Carbon dioxide lasers were first used by Bellina and associates in 1974 for
intra-abdominal applications.27 By adapting the laser to the operating microscope, reconstructive microsurgical
procedures, including salpingolysis, salpingostomy, fimbrioplasty, and
treatment of endometriosis, were possible. With improvement
in technology and increased experience performing laparoscopic procedures, the
use of the laser for laparotomy has been replaced by an endoscopic
approach. Laparoscopy Instrumentation and Lasers The CO2 laser is the laser most commonly used in gynecologic surgery, for both
extra- and intra-abdominal applications. It has the advantage of causing
little peripheral thermal damage, usually less than 1 mm, and what
is seen in penetration is the true end result. Thus, it can be used in
critical areas adjacent to bowel, ureter, and bladder. CO2 lasers can be used to vaporize, excise, or coagulate tissue by modifying
the power density. The CO2 laser beam can be directed by a handpiece when used in laparotomy or, alternatively, through
a first or second puncture when used in laparoscopy (Fig. 26). 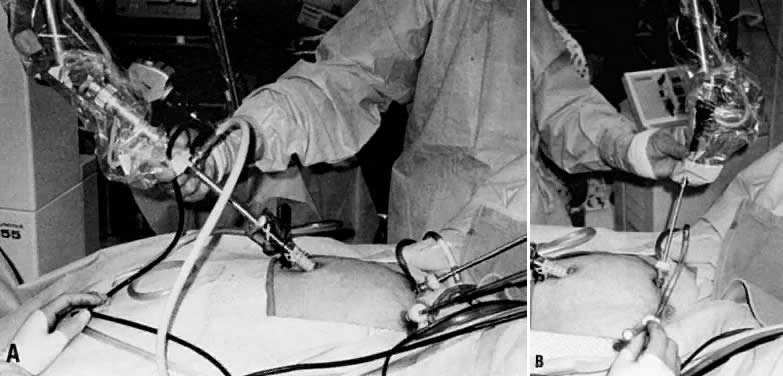 Fig. 26. A. First puncture laser use. B. Second puncture use. (Courtesy of Providence Hospital) Fig. 26. A. First puncture laser use. B. Second puncture use. (Courtesy of Providence Hospital)
|
The CO2 laser can be easily coupled to an operating laparoscope. The laser beam
should be aligned so that it lies in the middle of the viewing lens, and
it should be finely focused. A second or third puncture is necessary
only to manipulate pelvic structures, to clear the field of plume
production, or for irrigation purposes. It is also possible to use the
CO2 laser for second punctures by using wave guides that attach directly to
the CO2 laser and allow some flexibility in delivering the laser energy. Research
in developing a truly flexible fiber to deliver CO2 laser energy is still needed. At present, fiber systems used in intra-abdominal
laparoscopic surgery include primarily KTP, Nd:YAG, and argon
lasers. An advantage of the lasers using flexible delivery systems is that they
allow tactile contact with the tissue. Because each of these lasers has
a different wavelength and different absorption properties, it is important
to recognize their tissue interaction effects before they are
selected for surgery. The KTP and argon lasers share very similar wavelengths (532 μm versus 0.458 μm–0.515 μm) and thus produce similar tissue effects. The
energy produced is selectively absorbed by tissue containing
hemoglobin or is heavily pigmented. By moving the fibers closer or farther
away from the tissue, one can achieve cutting, vaporization, or coagulation
effects on tissue. The main drawback of these lasers is the
required use of goggles for eye protection, which distorts color discrimination. Although the Nd:YAG laser was originally used in gynecology primarily for
hysteroscopic application, it is now possible to use it solely intra-abdominally
by the use of contact sapphire probes or specially made
sculptured tips. These probes provide a tactile feel of the tissue, and
by selecting a variety of probes, one can incise, excise, vaporize, or
coagulate tissue. All of these lasers have been shown to be effective in the treatment of
various gynecologic conditions, including: Endometriosis
Laser uterosacral nerve ablation
Adhesiolysis
Neosalpingostomy
Fimbrioplasty
Ectopic pregnancy
Uterine fibroids
Endometriosis Areas of endometriosis can be vaporized or excised with the CO2 laser depending on the depth of penetration of the lesion. Superficial
