective, randomized, placebo-controlled study, high-dose MPA (100 mg/day) for 6 months followed by a 6-month observation period resulted in pain relief comparable to danazol and significantly better than placebo.172 Moreover, after this 1-year period, laparoscopy revealed a significant reduction in disease volume compared with placebo, which was as effective as danazol. A reduction in high-density-lipoprotein cholesterol levels with high-dose MPA has been reported.183 The significance of this reduction, however, is unknown.
In contrast to its ability to relieve pain, progestins are not effective in improving endometriosis-associated infertility. In a nonrandomized, controlled study of women with early-stage endometriosis, no difference in the cumulative pregnancy rates at 30 months was observed with oral MPA, danazol, or expectant management.184 Similarly, in a study of women at all stages of endometriosis treated with high-dose MPA, danazol, or placebo, the pregnancy rates among the treatment groups were not different after 30 months of observation. Moreover, progestins suppress ovulation, delaying the opportunity for conception. Progestin therapy is generally not recommended for patients with endometriosis-associated infertility.
DANAZOL.
Danazol is an orally active isoxazol derivative of 17α-ethinyl testosterone (ethisterone) that has been used for endometriosis treatment since 1971.185 The clinical effects of hypoestrogenic vaginal changes, vasomotor symptoms, and endometrial atrophy associated with ovarian inactivity from danazol use have resulted in the description of a “pseudomenopause.” Danazol, however, does not alter basal levels of gonadotropins. Suppression of the midcycle follicle-stimulating hormone and luteinizing hormone surge occurs, resulting in a chronic anovulatory state and amenorrhea.186, 187
Many other hormonal effects have been attributed to danazol. Danazol inhibits multiple enzymes in the steroidogenesis pathway188 and increases free testosterone levels by displacing it from sex hormone-binding globulin (SHBG).189 Estradiol is also displaced from SHBG along with progesterone and cortisol from corticosteroid-binding globulin. Danazol binds well to the androgen receptor190 and interacts with progestational and glucocorticoid cytosol receptors.191, 192
Danazol is associated with numerous side-effects193 (Table 2) that are primarily attributable to its androgenic activity and have limited its widespread use among patients. Although most of the side-effects are reversible, some may be irreversible such as deepening of the voice,194 and the occurrence of this side-effect is an indication for discontinuing the medication. The potential metabolic side-effects include increased serum enzyme levels possibly associated with cholestatic jaundice,195, 196 decreased SHBG levels,197 and decreased levels of high-density lipoproteins.183, 198 These alterations are expected to return to normal after completion of therapy within several weeks. Long-term use of danazol has raised some concerns regarding the risk of atherosclerotic heart disease due to changes in the lipid profile.
Table 2. Side-effects of danazol treatment
Side-effect | Incidence (%) |
Weight gain* | 85 |
Muscle cramps | 52 |
Decreased breast size | 48 |
Flushing | 42 |
Mood change | 38 |
Oiliness, skin or hair | 37 |
Depression | 32 |
Sweating | 32 |
Edema | 28 |
Change in appetite | 28 |
Acne | 27 |
Fatigue | 25 |
Hirsutism | 21 |
Decreased libido | 20 |
Nausea | 17 |
Headache | 17 |
Dizziness | 10 |
Insomnia | 10 |
Rash | 8 |
Increased libido | 8 |
Deepening of voice | 7 |
*0–1 lb, 15%; 1–5 lb, 22%; 6–10 lb, 32%; 11–15 lb, 18%; 16–20 lb, 11%.
(Adapted from Buttram VC et al: Treatment of endometriosis with danazol: report of a 6-year prospective study. Fertil Steril 37:478, 1982)
The recommended dosage of danazol has varied, with most authorities recommending 400 to 800 mg daily in divided doses. The duration of treatment is usually 6 months. The general consensus is that amenorrhea must be induced for danazol to be effective. At 600–800 mg/day, danazol produced amenorrhea in 90–100% of women.199 The 400- and 200-mg/day doses resulted in amenorrhea in 80% and 44% of women, respectively. To minimize side-effects, danazol is occasionally started at 400 mg/day and titrated upward as tolerated until the desired effect is achieved.
Symptomatic improvement in pain has been reported with danazol treatment in many trials. After 6 months of danazol, improvement in pain was observed in up to 90% of women.200 In a randomized, controlled study, pain reduction was significantly better in women treated with danazol compared with placebo for up to 6 months after discontinuation of therapy.172 In the same study, a reduction in apparent implants was noted in 60% of danazol-treated women compared with 18% in the placebo group. Unfortunately, danazol along with the other pharmacologic interventions are unable to reduce the amount of adhesions and the pain that may result from them. The long-term recurrence of pain has not been well studied. One report, however, suggests that the pain symptom recurrence rate is about 50% per year.201
The effectiveness of danazol in treating infertility has been less encouraging. One randomized, prospective study of danazol treatment of minimal endometriosis with 12 months of follow-up resulted in a cumulative pregnancy rate of 37.2% in the danazol group and 57.4% in the untreated group.200 In another randomized, placebo-controlled study of all stages of endometriosis with 30 months of follow-up, the cumulative pregnancy rates in the danazol group and placebo group were 33% and 46%, respectively.202 In light of these studies and the inability to treat anatomic distortions, danazol has no proven benefit in the treatment of endometriosis-associated infertility.
GESTRINONE.
Gestrinone is a 19-nortestosterone derivative that acts as an androgen receptor agonist and a progesterone receptor agonist or antagonist. Treatment with this steroid results in amenorrhea and endometrial atrophy similar to danazol.203, 204 The potential side-effects, which are similar to those of danazol, tend to be mild and transient. Compared with danazol, the incidence of side-effects is less with gestrinone.205 Moreover, no adverse effects on the lipid profile or liver function tests were noted.
Because of the long half-life, gestrinone is typically administered in oral doses two or three times weekly (5–10 mg/week). After 6 months of treatment, a significant reduction in endometriosis implants was observed in a randomized, placebo-controlled study.206 Gestrinone also appears to be effective in reducing pain symptoms.206 In the treatment of infertility, however, gestrinone did not improve the cumulative pregnancy rate compared with placebo or a control group with unexplained infertility.207 There is no evidence to support the use of gestrinone for infertility treatment in patients with endometriosis.
GONADOTROPIN-RELEASING HORMONE ANALOGS.
The GnRH analogs are synthetic decapeptides that have substitutions at the 6 and sometimes at the 10 position relative to the naturally occurring GnRH decapeptide. These synthetic analogs are long-acting and downregulate the pituitary gland, resulting in a reversible decrease in gonadotropins and subsequent “medical oophorectomy” with continued use.208 The amount of time required to reach castrate levels of estradiol is approximately 3–6 weeks. Various forms of GnRH analogs are available that can be administered intranasally, by injection, or as a subcutaneous pellet. All of the available analogs are effective in producing hypoestrogenism and amenorrhea.
The potential side-effects of GnRH analogs include hot flashes, vaginal dryness, irregular vaginal bleeding, insomnia, depression, fatigue, irritability, headache, and decreased libido. Compared with danazol, the analogs produced more hot flashes and vaginal dryness but less weight gain, mood changes, and fluid retention.173 One of the primary concerns with the prolonged use of GnRH analogs is the potential for bone demineralization because of hypoestrogenism.209 The trabecular bone loss appears to be reversible if therapy is limited to 6 months.210
The gonadal suppression obtained with GnRH analogs results in endometriosis implant regression and pain relief. The GnRH analogs were as effective as danazol in causing regression of endometriosis implants.173, 178, 211 Similarly, pain relief also has been demonstrated after treatment. After leuprolide acetate treatment, a decrease in pelvic pain, dysmenorrhea, pelvic tenderness, and pelvic induration was observed compared with placebo.212 GnRH analogs also compare favorably to danazol in treating pain symptoms.211, 213, 214 The recurrence rate of pain after completion of treatment is less clear. One study reported about one half the patients experiencing recurrence of symptoms by 1 year.178
Treatment of endometriosis-associated infertility with GnRH analogs does not appear to be beneficial. Compared with danazol, no difference in the pregnancy rates was observed at 12 months or 18 months of follow-up.173, 178 In most situations, the use of GnRH analogs with infertility as the only indication is generally not advisable.
The adverse effect of prolonged hypoestrogenism has limited the long-term use of GnRH analogs for the treatment of endometriosis. Because of the recurrence rate of endometriosis after discontinuation of therapy, prolonging treatment with these effective medications would be advantageous. To this end, add-back therapy combined with GnRH analogs has been employed to minimize the short- and long-term side-effects of hypoestrogenism while maintaining therapeutic efficacy.215
The various agents and regimens that have been used have generally yielded good results.216 These regimens include progestin only (e.g. medroxyprogesterone acetate, norethindrone, norethindrone acetate, tibolone), progestin (e.g. norethindrone) plus bisphosphonate (e.g. sodium etidronate), and estrogen (e.g. conjugated equine estrogens, 17β-estradiol) plus progestin (e.g. medroxyprogesterone acetate, norethindrone). Suppression of vasomotor and vaginal symptoms, elimination of significant bone mineral density loss, and a decrease in pelvic pain was observed with all the add-back regimens. Adverse alterations in the high-density- and low-density-lipoprotein cholesterol ratio occurred with higher norethindrone doses (10 mg/day).217 Current recommendations are not to use add-back therapy for anticipated GnRH agonist treatment periods of less than 3 months, to consider add-back for 3- to 6-month treatment periods, and to use add-back for prolonged GnRH agonist treatment beyond 6 months.216 The simplest add-back regimen is norethindrone acetate (5 mg/day). Other regimens also found to be successful in alleviating symptoms and achieving pain relief after 1 year are low-dose norethindrone (2.5 mg/day) plus a bisphosphonate or norethindrone acetate (5 mg/day) in conjunction with conjugated equine estrogens (0.625 mg/day). Supplemental calcium (1000 mg/day) should be administered during treatment. Periodic assessment of bone mineral density and lipid profiles is also recommended.
