Dermatologic conditions of the vulva are responsible for a large number of gynecologic office visits. The vulvar skin is a frequent site of contact dermatitis produced by both primary irritants and allergic phenomena. The vulvar area may be irritated by local cosmetic or therapeutic agents, as well as by biological fluids such as urine or feces in cases of incontinence or difficult hygiene. Generalized skin conditions such as psoriasis, seborrheic dermatitis, and lichen planus may also have manifestations in the vulva and may be confused with other etiologies, such as candidiasis. These skin conditions may have a slightly different appearance on the vulva than in other areas of the body because of the moisture present. Steroid preparations are commonly used for these dermatologic conditions. In contact dermatitis the offending substance, if identified, is removed. Biopsy is recommended in any of these circumstances if the course is chronic or the precise etiology unclear.
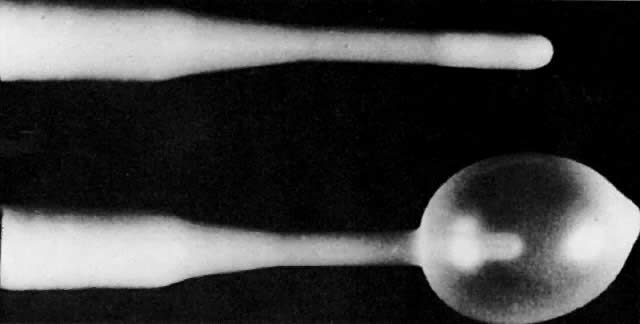
Biopsy of the vulvar skin is usually obtained with a Keyes biopsy punch. A simple alcohol preparation is sufficient with infiltration of local anesthetic, usually 1% lidocaine injected subepidermally with a 25-gauge needle. The addition of epinephrine promotes vasoconstriction and prolongs the anesthetic effect. The Keyes punch is available in diameters ranging from 2 to 5 mm, with 4- and 5-mm diameters most commonly employed for vulvar use. The site selected for biopsy should include tissue representative of the lesion or area of abnormality, but not necessarily the most central inflamed or necrotic area, which may give minimal tissue diagnosis because of the inflammation present. Therefore, the site picked is often at the periphery and may even include an edge of the lesion as it approaches the normal tissue. The cutting edge of the punch is applied to the surface (Fig. 1). With light pressure, the punch is rotated clockwise and counter clockwise, essentially drilling a hole through the full thickness of the skin. The specimen is then elevated with forceps and removed sharply from the underlying subcutaneous tissue. Hemostasis may be controlled with application of a silver nitrate stick to the site. Direct pressure may also be employed. Occasionally a suture of 3.0 chromic is required.
|
Intractable Pruritus
Some patients with benign dermatologic conditions have chronic pruritus that is not amenable to topical agents. This may be due to the inability of these drugs to penetrate the thickened, hyperkeratotic surface of the skin. In these instances a steroid injection into the subepithelial dermis may be appropriate. An injection of 20 to 30 mg (10 mg/mL) of triamcinolone acetonide (Kenalog) to a localized area is effective. The injected solution should be rubbed thoroughly into the tissue. Relief of symptoms may occur within 48 hours. Remissions may last for 4 to 6 months. Injections can be repeated for recurrent symptoms.
Local alcohol injections have also been employed, but require a general anesthetic. The entire vulvar area is marked off in a grid of 1-cm squares (Fig. 2). Absolute ethyl alcohol, 0.1 to 0.2 mL, is then injected into the subcutaneous tissue with a 25-gauge needle at each intersection of the lines, beginning at the lowest level of the grid.8 Care must be taken to avoid injection into the epithelium or into the deep subcutaneous tissue to avoid tissue necrosis and sloughing. Thin folds of the labia minora should be injected only at the bases. All areas should be fully massaged to facilitate even distribution. Localized edema is noted rapidly and is present for 2 to 3 weeks. Recurrent symptoms may require additional treatment. Most patients get at least enough relief so that their symptoms may be controlled with topical agents.
|
The Mering procedure may be employed if all other measures have failed to produce relief of symptoms.9 It involves blunt dissection through the subcutaneous tissue of the vulva to interrupt the branches of the ilioinguinal and genitofemoral nerves. The procedure requires a general or regional anesthetic. Incisions are made at the lateral margins of the labia majora, extending to the level of the clitoris superiorly and the anal orifice inferiorly (Fig. 3). The dissection is continued to the level of the fascia. The nerves in the adjacent tissue are disrupted bluntly, allowing the fingers in each incision to meet in the midline above and below the clitoris; blunt dissection proceeds posteriorly to meet in the perineum, and even around the rectum if symptoms are present in this area. This perianal disruption will also affect branches of the pudendal nerve. Hematoma formation and cellulitis are potential complications. A small drain is therefore placed in the most dependent portion of the incision. Both the underlying tissue and the skin edges are closed with absorbable suture. It is recommended that this area be treated with direct pressure for 24 hours, followed by ice packs.
|
Vulvar Vestibulitis
Vulvar vestibulitis is the most prevalent of the vulvar pain syndromes, or vulvodynia. It is a chronic condition for which no single etiology has been identified. It is characterized by inflammation localized to the vulvar vestibule, with dyspareunia as the most common complaint. The technique described for diagnosis includes probing the vestibule with a cotton-tipped applicator to map the area of burning and pain, which is often exquisite, thus mimicking the patient's symptoms. The area involved is nonkeratinized squamous epithelium containing mucous-secreting minor vestibular glands. These glands supply lubrication for coitus and may become inflamed due to edema, trauma, or infection. The examination reveals areas of bright erythema consistent with focal inflammation. Biopsy often shows a chronic inflammatory infiltrate with plasma cells. HPV has been demonstrated in some lesions by DNA hybridization techniques.10
Therapy has been directed toward treating any underlying infectious or dermatologic etiologies that may be aggravating these symptoms, as well as toward the use of topical anesthetic solutions or gels applied to the affected areas before coitus. Other therapies that have been reported as having some success in small series include acyclovir given over a 3-month period,11 intradermal injection of interferon alfa three times per week for 4 weeks,12 and low-dose 5-fluorouracil.13 Laser ablation has been successful in some cases.14 Surgical excision is considered for women whose symptoms have persisted for more than 6 months despite use of the therapies already mentioned. With vulvar vestibulectomy, 60% to 80% of women report significant pain relief. In performing the vestibulectomy with perineoplasty, the specific area of pain should be carefully delineated with a marking pen immediately before the administration of any anesthetic. The full epithelial thickness should be excised with inclusion of the adjacent hymen (Fig. 4). The posterior vaginal wall should be separated from the underlying tissue for 2 to 3 cm above the hymenal ring so that it may be pulled down and out to close the defect created. This vaginal mucosa is attached to the perineum with a mattress closure of interrupted absorbable suture.
|