areas of endometriosis in the cul-de-sac, uterosacral areas, or peritoneum
in general can be vaporized with wattages of 10 W to 20 W with spot
sizes of 1 mm. With lesions larger than 5 mm, it is recommended that
the surgeon cut through a healthy margin of the peritoneum and totally
excise the lesion. This scalpel effect can also be accomplished with
flexible laser fibers, as well as with electrosurgery and scissors. In
addition, the wavelengths of the argon and KTP lasers have an affinity
for pigmented lesions such as endometriosis, and these lasers have
been used extensively and effectively by Keye and Dixon to heat and
vaporize these lesions.28 The CO2 laser, however, remains the most commonly used laser and is the method
of choice for treating American Fertility Society (AFS) stage I to IV
endometriosis. The main reason is its high margin of safety, which is
due to its limited peripheral tissue injury and penetration. This makes
it ideal for adhesion excision near ureters and bowel. Although the
CO2 laser is ideal for surgical treatment of endometriosis, it does not offer
an increased pregnancy rate over other options, including sharp dissection
with scissors or electrosurgery.29 Reported pregnancy rates after laser treatment of endometriosis are 57%, 53%, and 61% for
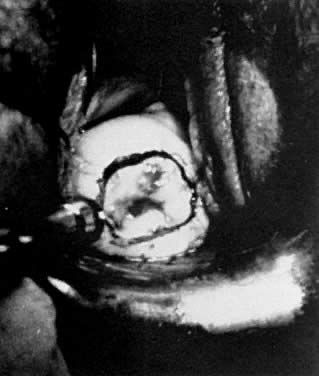
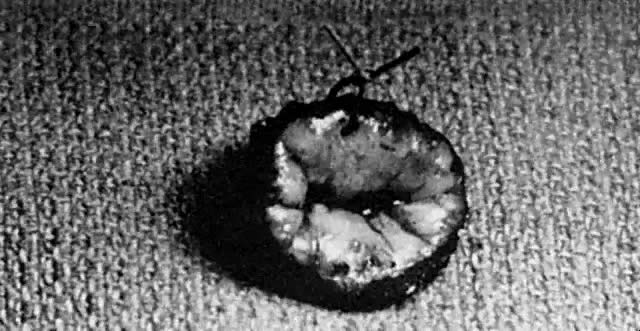
mild, moderate, and severe disease, respectively.30 Endometriomas can also be effectively treated with the CO2 laser. Initially, a small opening on the cyst wall is made to allow for
aspiration of the chocolate contents and profuse irrigation with a 5-mm
aspirator probe. The edge of the endometrioma and normal ovarian cortex
are then grasped individually with atraumatic forceps. With the
CO2 laser used intermittently at 10 W to 20 W, and with traction and countertraction
of the forceps holding the ovarian cortex and endometrium cyst
wall, the cyst can be stripped off. Removal of the cyst wall may be
in several portions. The base of the ovary after removal of the cyst
wall can then be ablated by defocusing the beam and decreasing to 10 W
of energy. This causes coagulation of small areas of oozing and destroys
any small areas of cyst wall that may remain. Patients with endometriosis who suffer from significant dysmenorrhea are
also candidates for laparoscopic uterosacral nerve ablation. This controversial
procedure was originally described by Doyle in 1963 and refers
to the denervation of sensory fibers in the lower uterine segment.31 The CO2 laser is used to vaporize a lesion 1 cm in diameter by 1 cm in depth at
the junction of the uterosacral ligaments to the posterior cervix. A
comparison between the CO2 laser and electrosurgery for treatment of dysmenorrhea revealed a 50% relief
of pain from both procedures.32 Adhesiolysis Pelvic adhesions are common sequelae to previous pelvic infections and
pelvic surgery. Although adhesiolysis is commonly performed with scissors
or electrosurgery, the laser is another option and represents an ideal
instrument for lysis of vascular adhesions, because excision and
coagulation can be performed simultaneously while limiting peripheral
tissue trauma. The use of graspers to apply tension on the adhesions maximizes
the efficiency of the laser (Fig. 27). The use of quartz rods, rods with backstops, and irrigation is recommended
to avoid injury to adjacent normal tissue. The pregnancy rate outcome
with the laser, however, does not significantly differ from that
with other standard modalities used to treat adhesions.33  Fig. 27. Adhesiolysis with CO2 laser. Fig. 27. Adhesiolysis with CO2 laser.
