Gartner's Duct Cyst
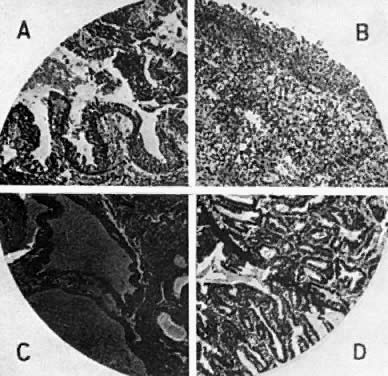
Gartner's duct cysts develop as a result of incomplete regression of the mesonephric or wolffian duct during fetal development (Fig. 1). In the male, these ducts form the epididymis. When present, these cysts may be multiple, and are located submucosally along the lateral aspects of the upper vagina. Histologic evaluation reveals nonsecretory, columnar epithelium. If these cysts are small, asymptomatic, and located in the lateral aspects of the upper vagina, no treatment is indicated. If the diagnosis is in question, or there is a history of antenatal exposure to synthetic hormones, adenosis of the vagina must be considered. The presence of mucosa, which stains normally with Lugol's solution, helps to exclude the diagnosis of adenosis. Regardless of size, biopsies should be performed on symptomatic cysts or they should be excised. Larger cysts in the vaginal fornix may extend to the lateral aspects of the cervix and require excision in the operating room.
|
Paramesonephric Duct Cyst
In contrast to Gartner's duct cysts, paramesonephric duct cysts are lined with secretory epithelium resembling endocervix or fallopian tube, suggesting mu¨llerian origin. These cysts may be found anywhere in the vagina and frequently contain mucus. Vaginal adenosis is excluded by staining with Lugol's solution. The diagnosis is established with an excisional biopsy if the cyst is large, symptomatic, or only recently identified.
Inclusion Cyst
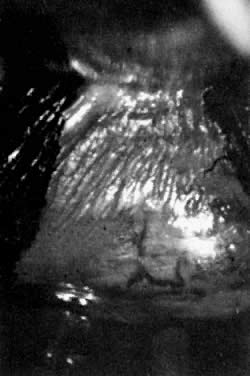
Inclusion cysts of the vagina result from mucosa trapped in the submucosal area by surgical procedures such as episiotomy, colporrhaphy, or trauma including childbirth (Fig. 2). As the cysts enlarge, symptoms may develop. These cysts are lined with squamous epithelium and contain keratin and squamous debris. Foreign-body reaction and inflammation surround the cyst. Treatment involves excision of the intact cyst and approximation of normal epithelium.
|
Endometriosis
Endometriosis in the vagina may develop at the site of a previous operation or as primary implants. Nodularity of the posterior vaginal fornix may represent endometriotic implants of the posterior cul-de-sac and may eventually erode or grow into the vaginal mucosa. When visualized colposcopically, these implants may appear dark blue or brown. If associated with fibrosis, the submucosal implants may appear white. Biopsy may yield chocolate-colored material representing old hemorrhage and dense fibrosis. Endometrial glands and stroma are usually identified histologically although the presence of both are not required to make the diagnosis. The diagnosis is made by biopsy unless endometriosis is identified in other parts of the pelvis. Small, symptomatic lesions are treated by excision or laser vaporization. Large lesions arising in the posterior cul-de-sac and extending into the posterior vaginal fornix may require laparotomy to accomplish excision. Preoperative therapy with gonadotropin releasing hormone analogs may greatly reduce the size of the implants, therefore, reducing the extent of excision or vaporization. We recommend outpatient mechanical bowel preparation prior to surgery. For the symptomatic patient who does not wish surgical excision of the lesion, gonadotropin releasing hormone analog therapy followed by suppression with oral contraceptives may be beneficial.