Surgical Treatment
The surgical approach to endometriosis may be accomplished by laparotomy or laparoscopy. With improvements in equipment and operative technique, laparoscopy is the most common choice for surgery. The degree of success, however, depends on the laparoscopic skills of the surgeon. Laparoscopy provides better visualization, less tissue trauma and exposure to foreign bodies, possibly less adhesion formation, and lower complication rates.218, 219 Laparoscopic incisions are smaller and less painful, allowing faster recovery times.220 The disadvantages of laparoscopy compared with laparotomy include the lack of three-dimensional perspective, greater likelihood of operator fatigue, inability to palpate structures, and need for expensive equipment. Laparotomy is usually reserved for extensive enterolysis, bowel resection, or other situations deemed too complex for the laparoscopic approach.221
Laparoscopic elimination of endometrial implants may be accomplished by laser ablation, electrosurgical desiccation, or sharp resection. The type of laser used during laparoscopic surgery depends on the desired laser characteristics for the particular clinical situation. The carbon dioxide (CO2) laser has excellent precision (depth of tissue destruction is 0.1 mm) but poor coagulating ability that allows the surgeon to create tissue injury at a precise and identifiable localized area. The potassium-titanyl-phosphate laser (KTP532) and argon lasers are less precise than the CO2 laser but have better coagulating properties. The neodymium-doped yttrium-aluminum-garnet (Nd:YAG) laser has good coagulating properties but poor precision (depth of tissue destruction is 4 mm) and can cause large volume thermal injury that is invisible to the operator. Sharp resection is effective in removing disease with a low risk of inadequate treatment but is prone to increased bleeding. Unipolar electrosurgery is also effective but has the risk of deeper tissue damage. Bipolar electrosurgery may be used to desiccate endometriosis lesions. The precise extent of tissue destruction, however, cannot be determined and carries the risk of inadequate treatment.
The techniques used during surgery are directed toward removing all endometrial implants in an atraumatic, hemostatic fashion in the least amount of time. The choice of instruments must reflect the best judgment and skill level of the surgeon as to the optimal means of accomplishing these goals. Adhesions are excised rather than simply lysed because of the possible presence of endometriosis within adhesions. Reduction of tissue desiccation and maintenance of a clean surgical field is facilitated by copious irrigation with physiologic fluids. The operative success rate correlates with meticulous surgical technique that maintains serosal integrity and decreases the risk of de novo adhesion formation. Close adherence to surgical principles can increase the likelihood of a successful outcome222 (Table 3).
Table3. Surgical principles in the treatment of endometriosis
Knowledge of disease and treatment modalities
Experienced surgeon
Adequate facilities, personnel, and equipment
Appropriate patient selection
Informed consent
Proper patient position
Careful pelvic evaluation
Maximum exposure
Use of magnification
Minimum tissue trauma
Excellent hemostasis
Removal of all diseased tissue
Avoidance of foreign body material
Confirmation of tissue pathology
From Adamson GD: Laparoscopic treatment of endometriosis. In Adamson GD, Martin DC (eds): Endoscopic Management of Gynecologic Disease. Philadelphia: Lippincott-Raven, 1996.
INFERTILITY.
Surgery is usually the treatment of choice for endometriosis-associated infertility. The advantage of surgical therapy in the treatment of infertility is the opportunity to remove adhesions and restore normal anatomy. In contrast to medical treatment, a period of contraception is not required. This provides the older infertility patients a time savings of up to 6 months, during which time fertility may decrease. In general, within 1–2 years after surgical therapy for endometriosis, a pregnancy rate of approximately 65% can be expected. In a study of women in whom endometriosis was the only known cause of infertility, about one half of the women conceived within the first 6 months after surgery, and 86% conceived within 15 months.223 Recurrence of endometriosis implants after surgery was reported for 28% of patients within 18 months224 and 40.3% after 5 years.225 In a meta-analysis of studies comparing surgery with nonsurgical treatments for all stages of endometriosis-associated infertility, the surgical approach was found to be superior.226
In patients with minimal or mild endometriosis, laparoscopic treatment has been used frequently because treatment can be accomplished easily during diagnostic laparoscopy. However, the ablation or removal of endometriosis implants potentially can increase the risk for postsurgical adhesion formation. The decision to treat minimal or mild endometriosis has been based on the nature and location of the lesions, on the potential of the disease to become more advanced, and on the presence of pain symptoms. In light of the difficulties in evaluating the data in the literature, the lack of rigorous clinical studies showing an improvement in fertility, and the variable length of follow-up in infertility studies, the conventional wisdom has been that surgical treatment for minimal or mild endometriosis does not confer an advantage over expectant management.
Some data support the surgical approach to infertile patients with minimal or mild endometriosis. In a prospective, multicenter, double-blind, controlled, randomized study, surgical treatment by laparoscopy resulted in a significantly higher pregnancy rate after 36 weeks than expectant management.227 Cautery, laser, or a combination of the two were used to treat the endometriosis implants and adhesions. The cumulative probability of pregnancy in the surgically treated versus nontreated group was 30.7% and 17.7%, respectively. The corresponding fecundity rates per 100 person-months were 4.7 and 2.4. However, another prospective, randomized, controlled study did not show any difference in pregnancy rates between treatment and no treatment.228 The combined odds ratio of these two trials favors surgery compared to no treatment with a number needed to treat of 12.229 Although the evidence supports the treatment of minimal or mild endometriosis-associated infertility at laparoscopy, the use of surgery in the infertile patient must be weighed against the costs, risks, and alternative treatments because of the number needed to treat.
In the presence of moderate or severe endometriosis, surgery is the treatment of choice for endometriosis-associated infertility. Because of the usual anatomic distortion associated with moderate or severe endometriosis, surgery has been the usual treatment approach. As a result, few data exist regarding no treatment or medical treatment. The available evidence supports the surgical approach compared with the nonsurgical approach for invasive, adhesive, or endometriotic disease.226 Intuitively, surgical treatment that can potentially correct anatomic defects should result in better outcomes than expectant management or medical treatment, which does not restore normal anatomy.
Because of the ineffectiveness of medical therapy, surgery has been the approach for treating endometriomas. Complete resection of the cyst wall is preferred to minimize thermal injury to the ovary, have greater assurance of complete removal, and obtain a specimen for pathologic examination. In two retrospective studies, pregnancy rates after laparoscopic treatment of endometriomas in infertility patients were 50% (26 of 52) and 52% (12 of 23).230, 231 In a prospective cohort study comparing endometrioma treatment by laparoscopy or laparotomy, the estimated cumulative pregnancy rate at 3 years was 52% with laparoscopy and 46% with laparotomy.232 The size or number of endometriomas did not affect the pregnancy rates. The recurrence rate of resected endometriomas is less than 10%, with an associated 20% incidence of de novo adhesion formation and approximately 80% incidence of recurring complete or partial dense adhesions.230, 233 The use of sutures on the ovary to achieve hemostasis following cyst resection instead of bipolar coagulation may reduce the rate of postoperative adhesion formation234 and functional ovarian damage.235 After drainage and cystectomy, normal ovarian function appears to be retained.236 However, postcystectomy ovaries may also have reduced follicular response in natural and clomiphene citrate-stimulated cycles.237
The posterior cul-de-sac and rectovaginal septum are locations where deeply invading endometriosis can be found. These areas also can be the most difficult to dissect. In one study of infertile patients with partial or complete cul-de-sac obliteration, 74% (34 of 46) of the patients conceived after laparoscopic treatment with 38% (13 of 34) requiring more than one laparoscopy.238
PELVIC PAIN.
Surgical treatment for endometriosis-associated pelvic pain has been poorly studied but appears to be useful. Uncontrolled trials report success in relieving pain in 70–100% of patients.239 In one study, complete relief of pain 1 year after surgery was reported in 82% of patients.240 In a prospective, randomized, double-blind, controlled study comparing CO2 and KTP532 laser laparoscopy treatment of pelvic pain associated with all stages of endometriosis, an improvement or resolution of symptoms 6 months after surgery was observed in 62.5% of treated patients and 22.6% of untreated patients.241 Patients with higher-stage disease had more pain relief 6 months after surgery than patients with mild disease. Another consideration in determining the success of treatment in addition to the percentage of patients experiencing pain relief and the duration of pain relief is the recurrence rate of pain. Unfortunately, a return of symptoms is experienced by at least 10–20% of patients treated for endometriosis-associated pain per year.242
Deep lesions, including those that invade into the rectovaginal septum, appear to correlate with the severity of pelvic pain.243, 244 Complete excision of the lesions offers the best opportunity for relief of pain. In one study of 250 women, surgical excision resulted in a 70% cure rate for pelvic pain and a recurrence rate of less than 5% after 5 years.245 After 1 year, the recurrence rate for pain has been reported to be as high as 32% after surgical excision of infiltrating rectovaginal endometriosis, with only 2 of 151 experiencing severe pain.246 In another study, no dysmenorrhea or dyspareunia was reported after 40 months after surgical excision of rectovaginal lesions.247
Ovarian endometriomas have been treated by various surgical techniques.248 Drainage, cyst stripping or ablation, and wedge excision had comparable results in improving pain symptoms. After surgery, pain relief has been observed in 61–100% of patients.231, 248, 249 The approach of wide excision and drainage has been recommended as an alternative to wedge excision because of less adhesion formation and a recurrence rate (23%)250 similar to that for cyst stripping and ablation. Other studies, however, have reported an even lower recurrence rate (<5%) of endometriomas using the stripping or ablation techniques, which are perhaps the most widely used techniques.249, 250
Definitive surgery consisting of hysterectomy and salpingo-oophorectomy is effective for relieving endometriosis-associated pain. This approach should be considered for patients who fail medical or conservative surgical treatment and can accept loss of fertility. Alternatively, women who have completed childbearing and desire a more definitive approach to their symptoms may elect to proceed with this treatment as the primary option. Persistence of symptoms due to adhesions, residual peritoneal lesions, or ovarian remnant syndrome is possible during the course of endometriosis treatment. Pain relief after hysterectomy and salpingo-oophorectomy is observed in up to 90% of patients.8 In selected patients with no significant ovarian involvement, hysterectomy alone is an option associated with a disease recurrence rate of approximately 7%, requiring reoperation.251 In moderate or severe endometriosis, the risk of recurring pelvic pain has been suggested to be as much as five times greater if the ovaries are not removed at the time of hysterectomy.