|
Salpingostomy Correction of distal tubal obstruction by cuff salpingostomy was first
reported in 1884 by Schroeder.34 Because of the dismal pregnancy rate, this procedure did not become popular
until principles of microsurgery were emphasized. Despite improvements
in surgical technique, pregnancy results remained low and dependent
on the extent of tubal disease at the time of surgery. With mild
disease there is a small (< 15 mm) enlargement of the distal tube, fimbriae
are inverted but recognized when patency is achieved, there is
a paucity of peritubal adhesions, and a rugal pattern is evident by
hysterosalpingogram (HSG). In moderate disease there is a distended tube (15 mm—30 mm
in size), fimbriae are not identified, and a rugal
pattern on HSG is not evident. With severe disease, a large (> 30 mm) hydrosalpinx
is present, no fimbriae are present, and there are
dense pelvic adhesions. The pregnancy rate is 30% to 40%, 10% to 30%, and 0% to 5% for
mild, moderate, and severe disease, respectively.35,36 In the eighties, our technology improved with the use of operative laparoscopy
and the use of lasers. Laser salpingostomy is routinely performed, with
pregnancy rates similar to those with the laparotomy approach. Treatment of distal tubal blockage begins with lysis of peritubal and ovarian
adhesions until the fallopian tube is completely free and movable. The
obstructed end of the tube can be assessed for diameter, presence
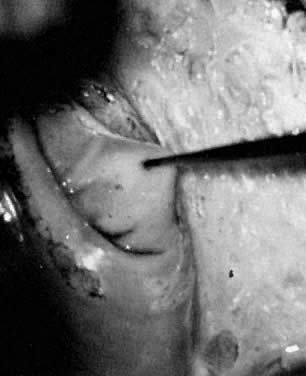
or absence of fimbriae, and patency. With the CO2 laser at 30 W, two linear incisions in the form of a cross are made in
the distal obstructed end of the tube (Fig. 28). It is recommended that the incision begin on the area where the tube
finally closed, because this is the thinnest and most avascular area. Continuous
dye injection helps to keep the distal tube distended while
the incision is being performed. The edges can then be everted by defocusing
the beam on the serosal edges and lowering the energy to 5 W
to 10 W. Continuous irrigation is applied during the procedure. The pregnancy
rate with the laparoscopic laser technique is not superior to
that with the standard microsurgery technique, and patients remain at
risk for ectopic pregnancy.  Fig. 28. Salpingostomy with CO2 laser. Fig. 28. Salpingostomy with CO2 laser.
