The anatomy and histology of the female breasts are essentially the same as in the male until puberty. The development of the female breast (thelarche) usually begins approximately 3 years before the onset of menstruation (menarche). Commonly, thelarche begins at approximately age 11 and menarche at age 13. The breasts are usually fully developed by age 18. Multiple hormones (Table 1) act in balanced consort to mature the female breast and prepare for the physiologic function of lactation. Development of the breast stroma, growth of the ducts, and fat deposition are promoted primarily by estrogen. Lobular growth, alveolar budding, and alveolar secretory changes are promoted primarily by progesterone. However, the complete maturation of the ductal alveolar system requires both estrogen and progesterone acting in balanced consort.
During pregnancy, chorionic gonadotropin, placental lactogen, and prolactin stimulate the ductal alveolar system. Milk secretion and lactation require the consorted action of cortisol, growth hormone, oxytocin, parathyroid hormone, and thyroxine. Prolactin primarily regulates milk secretion and lactation after delivery.
Table 1. Essential Hormones for Female Breast Development
| Adrenal glucocorticoids |
| Estrogen |
| Growth hormone |
| Insulin |
| Progesterone |
| Prolactin |
Particularly during a menstrual cycle, the ductal and alveolar epithelial cells undergo replication and programmed physiologic cell death (apoptosis), although these processes are not uniform throughout the ductal alveolar systems. Ductal mitotic activity is reported to be prominent during the late luteal phase of the menstrual cycle, when progesterone is relatively dominant.1,2
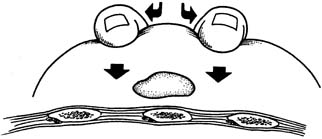
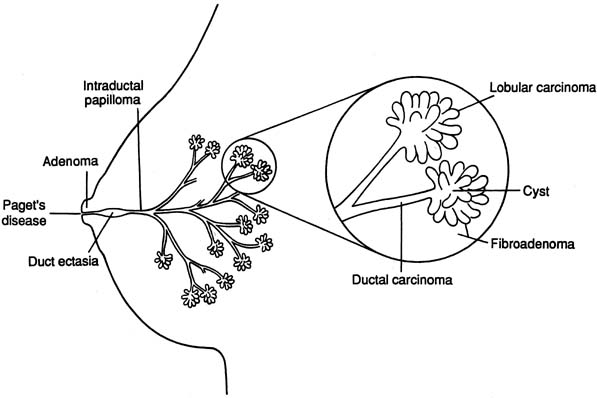
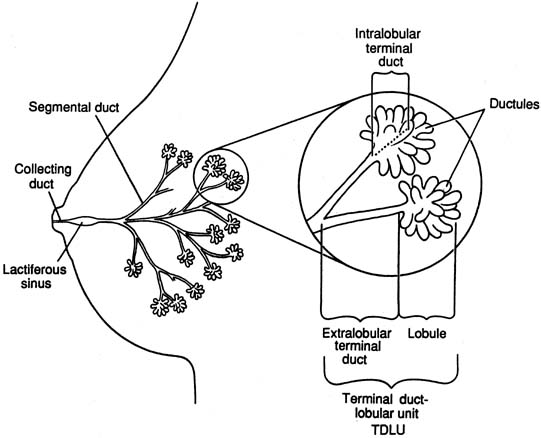
The diagrammatic representation of a single lobe and terminal duct lobular units is depicted in Figure 1. The common sites of breast pathology are depicted on a similar diagram in Figure 2. Although traditionally the breast is described as containing 12 to 15 distinct lobes, observation reveals that there are usually approximately six openings onto the nipple (galactophores), as some of the lobes join at the level of the collecting duct or even into the lactiferous sinus. Otherwise, there is no direct anatomical connection between the various lobes.
|
|
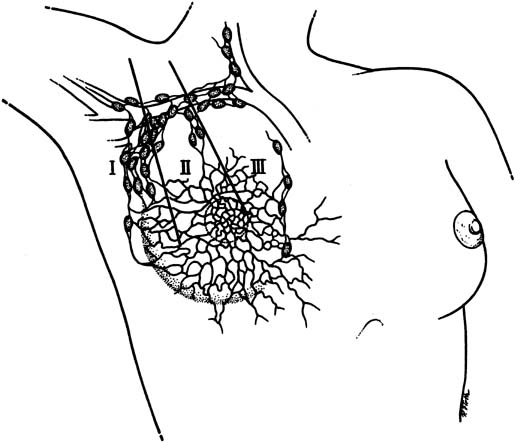
The lymphatic drainage of the breast is primarily to the axillary lymph nodes (Fig. 3), which are usually the initial site of detectable breast cancer metastases. In surgical anatomy, the axillary lymph nodes are described as: level I, lateral to the pectoralis minor muscle; level II, under the insertion of the pectoralis minor; and level III, medial to the pectoralis minor. In current surgical practice, axillary lymph node dissection for breast cancer calls for the removal of the level I and level II nodes.
|
The bulk of the breast is adipose tissue, regardless of the size of the breast. There is no correlation between breast size and breast cancer risk. The lobes develop in a random branching pattern similar to the spreading branches of a tree. Beginning at approximately during the age of mid 20 years, there is progressive diminution of the fibroglandular tissue in the breast and the adipose tissue becomes more prominent. Mammography becomes more effective as a woman's age advances because of the contrast of an abnormal mass to the surrounding adipose tissue.
Major developmental breast abnormalities (Table 2) are rare and do not respond to hormone therapy. If the patient or her mother insists on treatment, referral to a breast plastic surgeon is appropriate. Supernumerary nipples and ectopic breast tissue can occur along the embryologic milk line. The most common location is in the axillae.
Table 2. Congenital and Developmental Breast Abnormalities
| Accessory axillary breast tissue: ectopic breast tissue, usually bilateral and often symptomatic with pregnancy |
| Amastia: absence of one or both breasts |
| Delayed thelarche: no breast development by age 15 |
| Macromastia (gigantomastia): grossly enlarged breasts occurring with pregnancy or drug-induced |
| Juvenile hypertrophy: excessively enlarged breasts, usually bilateral |
| Poland syndrome: absence of the breasts, pectoralis muscles, and shoulder girdle; upper limb malformations |
| Polymastia: supernumerary breast |
| Polythelia: supernumerary nipples |
| Symmastia: midline confluence or webbing |
Source: Adapted from Hindle and Pan,1 with permission.