The relation between pelvic adhesions and pain is unclear. Adhesions can distort normal anatomic relationships, potentially restricting the mobility and distensibility of organs and causing pain.252 However, a correlation between the extent or location of adhesions and the severity and duration of pain has yet to be demonstrated.253, 254, 255 In uncontrolled studies, adhesiolysis resulted in an improvement in pelvic pain symptoms in approximately 85% of patients.252, 256, 257, 258 Adhesion reformation was observed in 97.1% of patients and at 66% of the sites of original adhesiolysis.259 Despite the uncertainty of the correlation between adhesions and pain, lysis of adhesions appears reasonable in the presence of endometriosis-associated pain, especially when the location of adhesions and pain correlate.
Presacral neurectomy involves interrupting the sympathetic innervation to the uterus at the level of the superior hypogastric plexus. This technique has had variable results when used to treat endometriosis-associated pain. In a randomized, prospective study, presacral neurectomy effectively relieved dysmenorrhea but had variable effects on dyspareunia, lateral pain, and back pain.260 In another randomized, controlled study, however, no significant difference in the frequency and severity of dysmenorrhea, pelvic pain, and dyspareunia was observed.261 Because of the variable results, only selected patients with primarily midline dysmenorrhea unresponsive to conservative treatment should be considered for presacral neurectomy.
Laparoscopic uterosacral nerve ablation (LUNA) is another procedure used for the treatment of endometriosis-associated pain. In a prospective, randomized, double-blind study of women with intractable dysmenorrhea, pain relief after LUNA was observed in 81% of women after 3 months, compared with no pain relief in all the women not having LUNA.262 However, the recurrence of pain after 1 year occurred in approximately one half of the women. For minimal to moderate endometriosis, another study showed improvement in pain symptoms after LUNA and ablation of endometriosis in 62% of women, compared with 23% of untreated women.241 It appears reasonable to perform a LUNA when the uterosacral ligaments are involved with endometriosis or when patients with central chronic pain are unresponsive to other therapies.
Other Treatment
Infertility associated with endometriosis may be addressed by advanced reproductive technologies. A variety of treatment options can be offered, depending on the clinical situation. After an infertility evaluation, the most common treatments are controlled ovarian hyperstimulation with or without intrauterine insemination and the assisted reproductive technologies (ART). These treatments are intended to increase the overall fecundity and do not directly cause regression of endometriosis implants.
Overall, clomiphene citrate treatment does not appear to be better than no treatment, whereas gonadotropin treatment appears to at least double the monthly fecundity. In a controlled, randomized study of women with minimal or mild endometriosis, controlled ovarian hyperstimulation with gonadotropins resulted in a monthly fecundity rate of 15%, compared with 4.5% in untreated women.263 Similar conclusions were reached in another study of women with minimal or mild endometriosis, demonstrating the superiority of gonadotropin and intrauterine insemination over no treatment.264 The addition of intrauterine insemination to clomiphene citrate and gonadotropin therapy appears to be helpful in increasing pregnancy rates.265 Although data on the treatment of moderate or severe endometriosis are relatively sparse, the expectation is for no improvement in pregnancy rates with ovulation induction because of the higher probability of significant anatomic distortion that would interfere with oocyte transport to the fallopian tube.
The assisted reproductive technologies refer to procedures such as in vitro fertilization (IVF), gamete intrafallopian transfer (GIFT), zygote intra-fallopian transfer (ZIFT), tubal embryo transfer (TET), intracytoplasmic sperm injection (ICSI), and assisted hatching. When assessing outcome according to diagnosis, patients with endometriosis were reported to have lower pregnancy rates compared with patients with tubal factor infertility.266, 267, 268 This observation may be attributed to the negative effects of endometriosis that result in a reduction in response to gonadotropins, number of oocytes retrieved, fertilization rates, and implantation rates.269 Based on the observation of lower pregnancy rates from oocytes donors with endometriosis and no decrease in pregnancy rates in oocyte recipients with endometriosis, poor oocyte quality was thought to be responsible for the adverse effect on the pregnancy rate in patients with endometriosis.266 Other studies, however, found no difference in IVF success rates between patients with and without endometriosis.270, 271 Similarly, conflicting data regarding the success rates according to stage of endometriosis have been reported.267, 270, 271 Although success rates appear to be lower in some women with endometriosis, the overall chance of conception with IVF is good with a proportional increase in rates over the years as IVF technology has improved. Moreover, IVF is the best infertility treatment option for infertile patients with endometriosis.
In light of the potential adverse effects of moderate or severe endometriosis on the oocyte, it seems reasonable to consider surgical treatment of moderate or severe disease before initiating IVF cycles. In a prospective, randomized study, however, no difference in pregnancy rates or live birth rates was observed between patients who were treated or not treated for endometriosis at the time of GIFT.272 In the case of endometriomas, surgical removal of endometriomas larger than 4 cm prior to IVF has been recommended.273 It appears that cystectomy, if carefully performed, will not affect ovarian response to gonadotropins.274, 275, 276 Although expert opinion is in favor of surgery to remove endometriomas greater than 3–4 centimeters prior to IVF treatment, conflicting data prevents definitive conclusions from being made.277, 278
Medical suppression with GnRH agonists for 2–3 months may also be considered.279 Frequently, surgery has been performed earlier during the course of the infertility workup. IVF is usually considered after expectant management or controlled ovarian hyperstimulation with intrauterine inseminations has failed after surgery.
CONCLUSIONS
The surgical approach to endometriosis-associated infertility and pain has assumed a prominent role. In light of the relative lack of prospective, randomized, controlled studies and the absence of a scoring system that correlates with the degree of reproductive impairment or pelvic pain, selection of the optimal treatment is often difficult to make. With respect to infertility, however, current data support the surgical approach to endometriosis. Medical treatment is ineffective and should not be used for endometriosis-associated infertility.
The management of endometriosis-associated pain can be multifaceted, with surgical treatment as one of the options. With the exception of selected patients who are young and have relatively mild symptoms that respond to medical therapy, many patients during the course of a diagnostic evaluation have laparoscopy and subsequent treatment of endometriosis. Ultimately, a comprehensive treatment plan that may use various treatment modalities should be developed for each patient's clinical situation, reproductive objectives, and unique needs. As more sophisticated studies are performed, the ability to make better decisions regarding the optimal treatment approach will become possible.