|
In contrast to the low pregnancy rate with neosalpingostomy, fimbrioplasty
offers much better results in the 30% to 60% range37 because of the limited mucosal damage in these patients. In performing
fimbrioplasty, the CO2 laser is used in a continuous mode with 15 W to 20 W of energy, with a
backstop and irrigation used as needed. With a spot size of 0.5 mm, the
adhesions are easily removed by vaporization. Ectopic Pregnancy A conservative procedure for ectopic pregnancy was first reported by Stromme
in the English literature in 1953.38 This procedure did not become very popular until De Cherney and colleagues
in the early eighties published their success in treating unruptured
ectopic pregnancies.39 Laparoscopic treatment of ectopic pregnancy was reported in the mid-eighties
with a CO2 laser incision on the antimesenteric border of the tube.40 Paulson reported the treatment of 125 consecutive patients with ectopic
pregnancy.41 Laparoscopy was successful in all but four patients who needed laparotomy. The
CO2 laser offers another alternative to electrosurgery and scissors in the
treatment of ectopic pregnancy by laparoscopy. A linear incision is made
on the antimesenteric side of the tube over the dilated portion of
the ectopic pregnancy using 30 W of energy with a finely focused beam (Fig. 29). A dilute concentration of vasopressin can be injected into the mesosalpinx
below the ectopic tissue and on the serosa overlying the ectopic
pregnancy to decrease intraoperative bleeding. With the use of hydrodissection, the
ectopic tissue is then gently lifted from its tubal bed. Small
amounts of vascular oozing can be controlled with the laser, or
alternatively with bipolar forceps. The tubal lumen does not have to
be closed because fistula formation has not proved to be a problem. Results
of treatment of ectopic pregnancies with use of the laser do not
differ from those found with the conventional use of scissors or electrocautery.  Fig. 29. Laparoscopic laser removal of ectopic pregnancy. Fig. 29. Laparoscopic laser removal of ectopic pregnancy.
|
Uterine Fibroids Uterine leiomyomas are extremely common benign smooth muscle tumors occurring
in 25% of women older than 30 years of age.42 Although most women are asymptomatic, at least 25% of women have complaints
of pain, pressure, abnormal bleeding, urinary frequency, constipation, and
bloating. Recurrent abortion and infertility can also be linked
to large intramural and submucous fibroids, and surgery is indicated
only after a complete infertility evaluation has been performed and
all other factors are excluded. The laparoscopic approach is recommended only for pedunculated and subserosal
fibroids. Intramural myomectomies result in poor laparoscopic closure
with the potential for future uterine rupture during pregnancy.43 Laser energy can be delivered through a handpiece for laparotomies or via
the laparoscope. Small fibroids can be vaporized directly with 20 W
to 30 W of energy or can be shelled out in their entirety, as during
conventional surgery. Dilute vasopressin (1:30) is frequently used to
decrease intraoperative bleeding. Although the laser is capable of coagulation, it
is necessary to suture or coagulate larger vessels (greater
than 0.5 mm) with a bovie. Large intramural defects are closed with3-0 Dexon
sutures for the muscularis, followed by 4-0 Dexon for the serosa. The advantages of the CO2 laser for removal of uterine fibroids over scissors and standard electrosurgery
are improved hemostasis, decreased tissue trauma, and decreased
severity of adhesion formation. Approximately 50% to 60% of patients
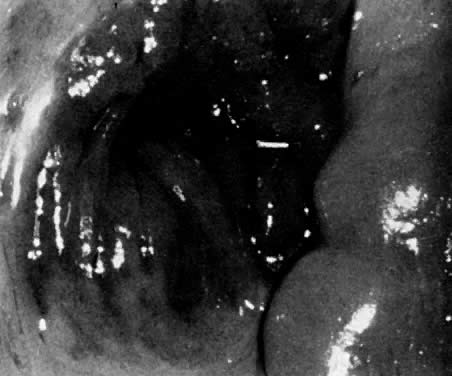
ultimately achieve pregnancy with laser myomectomy.44 Ovarian Wedge Resection Ovarian wedge resection by laparotomy, once a popular treatment option
for patients resistant to clomiphene citrate, is now rarely performed
because of the development of severe postoperative adhesions. However, with
strict adherence to microsurgical technique and the use of fine
electrocautery needle tips or lasers, it is possible to perform ovarian
wedge resection with pregnancy rates of 40%, which may be due to less
adhesion formation.45 Once the ovaries are exposed, they are draped with moist sponges. With 30 W
of energy, a focused beam of 0.5 mm can be used as a scalpel to remove
a wedge of the ovary. The use of hooks to retract the ovarian tissue
is helpful because tension on the tissue that is being incised expedites
the surgery. The ovarian defect is then closed with 3-0 Dexon
interrupted sutures, and 6-0 nylon is used for the cortical layer. To achieve the same endocrinologic effect of lower ovarian androgen levels
and ovulation that occurs with laparotomy, laparoscopic electrocoagulation
or laser coagulation of the ovary can be performed. In this technique, either
each ovary is cauterized with a unipolar needle electrode, or
laser energy is applied in multiple areas, causing small ovarian
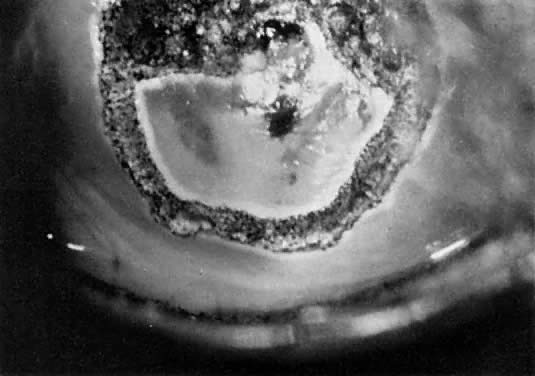
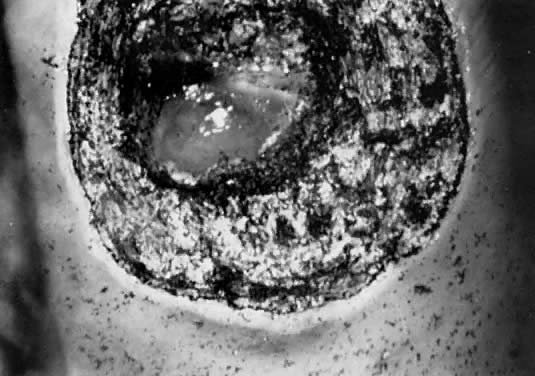
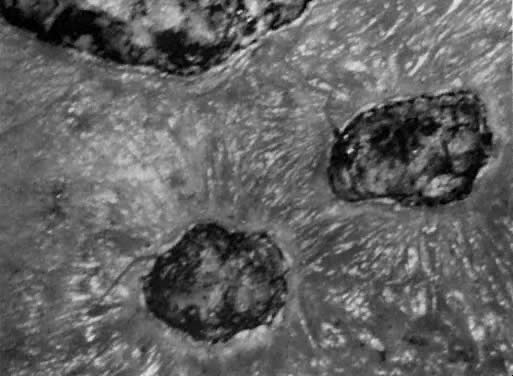
craters (Fig. 30). The CO2, KTP, argon, and Nd:YAG lasers have been used to treat polycystic ovaries
with ovulation rates of 70% and pregnancy rates of 40%.45 The endocrinologic effect of this procedure is temporary and rarely exceeds 12 months.  Fig. 30. Ovarian wedge craters produced by CO2 laser. Fig. 30. Ovarian wedge craters produced by CO2 laser.