REFERENCES
Sampson JA: Perforating haemorrhagic (chocolate) cysts of the ovary: their importance and especially their relation to pelvic adenomas of endometrial type. Arch Surg 3: 245, 1921 |
|
Wheeler JM: Epidemiology and prevalence of endometriosis. Infertil Reprod Med Clin North Am 3: 545, 1992 |
|
Eskenazi B, Warner ML: Epidemiology of endometriosis. Obstet Gynecol Clin North Am 24: 235, 1997 |
|
Boling RO, Abbasi R, Ackerman G et al: Disability from endometriosis in the United States Army. J Reprod Med 33: 49, 1988 |
|
Wheeler JM: Epidemiology of endometriosis-associated infertility. J Reprod Med 34: 41, 1989 |
|
Velebil P, Wingo PH, Xia Z et al: Rate of hospitalization for gynecologic disorders among reproductive-age women in the United States. Obstet Gynecol 86: 764, 1995 |
|
Houston DE, Noller KL, Melton LJ et al: Incidence of pelvic endometriosis in Rochester, Minnesota, 1970-1979. Am J Epidemiol 125: 959, 1987 |
|
Olive DL, Schwartz LB: Endometriosis. N Engl J Med 328: 1759, 1993 |
|
Clark AH: Endometriosis in a young girl. JAMA 136: 690, 1948 |
|
Kempers RD, Dockerty MB, Hunt AB, Symmonds RE: Significant postmenopausal endometriosis. Surg Gynecol Obstet 111: 348, 1960 |
|
Punnonen R, Klemi PJ, Nikkanen V: Postmenopausal endometriosis. Eur J Obstet Gynecol Reprod Biol 11: 195, 1980 |
|
Schifrin BS, Erez S, Moore JG: Teenage endometriosis. Am J Obstet Gynecol 116: 973, 1973 |
|
Huffman JW: Endometriosis in young teen-age girls. Pediatr Ann 10: 44, 1981 |
|
Vessey MP, Villard-Mackintosh L, Painter R: Epidemiology of endometriosis in women attending family planning clinics. Br Med J 306: 182, 1993 |
|
Sangi-Haghpeykar H, Poindexter AN: Epidemiology of endometriosis among parous women. Obstet Gynecol 85: 983, 1995 |
|
Meigs JV: Medical treatment of endometriosis and significance of endometriosis. Surg Gynecol Obstet 89: 317, 1949 |
|
Scott RB, Te Linde RW: External endometriosis-the scourge of the private patient. Ann Surg 131: 697, 1950 |
|
Lloyd FP: Endometriosis in the Negro woman. Am J Obstet Gynecol 89: 468, 1964 |
|
Ridley JH: The histogenesis of endometriosis. Obstet Gynecol Surv 23: 1, 1968 |
|
Darrow SL, Selman S, Batt RE et al: Sexual activity, contraception, and reproductive factors in predicting endometriosis. Am J Epidemiol 140: 500, 1994 |
|
Cramer DW, Wilson E, Stillman RJ et al: The relation of endometriosis to menstrual characteristics, smoking, and exercise. JAMA 255: 1904, 1986 |
|
Darrow SL, Vena JE, Batt RE et al: Menstrual cycle characteristics and the risk of endometriosis. Epidemiology 4: 135, 1993 |
|
Candiani GB, Danesino V, Gastaldi A et al: Reproductive and menstrual factors and risk of peritoneal and ovarian endometriosis. Fertil Steril 56: 230, 1991 |
|
McCann SE, Freudenheim JL, Darrow SL et al: Endometriosis and body fat distribution. Obstet Gynecol 82: 545, 1993 |
|
Parazzini F, Ferraroni M, Bocciolone L et al: Contraceptive methods and risk of pelvic endometriosis. Contraception 94: 47, 1994 |
|
Frey GH: The familial occurrence of endometriosis: report of five instances and review of the literature. Am J Obstet Gynecol 73: 418, 1957 |
|
Ranney B: Endometriosis. IV. Hereditary tendency. Obstet Gynecol 37: 734, 1971 |
|
Lamb K, Hoffmann RG, Nichols TR: Family trait analysis: a case-control study of 43 women with endometriosis and their best friends. Am J Obstet Gynecol 154: 596, 1986 |
|
Moen MH: Endometriosis in monozygotic twins. Acta Obstet Gynecol Scand 73: 59, 1994 |
|
Hadfield RM, Mardon HJ, Barlow DH, Kennedy SH: Endometriosis in monozygotic twins. Fertil Steril 68: 941, 1997 |
|
Simpson JL, Elias S, Malinak LR et al: Heritable aspects of endometriosis. I. Genetic studies. Am J Obstet Gynecol 137: 327, 1980 |
|
Coxhead D, Thomas EJ: Familial inheritance of endometriosis in a British population. A case control study. J Obstet Gynaecol 13: 42, 1993 |
|
Moen MH, Magnus P: The familial risk of endometriosis. Acta Obstet Gynecol Scand 72: 560, 1993 |
|
Von Recklinghausen F: Adenomyomas and cystadenomas of the wall of the uterus and tube: their origin as remnants of the wolffian body. Wien Klin Wochenschr 8: 530, 1896 |
|
Russell WW: Aberrant portions of the müllerian duct found in a ovary: ovarian cysts of müllerian origin. Bull Johns Hopkins Hosp 10: 8, 1899 |
|
Cullen TS: Adenomyoma of the Uterus. Philadelphia: WB Saunders, 1908 |
|
Phillip E, Huber H. Die entstehung der Endometriose. Gleichzeitig ein bertrag zur Pathologie des interstitiellen Tubenabschnittes. Zentralbl Gynakil 63:7, 1939 |
|
Sampson JA: Heterotopic or misplaced endometrial tissue. Am J Obstet Gynecol 10: 649, 1925 |
|
Sampson JA: Peritoneal endometriosis due to menstrual dissemination of endometrial tissue into peritoneal cavity. Am J Obstet Gynecol 14: 422, 1927 |
|
Geist SH: The viability of fragments of menstrual endometrium. Am J Obstet Gynecol 25: 751, 1933 |
|
Halme J, Hammond MG, Hulka JF et al: Retrograde menstruation in healthy women and in patients with endometriosis. Obstet Gynecol 64: 151, 1984 |
|
Liu DTY, Hitchcock A: Endometriosis: its association with retrograde menstruation, dysmenorrhea and tubal pathology. Br J Obstet Gynaecol 93: 859, 1986 |
|
Kruitwagen RFPM, Poels LG, Willemsen WNP et al: Endometrial epithelial cells in peritoneal fluid during the early follicular phase. Fertil Steril 55: 297, 1991 |
|
Halban J: Metastatic hysteroadenosis. Wien Klin Wochenschr 37: 1205, 1924 |
|
Scott RB, Novak RJ, Tindale RM: Umbilical endometriosis and Cullen's sign: study of lymphatic transport from pelvis to umbilicus in monkeys. Obstet Gynecol 11: 556, 1958 |
|
Javert CT: Pathogenesis of endometriosis based on endometrial homeoplasia, direct extension, exfoliation and implantation, lymphatic and hematogenous metastasis, including five case reports of endometrial tissue in pelvic lymph nodes. Cancer 2: 399, 1949 |
|
Sampson JA: Metastatic or embolic endometriosis due to menstrual dissemination of endometrial tissue into venous circulation. Am J Pathol 3: 93, 1927 |
|
Hobbs JE, Bortnick AR: Endometriosis of the lungs: experimental and clinical study. Am J Obstet Gynecol 40: 832, 1940 |
|
Kale S, Shuster M, Sahmgold I: Endometrioma in caesarean scar: case report and review of the literature. Am J Obstet Gynecol 111: 596, 1971 |
|
Wittich AC: Endometriosis in an episiotomy scar: review of the literature and report of case. J Am Osteopath Assoc 82: 22, 1982 |
|
Schenken RS, Asch RH: Surgical induction of endometriosis in the rabbit: effects on fertility and concentrations of peritoneal fluid prostaglandins. Fertil Steril 34: 581, 1980 |
|
Schmid HH: Artificial endometriosis for therapeutic purposes. Geburtshilfe Frauenheilkd 21: 679, 1961 |
|
Keettel WC, Stein RJ: The viability of the cast-off menstrual endometrium. Am J Obstet Gynecol 61: 440, 1951 |
|
Ridley JH, Edwards IK: Experimental endometriosis in the human. Am J Obstet Gynecol 76: 783, 1958 |
|
TeLinde RW, Scott RB: Experimental endometriosis. Am J Obstet Gynecol 60: 1147, 1950 |
|
Jenkins S, Olive DL, Haney AF: Endometriosis: pathogenetic implications of the anatomic distribution. Obstet Gynecol 67: 335, 1986 |
|
Olive DL, Henderson DY: Endometriosis and müllerian anomalies. Obstet Gynecol 69: 412, 1987 |
|
Gruenwald P: Origin of endometriosis from the mesenchyme of the coelomic walls. Am J Obstet Gynecol 44: 470, 1942 |
|
Oliker AJ, Harns AE: Endometriosis of the bladder in a male patient. J Urol 106: 858, 1971 |
|
Pinkert TC, Catlow CE, Straus R: Endometriosis of the urinary bladder in a man with prostatic carcinoma. Cancer 43: 1562, 1979 |
|
Schrodt GR, Alcorn MD, Ibanez J: Endometriosis of the male urinary system: a case report. J Urol 124: 722, 1980 |
|
Levander G, Normann P: The pathogenesis of endometriosis: an experimental study. Acta Obstet Gynecol Scand 34: 366, 1955 |
|
Merrill JA: Endometrial induction of endometriosis across millipore filter. Am J Obstet Gynecol 94: 780, 1966 |
|
Stock RJ: Postsalpingectomy endometriosis: a reassessment. Obstet Gynecol 60: 560, 1982 |
|
Donnez J, Casana-Roux F, Ferin J, Thomas K: Tubal polyps, epithelial inclusions, and endometriosis after tubal sterilization. Fertil Steril 41: 564, 1984 |
|
Ulukus M, Cakmak H, Arici A: The role of endometrium in endometriosis. J Soc Gynecol Investig 2006 Oct;13(7):467-76. Epub 2006 Sep 20. |
|
Dmowski WP, Steele RW, Baker GF: Deficient cellular immunity in endometriosis. Am J Obstet Gynecol 141: 377, 1981 |
|
Oosterlynck DJ, Cornillie FJ, Waer M et al: Women with endometriosis show a defect in natural killer activity resulting in a decreased cytotoxicity to autologous endometrium. Fertil Steril 56: 45, 1991 |
|
Wilson TJ, Hertzog PJ, Angus D et al: Decreased natural killer cell activity in endometriosis patients: relationship to disease pathogenesis. Fertil Steril 62: 1086, 1994 |
|
Hill JA: Immunology and endometriosis. Fertil Steril 58: 262, 1992 |
|
Garzetti GG, Ciavattini A, Provinciali M et al: Natural killer cell activity in endometriosis: correlation between serum estradiol levels and cytotoxicity. Obstet Gynecol 81: 665, 1993 |
|
DiStefano G, Provinciali M, Muzzioll M et al: Correlation between estradiol serum levels and NK cell activity in endometriosis. Ann N Y Acad Sci 741: 197, 1994 |
|
Garzetti GG, Ciavattini A, Provinciali M et al: Natural cytotoxicity and GnRH agonist administration in advanced endometriosis: positive modulation on natural killer activity. Obstet Gynecol 88: 234, 1996 |
|
Oosterlynck DJ, Meuleman C, Waer M et al: Transforming growth factor-&b.beta; activity is increased in peritoneal fluid from women with endometriosis. Obstet Gynecol 83: 287, 1994 |
|
Fakih H, Baggett B, Holtz G et al: Interleukin-1: a possible role in the infertility associated with endometriosis. Fertil Steril 47: 213, 1987 |
|
Halme J: Release of tumor necrosis factor-alpha by human peritoneal macrophages in vivo and in vitro. Am J Obstet Gynecol 161: 1718, 1989 |
|
D'Hooghe TM, Scheerlinch JP, Koninckx PR et al: Anti-endometrial lymphocytotoxicity and natural killer cell activity in baboons with endometriosis. Hum Reprod 10: 558, 1995 |
|
D'Hooghe TM, Bambra CS, Raeymaekers BM et al: The effects of immunosuppression on development and progression of endometriosis in baboons (Papio anubis). Fertil Steril 64: 172, 1995 |
|
Cunningham DS, Hansen KA, Coddington CC: Changes in T-cell regulation of responses to self antigens in women with pelvic endometriosis. Fertil Steril 58: 114, 1992 |
|
Gleicher N, Dmowski WP, Siegel I et al: Lymphocyte subsets in endometriosis. Obstet Gynecol 63: 463, 1984 |
|
Dudley DJ: The immune system in health and disease. Clin Obstet Gynecol 6: 393, 1992 |
|
Steele RW, Dmowski WP, Marmer DJ. Immunologic aspects of human endometriosis. Am J Reprod Immunol 6:33, 1984 |
|
Evers JLH, Dunselman GAJ, Vanderlinden PJO: Markers for endometriosis. Clin Obstet Gynecol 7: 715, 1993 |
|
Haney AF, Muscato JJ, Weinberg JB: Peritoneal fluid cell populations in infertility patients. Fertil Steril 35: 696, 1981 |
|
Hill JA, Faris HMP, Schiff I, Anderson DJ: Characterization of leukocyte subpopulations in the peritoneal fluid of women with endometriosis. Fertil Steril 50: 216, 1988 |
|
Halme J, Becker S, Haskill S: Altered maturation and function of peritoneal macrophages: possible role in pathogenesis of endometriosis. Am J Obstet Gynecol 156: 783, 1987 |
|
Halme J, Becker S, Wing R: Accentuated cyclic activation of peritoneal macrophages in patients with endometriosis. Am J Obstet Gynecol 148: 85, 1984 |
|
Halme J, White C, Kauma S et al: Peritoneal macrophages from patients with endometriosis release growth factor activity in vitro. J Clin Endocrinol Metab 66: 1044, 1988 |
|
Shifren JL, Tseng JF, Zaloudek CJ et al: Ovarian steroid regulation of vascular endothelial growth factor in the human endometrium: implications for angiogenesis during the menstrual cycle and in the pathogenesis of endometriosis. J Clin Endocrinol Metab 81: 3112, 1996 |
|
Rier SE, Parsons AK, Becker JL: Altered interleukin-6 production by peritoneal leukocytes from patients with endometriosis. Fertil Steril 61: 294, 1994 |
|
Ryan IP, Tseng JF, Schriock ED et al: Interleukin-8 concentrations are elevated in peritoneal fluid of women with endometriosis. Fertil Steril 63: 929, 1995 |
|
Arici A, Tazuke S, Attar E et al: Interleukin-8 concentration in peritoneal fluid of patients with endometriosis and modulation of interleukin-8 expression in human mesothelial cells. Mol Hum Reprod 2: 40, 1996 |
|
Rana N, Braun DP, House R et al: Basal and stimulated secretion of cytokines by peritoneal macrophages in women with endometriosis. Fertil Steril 65: 925, 1996 |
|
Arici A, Oral E, Attar E et al: Monocyte chemotactic protein-1 concentration in peritoneal fluid of women with endometriosis and its modulation of expression in mesothelial cells. Fertil Steril 67: 1065, 1997 |
|
Oral E, Seli E, Bahtiyar MO et al: Growth-regulated α expression in the peritoneal environment with endometriosis. Obstet Gynecol 88: 1050, 1996 |
|
Khorram O, Taylor RN, Ryan IP et al: Peritoneal fluid concentrations of the cytokine RANTES correlate with the severity of endometriosis. Am J Obstet Gynecol 169: 1545, 1993 |
|
Surrey E, Halme J: Effect of peritoneal fluid from endometriosis patients on endometrial cell proliferation in vitro. Obstet Gynecol 76: 792, 1990 |
|
Oosterlynck DJ, Meuleman C, Sobis H et al: Angiogenic activity of peritoneal fluid from women with endometriosis. Fertil Steril 59: 778, 1993 |
|
Strowitzki T, Wiedemann R, Hepp H. Influence of growth factors EGF, IGF-1, and human growth hormone on human endometrial stromal cells in vitro. Ann N Y Acad Sci 626:308, 1991 |
|
Surrey ES, Halme J. Effect of platelet-derived growth factor on endometrial stromal cell proliferation in vitro: a model for endometriosis? Fertil Steril 56: 672, 1991 |
|
Olive DL, Montoya L, Riehl RM, Schenken RS: Macrophage-conditioned media enhance endometrial stromal cell proliferation in vitro. Am J Obstet Gynecol 164: 953, 1991 |
|
Koninckx PR, Barlow D, Kennedy S: Implantation versus infiltration: the Sampson versus the endometriotic disease theory. Gynecol Obstet Invest 47 (Suppl 1): 3, 1999 |
|
Koninckx PR, Kennedy SH, Barlow DH: Pathogenesis of endometriosis: the role of peritoneal fluid. Gynecol Obstet Invest 47 (Suppl 1): 23, 1999 |
|
Lessey BA, Young SL: Integrins and other cell adhesion molecules in endometrium and endometriosis. Semin Reprod Endocrinol 15: 291, 1997 |
|
Mu L, Zheng W, Wang L et al: Alteration of focal adhesion kinase expression in eutopic endometrium of women with endometriosis. Fertil Steril 2008 Mar;89(3):529-37. Epub 2007 Jun 4. |
|
Zeyneloglu HB, Arici A, Olive DL: Environmental toxins and endometriosis. Obstet Gynecol Clin North Am 24: 307, 1997 |
|
Rier SE, Martin DC, Bowman RE et al: Endometriosis in rhesus monkeys (Macaca mulatta) following chronic exposure to 2,3,7,8-tetrachlorodibenzo-p-dioxin. Fundam Appl Toxicol 21: 433, 1993 |
|
Cummings AM, Metcalf JL, Birnbaum L: Promotion of endometriosis by 2,3,7,8-tetrachlorodibenzo-p-dioxin in rats and mice: time-dose dependence and species comparison. Toxicol Appl Pharmacol 138: 131, 1996 |
|
Chatman DL, Zbella EA. Pelvic peritoneal defects and endometriosis: further observations. Fertil Steril 46: 711, 1986 |
|
Redwine DB. Peritoneal pockets and endometriosis: confirmation of an important relationship, with further observations. J Reprod Med 34: 270, 1989 |
|
Stripling MC, Martin DC, Chatman DL et al: Subtle appearance of pelvic endometriosis. Fertil Steril 49: 427, 1988 |
|
Metzger DA, Olive DL, Haney AF: Limited hormonal responsiveness of ectopic endometrium: histologic correlation with intrauterine endometrium. Hum Pathol 19: 1417, 1988 |
|
Pittaway DE: Diagnosis of endometriosis. Infertil Reprod Med Clin North Am 3: 619, 1992 |
|
Sinaii N, Plumb K, Cotton L et al: Differences in characteristics among 1,000 women with endometriosis based onextent of disease. Fertil Steril 2008 Mar;89(3):538-45. Epub 2007 May 11 |
|
Cornillie FJ, Oosterlynck D, Lauweryns JM, Koninckx PR: Deeply infiltrating pelvic endometriosis: histology and clinical significance. Fertil Steril 53: 978, 1990 |
|
Vercellini P, Trespidi L, De Giorgi O et al: Endometriosis and pelvic pain: relation to disease stage and localization. Fertil Steril 65: 299, 1996 |
|
Pauerstein C: Clinical presentation and diagnosis. In Schenken RS (ed): Endometriosis: Contemporary Concepts in Clinical Management. Philadelphia: JB Lippincott, 1989 |
|
Strathy JH, Molgaard CA, Coulam CB, Melton LJ: Endometriosis and infertility: a laparoscopic study of endometriosis among fertile and infertile women. Fertil Steril 38: 667, 1982 |
|
Dmowski WP, Radwanska E, Binor Z, Rana N: Mild endometriosis and ovulatory dysfunction: effect of danazol treatment on success of ovulation induction. Fertil Steril 46: 784, 1986 |
|
Tummon IS, Maclin VM, Radwanska E et al: Occult ovulatory dysfunction in women with minimal endometriosis or unexplained infertility. Fertil Steril 50: 716, 1988 |
|
Muscato JJ, Haney AJ, Weinberg JB: Sperm phagocytosis by human peritoneal macrophages: a possible cause of infertility in endometriosis. Am J Obstet Gynecol 144: 503, 1982 |
|
Mahadevan MM, Trounson AO, Leeton JF: The relationship of tubal blockage, infertility of unknown cause, suspected male infertility, and endometriosis to success of in vitro fertilization and embryo transfer. Fertil Steril 40: 755, 1983 |
|
Yovich JL, Yovich JM, Tuvik AI et al: In vitro fertilization for endometriosis. Lancet ii: 552, 1985 |
|
Grant A: Additional sterility factors in endometriosis. Fertil Steril 17: 514, 1966 |
|
Damewood MD, Hesla JS, Schlaff WD et al: Effect of serum from patients with minimal to mild endometriosis on mouse embryo development in vitro. Fertil Steril 54: 917, 1990 |
|
Taketani Y, Kuo T-M, Mizuno M: Tumor necrosis factor inhibits the development of mouse embryos co-cultured with oviducts: possible relevance to infertility associated with endometriosis. J Mamm Ovar Res 8: 175, 1991 |
|
Pittaway DE, Maxson W, Daniell J et al: Luteal phase defects in infertility patients with endometriosis. Fertil Steril 39: 712, 1983 |
|
Gilmore SM, Aksel S, Hoff C et al: In vitro lymphocyte activity in women with endometriosis – an altered immune response? Fertil Steril 58: 1148, 1992 |
|
Drake TS, Metz SA, Grunert GM, O'Brien WF: Peritoneal fluid volume in endometriosis. Fertil Steril 34: 280, 1980 |
|
Dunselman G, Hendrix M, Bouckaert P, Evers J: Functional aspects of peritoneal macrophages in endometriosis of women. J Reprod Fertil 82: 707, 1988 |
|
Haney A, Muscato J, Weinberg J: Peritoneal fluid cell populations in infertility patients. Fertil Steril 35: 696, 1981 |
|
Halme J, Becker S, Hammond M, Raj S: Pelvic macrophages in normal and infertile women: the role of patent tubes. Am J Obstet Gynecol 142: 890, 1982 |
|
Schenken RS, Asch RH, Williams RF, Hodgen GD: Etiology of infertility in monkeys with endometriosis: luteinized unruptured follicles, luteal phase defects, pelvic adhesions, and spontaneous abortions. Fertil Steril 41: 122, 1984 |
|
Schenken RS, Asch RH: Surgical induction of endometriosis in the rabbit: effects on fertility and concentrations of peritoneal fluid prostaglandins. Fertil Steril 34: 581, 1989 |
|
Kaplan CR, Eddy CA, Olive DL, Schenken RS: Effects of ovarian endometriosis on ovulation in rabbits. Am J Obstet Gynecol 160: 40, 1989 |
|
Dunselman GAJ, Dumoulin JCM, Land JA, Evers JLH: Lack of effect of peritoneal endometriosis on fertility in the rabbit model. Fertil Steril 56: 340, 1991 |
|
Chauhan M, Barratt CLR, Cooke SMS, Cooke ID: Differences in the fertility of donor insemination recipients—a study to provide prognostic guidelines as to its success and outcome. Fertil Steril 51: 815, 1989 |
|
Dunphy BC, Kay R, Barratt CLR, Cooke ID: Female age and the length of involuntary infertility prior to investigation and fertility outcome. Hum Reprod 4: 527, 1989 |
|
Jansen RPS: Minimal endometriosis and reduced fecundability; prospective evidence from an artificial insemination by donor program. Fertil Steril 46: 141, 1986 |
|
Soules MR, Malinak LR, Bury R, Poindexter A: Endometriosis and anovulation: a coexisting problem in the infertile female. Am J Obstet Gynecol 125: 412, 1976 |
|
Buttram VC Jr: Conservative surgery for endometriosis in the infertile female: a study of 206 patients with implications for both medical and surgical therapy. Fertil Steril 31: 117, 1979 |
|
Foster DC, Stern JL, Buscema J et al: Pleural and parenchymal pulmonary endometriosis. Obstet Gynecol 58: 552, 1981 |
|
Nezhat C, Seidman D, Nezhat F, Nezhat C: Laparoscopic surgical management of diaphragmatic endometriosis. Fertil Steril 69: 1048, 1998 |
|
Thibodeau LL, Prioleau GR, Manuelidis EE et al: Cerebral endometriosis: case report. J Neurosurg 66: 609, 1987 |
|
Denton RO, Sherrill JD: Sciatic syndrome due to endometriosis of sciatic nerve. South Med J 48: 1027, 1955 |
|
Gleicher N, Karande V, Rabin D et al: The bubble test: a new tool to improve the diagnosis of endometriosis. Hum Reprod 10: 923, 1995 |
|
Redwine DB: Peritoneal blood painting: an aid in the diagnosis of endometriosis. Am J Obstet Gynecol 161: 865, 1989 |
|
Hoeger KM, Guzick DS: Classification of endometriosis. Obstet Gynecol Clin North Am 24: 347, 1997 |
|
Friedman H, Vogelzang RL, Mendelson EB et al: Endometriosis detection by US with laparoscopic correlation. Radiology 157: 217, 1985 |
|
Guerriero S, Mais V, Ajossa S et al: The role of endovaginal ultrasound in differentiating endometriomas from other ovarian cysts. Clin Exp Obstet Gynecol 22: 20, 1995 |
|
Volpi E, De Grandis T, Zuccaro G et al: Role of transvaginal sonography in the detection of endometriomata. J Clin Ultrasound 23: 163, 1995 |
|
Athey PA, Diment DD: The spectrum of sonographic findings in endometriomas. J Ultrasound Med 8: 487, 1989 |
|
Kurjak A, Kupesic S: Scoring system for prediction of ovarian endometriosis based on transvaginal color and pulsed Doppler sonography. Fertil Steril 62: 81, 1994 |
|
Togashi K, Nishimura K, Kimura I et al: Endometrial cysts: diagnosis with MR imaging. Radiology 180: 73, 1991 |
|
Arrive L, Hricak H, Martin MC: Pelvic endometriosis: MR imaging. Radiology 171: 687, 1989 |
|
Mol BWJ, Bayram N, Lijmer JG et al: The performance of CA-125 measurement in the detection of endometriosis: a meta-analysis. Fertil Steril 70: 1101, 1998 |
|
Pittaway D, Fayez J: The use of CA-125 in the diagnosis and management of endometriosis. Fertil Steril 46: 790, 1986 |
|
Pittaway DE, Rondinone D, Miller KA et al: Clinical evaluation of CA-125 concentrations as prognostic factor for pregnancy in infertile women with surgically treated endometriosis. Fertil Steril 64: 321, 1995 |
|
Kauppila A, Telimaa S, Ronnberg L, Vucri J: Placebo-controlled study on serum concentrations of CA-125 before and after treatment of endometriosis with danazol or high-dose medroxyprogesterone acetate alone or after surgery. Fertil Steril 49: 37, 1988 |
|
Koninckx PR, Meuleman C, Oosterlynck D et al: Diagnosis of deep endometriosis by clinical examination during menstruation and plasma CA-125 concentration. Fertil Steril 65: 280, 1996 |
|
Koninckx PR, Muyldermans M, Moerman P et al: CA 125 concentrations in ovarian “chocolate” cyst fluid can differentiate an endometriotic cyst from a cystic corpus luteum. Hum Reprod 7: 1314, 1992 |
|
Koninckx PR, Riittinen L, Seppala M et al: CA-125 and placental protein 14 concentrations in plasma and peritoneal fluid of women with deeply infiltrating pelvic endometriosis. Fertil Steril 57: 523, 1992 |
|
Telimaa S, Kauppila A, Rönnberg L et al: Elevated serum levels of endometrial secretory protein PP14 in patients with advanced endometriosis: suppression by treatment with danazol and high-dose medroxyprogesterone. Am J Obstet Gynecol 161: 866, 1989 |
|
Wild RA, Hirisave V, Bianco A et al: Endometrial antibodies versus CA-125 for the detection of endometriosis. Fertil Steril 55: 90, 1991 |
|
Switchenko AC, Kauffman RS, Becker M: Are there antiendometrial antibodies in sera of women with endometriosis? Fertil Steril 56: 235, 1991 |
|
American Fertility Society: Classification of endometriosis. Fertil Steril 30:240, 1979 |
|
American Fertility Society: Revised American Fertility Society classification for endometriosis. Fertil Steril 43: 351,1986 |
|
Hoeger KM, Guzick DS: Classification of endometriosis. Obstet Gynecol Clin North Am 24: 347, 1997 |
|
Kauppila A, Puolakka J, Ylikorkala O: Prostaglandin biosynthesis inhibitors and endometriosis. Prostaglandins 18: 655, 1979 |
|
Hughes EG, Fedorkow DM, Collins JA: A quantitative overview of controlled trials in endometriosis-associated infertility. Fertil Steril 59: 963, 1993 |
|
Silverberg KM: Combination therapy for endometriosis. Infertil Reprod Med Clin North Am 3: 683, 1992 |
|
Telimaa S, Puolakka J, Ronnberg L, Kaupilla A: Placebo-controlled comparison of danazol and high-dose medroxyprogesterone acetate in the treatment of endometriosis. Gynecol Endocrinol 1: 13, 1987 |
|
Henzl MR, Corson SL, Moghissi K et al: Administration of nasal nafarelin as compared with oral danazol for endometriosis. N Engl J Med 318: 485, 1988 |
|
Bayer SR, Seibel M: Medical treatment: danazol. In Schenken RS (ed): Endometriosis: Contemporary Concepts in Clinical Management. Philadelphia: JB Lippincott, 1989 |
|
Schlaff WD, Dugoff L, Damewood MD, Rock JA: Megestrol acetate for treatment of endometriosis. Obstet Gynecol 75: 646, 1990 |
|
Coutinho EM, Husson JM, Azadian-Boulanger G: Treatment of endometriosis with gestrinone—five years' experience. In Raynaud J-P, Ojasoo T, Martini L (eds): Medical Management of Endometriosis. New York: Raven, 1984 |
|
Hornstein MD, Yuzpe A, Burry KA et al: Prospective randomized double-blind trial of three versus six months of nafarelin therapy for endometriosis-associated pelvic pain. Fertil Steril 63: 955, 1995 |
|
Fedele L, Bianchi S, Arcaini L et al: Buserelin versus danazol in the treatment of endometriosis-associated infertility. Am J Obstet Gynecol 161: 871, 1989 |
|
Andrews MC, Andrews WC, Strauss AF: Effects of progestin-induced pseudopregnancy on endometriosis: clinical and microscopic studies. Am J Obstet Gynecol 78: 776, 1959 |
|
Kistner RW: The treatment of endometriosis by inducing pseudopregnancy with ovarian hormones: a report of 58 cases. Fertil Steril 10: 539, 1959 |
|
Olive DL: Medical treatment: alternatives to danazol. In Schenken RS (ed): Endometriosis: Contemporary Concepts in Clinical Management. Philadelphia: JB Lippincott, 1989 |
|
Moghissi KS, Boyce CRK: Management of endometriosis with oral medroxyprogesterone acetate. Obstet Gynecol 47: 265, 1976 |
|
Telimaa S, Penttila I, Puolakka J et al: Circulating lipid and lipoprotein concentrations during danazol and high-dose medroxyprogesterone acetate therapy of endometriosis. Fertil Steril 52: 31, 1989 |
|
Hull ME, Moghissi KS, Magyar DF, Hayes MF: Comparison of different treatment modalities of endometriosis in infertile women. Fertil Steril 47: 40, 1987 |
|
Greenblatt RB, Dmowski WP, Mahesh VB et al: Clinical studies with an antigonadotropin—danazol. Fertil Steril 22: 102, 1971 |
|
Goebel R, Rjosk HK: Laboratory and clinical studies with the new antigonadotropin, danazol. Acta Endocrinol 85: 134, 1977 |
|
Floyd WS: Danazol: endocrine and endometrial effects. Int J Fertil 25: 75, 1980 |
|
Barbieri RL, Canich JA, Makris A, Todd RB: Danazol inhibits steroidogenesis. Fertil Steril 28: 809, 1977 |
|
McGinley R, Casey JH: Analysis of progesterone in unextracted serum: a method using danazol—a blocker of steroid binding to proteins. Steroids 33: 127, 1979 |
|
Chamness GC, Asch RH, Pauerstein CJ: Danazol binding and translocation of steroid receptors. Am J Obstet Gynecol 136: 426, 1980 |
|
Jenkin G, Cookson CI, Thorburn GD: The interaction of human endometrial and myometrial steroid receptors with danazol. Clin Endocrinol 19: 377, 1983 |
|
Tamaya T, Murakami T, Yamada T et al: Serum hormone and steroid hormone receptor levels during luteal phase and long-term treatment with danazol. Fertil Steril 40: 585, 1983 |
|
Buttram VC Jr, Belue JB, Reiter R: Interim report of a study of danazol for the treatment of endometriosis. Fertil Steril 37: 478, 1982 |
|
Wardle PG, Whitehead MI, Mill RP: Non-reversible and wide-ranging voice changes after treatment with danazol. Br Med J 287: 946, 1983 |
|
Holt JP, Keller D: Danazol treatment increases serum enzyme levels. Fertil Steril 41: 70, 1984 |
|
Pearson K, Zimmerman HJ: Danazol and liver damage. Lancet 2: 645, 1980 |
|
Haning RV, Carlson IH, Cortes J et al: Danazol and its principal metabolites interfere with binding of testosterone, cortisol, and thyroxine by plasma proteins. Clin Chem 28: 696, 1982 |
|
Fahraeus L, Larsson-Cohn U, Ljungberg S et al: Profound alterations of the lipoprotein metabolism during danazol treatment in premenopausal women. Fertil Steril 42: 52, 1984 |
|
Young MD, Blackmore WP: The use of danazol in the management of endometriosis. J Int Med Res 5: 86, 1977 |
|
Bayer SR, Seibel MM, Saffan DS et al: Efficacy of danazol treatment for minimal endometriosis in infertile women: a prospective, randomized study. J Reprod Med 33: 179, 1988 |
|
Barbieri RL, Evans S, Kistner RW: Danazol in the treatment of endometriosis: analysis of 100 cases with a 4-year follow-up. Fertil Steril 37: 737, 1982 |
|
Telimaa S: Danazol and medroxyprogesterone acetate inefficacious in the treatment of endometriosis associated with infertility. Fertil Steril 50: 872, 1988 |
|
Fedele L, Marchini M, Baglioni A et al: Evaluation of histological and ultrastructural aspects of endometrium during treatment with gestrinone in women with amenorrhea or spotting. Acta Obstet Gynecol Scand 69: 143, 1990 |
|
Kauppila A, Isomaa V, Vierikko P et al: Effect of gestrinone in endometriosis tissue and endometrium. Fertil Steril 44: 466, 1985 |
|
Fedele L, Bianchi S, Viezzoli T et al: Gestrinone versus danazol in the treatment of endometriosis. Fertil Steril 51: 781, 1989 |
|
Hornstein MD, Gleason RE, Barbieri RL: A randomized double-blind prospective trial of two doses of gestrinone in the treatment of endometriosis. Fertil Steril 53: 237, 1990 |
|
Thomas EJ, Cooke ID: Successful treatment of asymptomatic endometriosis: does it benefit infertile women? Br Med J 294: 1117, 1987 |
|
Meldrum DR, Chang RJ, Lu J, Vale W: “Medical oophorectomy” using a long-acting GnRH agonist—a possible new approach to the treatment of endometriosis. J Clin Endocrinol Metab 51: 1081, 1982 |
|
Johansen JS, Riis BJ, Hassager C et al: The effect of a gonadotropin-releasing hormone agonist analog (nafarelin) on bone metabolism. J Clin Endocrinol Metab 67: 701, 1988 |
|
Matta W, Shaw R, Hesp R et al: Reversible trabecular bone density loss following induced hypoestrogenism with the GnRH analogue buserelin in premenopausal women. Clin Endocrinol (Oxf) 29: 45, 1988 |
|
Shaw RW, Zoladex Endometriosis Study Team: An open, randomized comparative study of the effect of goserelin depot and danazol in the treatment of endometriosis. Fertil Steril 58:26, 1992 |
|
Dlugi AM, Miller JD, Knittle J: Lupron depot (leuprolide acetate for depot suspension) in the treatment of endometriosis: a randomized, placebo-controlled, double-blind study: Lupron Study Group. Fertil Steril 54: 419, 1990 |
|
The Nafarelin European Endometriosis Trial Group (NEET): Nafarelin for endometriosis: a large-scale, danazol-controlled trial of efficacy and safety, with 1-year follow-up. Fertil Steril 57:514, 1992 |
|
Wheeler JM, Knittle JD, Miller JD, Lupron Endometriosis Study Group: Depot leuprolide acetate versus danazol in the treatment of women with symptomatic endometriosis: a multicenter double-blind randomized clinical trial. I. Efficacy results. Am J Obstet Gynecol 167:1367, 1992 |
|
Gargiulo AR, Hornstein MD: The role of GnRH agonists plus add-back therapy in the treatment of endometriosis. Semin Reprod Endocrinol 15: 273, 1997 |
|
Surrey ES, Add-Back Consensus Working Group: Add-back therapy and gonadotropin releasing hormone agonists in the treatment of patients with endometriosis: can a consensus be reached? Fertil Steril 71:420, 1999 |
|
Surrey ES, Judd HL: Reduction of vasomotor symptoms and bone mineral density loss with combined norethindrone and long-acting gonadotropin-releasing hormone agonist therapy of symptomatic endometriosis: a prospective randomized trial. J Clin Endocrinol Metab 75: 558, 1992 |
|
Bruhat MA, Mage C, Chapron C et al: Present-day endoscopic surgery in gynecology. Eur J Obstet Gynecol Reprod Biol 41: 4, 1991 |
|
Carbon Dioxide Laser Laparoscopy Study Group: Initial report of the carbon dioxide laser laparoscopy study group: complications. J Gynecol Surg 5:269, 1989 |
|
Peterson HB, Hulka JF, Phillips JM: American Association of Gynecologic Laparoscopists' 1988 membership survey on operative laparoscopy. J Reprod Med 35: 584, 1990 |
|
Luciano AA, Manzi D: Treatment options for endometriosis: surgical therapies. Infertil Reprod Med Clin North Am 3: 657, 1992 |
|
Adamson GD: Laparoscopic treatment of endometriosis. In Adamson GD, Martin DC (eds): Endoscopic Management of Gynecologic Disease. Philadelphia: Lippincott-Raven Publishers, 1996 |
|
Buttram VC Jr: Conservative surgery for endometriosis in the infertile female: a study of 206 patients with implications for both medical and surgical therapy. Fertil Steril 31: 117, 1979 |
|
Gordts S, Boeckx W, Brosens I: Microsurgery of endometriosis in infertile patients. Fertil Steril 42: 520, 1991 |
|
Wheeler JM, Malinak LR: Recurrent endometriosis: incidence, management, and prognosis. Am J Obstet Gynecol 146: 247, 1983 |
|
Adamson GD, Pasta DJ: Surgical treatment of endometriosis-associated infertility: meta-analysis compared with survival analysis. Am J Obstet Gynecol 171: 1488, 1994 |
|
Marcoux S, Maheux R, Berube S et al: Laparoscopic surgery in infertile women with minimal or mild endometriosis. N Engl J Med 337: 217, 1997 |
|
Parazzini F: Ablation of lesions or no treatment in minimal-mild endometriosis in infertilewomen: a randomized trial. Gruppo Italiano per lo Studio dell'Endometriosi. Hum Reprod 1999 May;14(5):1332-4 |
|
: Endometriosis and infertility. Fertil Steril 2006 Nov;86(5 Suppl):S156-60 |
|
Wood C, Mabler P, Hill D: Diagnosis and surgical management of endometriomas. Aust N Z J Obstet Gynaecol 32: 161, 1992 |
|
Reich H, McGlynn F: Treatment of ovarian endometriomas using laparoscopic surgical techniques. J Reprod Med 31: 577, 1986 |
|
Adamson GD, Subak LL, Pasta DJ et al: Comparison of CO2 laser laparoscopy with laparotomy for treatment of endometriomata. Fertil Steril 57: 965, 1992 |
|
Canis M, Mage G, Wattiez A et al: Second-look laparoscopy after laparoscopic cystectomy of large ovarian endometriomas. Fertil Steril 58: 617, 1992 |
|
Pellicano M, Bramante S, Guida M et al: Ovarian endometrioma: postoperative adhesions following bipolar coagulation and suture. Fertil Steril 2008 Apr;89(4):796-9. Epub 2007 Oct 22 |
|
Fedele L, Bianchi S, Zanconato G et al: Bipolar electrocoagulation versus suture of solitary ovary after laparoscopic excision of ovarian endometriomas. J Am Assoc Gynecol Laparosc 2004 Aug;11(3):344-7 |
|
Sayegh R, Garcia CR: Ovarian function after conservational ovarian surgery: a long-term follow-up study. Int J Gynaecol Obstet 39: 303, 1992 |
|
Loh FH, Tan AT, Kumar J et al: Ovarian response after laparoscopic ovarian cystectomy for endometriotic cysts in 132 monitored cycles. Fertil Steril 1999 Aug;72(2):316-21 |
|
Reich H, McGlynn F, Salvat J: Laparoscopic treatment of cul-de-sac obliteration secondary to retrocervical deep fibrotic endometriosis. J Reprod Med 36: 516, 1991 |
|
Redwine DB: Treatment of endometriosis-associated pain. Infertil Reprod Med Clin Am 3: 697, 1994 |
|
Nezhat C, Hood J, Winer W et al: Videolaseroscopy and laser laparoscopy in gynaecology. Br J Hosp Med 38: 219, 1987 |
|
Sutton CJG, Ewen SP, Whitelaw N et al: Prospective, randomized, double-blind controls: trial of laser laparoscopy in the treatment of pelvic pain associated with minimal, mild and moderate endometriosis. Fertil Steril 62: 696, 1994 |
|
Candiani GB, Fedele L, Vercellini P et al: Repetitive conservative surgery for recurrence of endometriosis. Obstet Gynecol 77: 421, 1991 |
|
Cornillie FJ, Oosterlynck D, Lauweryns J et al: Deeply infiltrating pelvic endometriosis: histology and clinical significance. Fertil Steril 53: 978, 1993 |
|
Koninckx PR, Martin DC: Deep endometriosis: a consequence of infiltration or retraction or possibly adenomyosis externa? Fertil Steril 58: 924, 1992 |
|
Koninckx PR, Martin D: Treatment of deeply infiltrating endometriosis. Curr Opin Obstet Gynecol 6: 231, 1994 |
|
Donnez J, Nisolle M, Casanas-Roux F et al: Rectovaginal septum endometriosis or adenomyosis: laparoscopic management in a series of 231 patients. Hum Reprod 10: 630, 1995 |
|
Candiani GB, Vercellini P, Fedele L et al: Conservative surgical treatment of rectovaginal septum endometriosis. J Gynecol Surg 8: 177, 1992 |
|
Fayez JA, Vogel MF: Comparison of different treatment methods of endometriosis by laparoscopy. Obstet Gynecol 78: 660, 1991 |
|
Kojima E, Morita M, Otaka K et al: Nd:YAG laser laparoscopy for ovarian endometriomas. J Reprod Med 35: 592, 1990 |
|
Marrs RP: The use of potassium-titanyl-phosphate laser for laparoscopic removal of ovarian endometriomas. Am J Obstet Gynecol 164: 1622, 1991 |
|
Walters MD: Definitive surgery. In Schenken RS (ed): Endometriosis: Contemporary Concepts in Clinical Management. Philadelphia: JB Lippincott, 1989. |
|
Peters AA, Trimbos-Kemper GC, Admiral C et al: A randomized clinical trial on the benefit of adhesiolysis in patients with intraperitoneal adhesions and chronic pelvic pain. Br J Obstet Gynaecol 99: 50, 1992 |
|
Kresch AJ, Seifer DB, Sachs LB et al: Laparoscopy in 100 women with chronic pelvic pain. Obstet Gynecol 64: 672, 1984 |
|
Rapkin AJ: Adhesions and pelvic pain: a retrospective study. Obstet Gynecol 68: 13, 1986 |
|
Stout AL, Steege JF, Dodson WC et al: Relationship of laparoscopic findings to self-report of pelvic pain. Am J Obstet Gynecol 164: 73, 1991 |
|
Sutton C, MacDonald R: Laser laparoscopic adhesiolysis. J Gynecol Surg 6: 155, 1990 |
|
Goldstein DP, DeCholnoky C, Emans SJ et al: Laparoscopy in the diagnosis and management of pelvic pain in adolescents. J Reprod Med 24: 251, 1980 |
|
Steege JF, Stout AL: Resolution of chronic pelvic pain after laparoscopic lysis of adhesions. Am J Obstet Gynecol 165: 278, 1991 |
|
Operative Laparoscopy Study Group: Postoperative adhesion development following operative laparoscopy: evaluation at early second-look procedures. Fertil Steril 55: 700, 1991 |
|
Tjaden B, Schlaff WD, Kimball A et al: The efficacy of presacral neurectomy for the relief of midline dysmenorrhea. Obstet Gynecol 76: 89, 1990 |
|
Candiani GB, Fedele L, Vercellini P et al: Presacral neurectomy for the treatment of pelvic pain associated with endometriosis: a controlled study. Am J Obstet Gynecol 167: 100, 1992 |
|
Lichten EM, Bombard J: Surgical treatment of primary dysmenorrhea with laparoscopic uterine nerve ablation. J Reprod Med 32: 37, 1987 |
|
Fedele L, Bianchi S, Marchini M et al: Superovulation with human menopausal gonadotropins in the treatment of infertility associated with minimal or mild endometriosis: a controlled randomized study. Fertil Steril 58: 28, 1992 |
|
Tummon IS, Asher LJ, Martin JSB, Tulandi T: Randomized controlled trial of superovulation and insemination for infertility associated with minimal or mild endometriosis. Fertil Steril 68: 8, 1997 |
|
Guzick DS, Sullivan MW, Adamson GD et al: Efficacy of treatment for unexplained infertility. Fertil Steril 70: 207, 1998 |
|
Simon C, Gutierrez A, Vidal A et al: Outcome of patients with endometriosis in assisted reproduction: results from in vitro fertilization and oocyte donation. Hum Reprod 9: 725, 1994 |
|
Sharma V, Riddle A, Mason BA et al: An analysis of factors influencing the establishment of a clinical pregnancy in an ultrasound-based ambulatory in vitro fertilization program. Fertil Steril 49: 468, 1988 |
|
Azem F, Lessing JB, Geva E et al: Patients with stages III and IV endometriosis have a poorer outcome of in vitro Fertil Steril 1999 Dec;72(6):1107-9 |
|
Barnhart K, Dunsmoor-Su R, Coutifaris C: Effect of endometriosis on in vitro fertilization. Fertil Steril 2002 Jun;77(6):1148-55 |
|
Dmowski WP, Rana N, Michalowska J et al: The effect of endometriosis, its stage and activity, and of autoantibodies on in vitro fertilization and embryo transfer success rates. Fertil Steril 63: 555, 1995 |
|
Inoue M, Kobayashi Y, Honda I et al: The impact of endometriosis on the reproductive outcome of infertile patients. Am J Obstet Gynecol 167: 278, 1992 |
|
Surrey MW, Hill DL. Treatment of endometriosis by carbon dioxide laser during gamete intrafallopian tube transfer. J Am Coll Surg 179:440,1994 |
|
Kennedy S, Bergqvist A, Chapron C et al: ESHRE guideline for the diagnosis and treatment of endometriosis. Hum Reprod 2005 Oct;20(10):2698-704. Epub 2005 Jun 24 |
|
Marconi G, Vilela M, Quintana R et al: Laparoscopic ovarian cystectomy of endometriomas does not affect the ovarian response to gonadotropin stimulation. Fertil Steril 2002 Oct;78(4):876-8 |
|
Donnez J, Wyns C, Nisolle M: Does ovarian surgery for endometriomas impair the ovarian response togonadotropin? Fertil Steril 2001 Oct;76(4):662-5 |
|
Garcia-Velasco JA, Mahutte NG, Corona J et al: Removal of endometriomas before in vitro fertilization does not improve fertility Fertil Steril 2004 May;81(5):1194-7 |
|
Wong BC, Gillman NC, Oehninger S et al: Results of in vitro fertilization in patients with endometriomas: is surgicalremoval beneficial? Am J Obstet Gynecol 2004 Aug;191(2):597-606; discussion 606-7 |
|
Marcus SF, Edwards RG: High rates of pregnancy after long-term down-regulation of women with severe endometriosis. Am J Obstet Gynecol 171: 812, 1994 |