|
Laser Hysteroscopy The hysteroscope has been used for many years as a diagnostic instrument
to evaluate the source of abnormal uterine bleeding. With refinement
of light sources, the use of low-viscosity fluids, and newer operating
hysteroscopes, it is now possible to use this technology as a therapeutic
modality for patients with abnormal uterine bleeding. Various instruments
can be used with the hysteroscope, including electrodes to cut
and coagulate, operating graspers, scissors, as well as various laser
fibers. The main laser delivery systems available for hysteroscopy
are the Nd:YAG and KTP 532. Both of these lasers use a flexible fiber
that can be passed easily through the operating sleeve of the hysteroscope. The
fiber can be directed by use of an Albarrán's bridge
that is attached to the operating hysteroscope. Hysteroscopic procedures
that can be accomplished with the laser include removal of fibroids
and polyps, transsection of uterine septa, lysis of adhesions, and
endometrial ablation. Endometrial Ablation Hysterectomy is the most common major operation performed in women, with 591,000 of
these procedures reported in 1990 by the Department of Health
and Human Services.46 Although there are many indications for hysterectomy, dysfunctional uterine
bleeding is the indication given in as many as half of these procedures
when there is no organic cause.47 An alternative to hysterectomy to treat dysfunctional uterine bleeding, unresponsive
to medical therapy, is endometrial ablation, which was
first reported by Goldrath and associates in 1981.48 The purpose of an endometrial ablation is to destroy the entire endometrium
and avoid future regeneration and menstrual bleeding. Patients are
initially pretreated with a gonadotropin-releasing hormone (GnRH) agonist
or danazol for a period of 4 weeks to decrease the endometrial thickness
to that seen in the menopausal state, thus facilitating the penetration
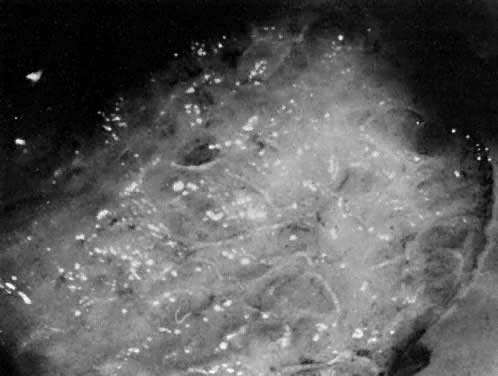
of the energy to the level of the myometrium. After adequate visualization of the entire uterine cavity, the laser fiber
can be inserted through the operating channel of the hysteroscope. The
Nd:YAG fiber can be used as either a touch or nontouch technique. With
the touch technique, the laser fiber is activated with 40 W to 50 W
of energy and dragged on the endometrial surface beginning on the
fundus and traveling down toward the endocervix in successive strokes (Fig. 31). This is done in a systematic way so that the entire surface is eventually
covered. With the nontouch or blanching technique, the laser fiber
is placed a few millimeters away from the endometrial surface while
the laser energy is activated. Of the two methods, the touch technique
is preferred because penetration is deeper, extending 4 mm to 6 mm into
the uterine wall. This depth is sufficient for destruction of the
endometrium.49  Fig. 31. Endometrial ablation with Nd:YAG laser fiber. Fig. 31. Endometrial ablation with Nd:YAG laser fiber.
|
Patients requesting endometrial ablation as a treatment for dysfunctional
uterine bleeding should understand that amenorrhea is possible only
in 50% to 65% of patients, whereas oligomenorrhea is observed in 25% to 30% and
no response to treatment is observed in 10% to 15% of patients. Endometrial ablation with the resectoscope using the roller ball technique
is an alternative to using the laser technique. Laser Excisional Hysteroscopic Procedures In addition to endometrial ablation, the laser can be used via hysteroscopy
for removal of submucous myomas and polyps, transsection of uterine
septa, and lysis of intrauterine adhesions. By using the laser fiber
as a scalpel with the touch technique, the tissue to be removed can
be morcellated and later removed with polyp forceps or a curette (Fig. 32). The advantage of the laser over scissors is that simultaneous coagulation
can be accomplished. Media used for distention do not have to be
free of electrolytes because electrical energy is not being used.  Fig. 32. A and B. Submucous laser myomectomy. Fig. 32. A and B. Submucous laser myomectomy.
|
Myomas larger than 4 cm can be pretreated with GnRH agonists to decrease
the size of the tumor, allow better visualization of the cavity, and
decrease presurgical uterine bleeding. An alternative instrument to scissors
and laser for removal of myomas is the resectoscope, which is
now the preferred method. Although the laser could be used for removal of polyps, these are usually
of very soft consistency and are easily removed with hysteroscopic
scissors. The laser should be reserved for larger myomatous lesions, where
use of the instrument is more efficient and cost-effective. Septate Uterus The uterine septum is one of several congenital uterine abnormalities that
arise from incomplete resorption of the müllerian ducts, and
it occurs in approximately 1% to 3.5% of women.50 The uterine septum is commonly associated with habitual miscarriage and
is transmitted as a polygenic or multifactorial pattern of inheritance. Diagnosis
of a septate uterus is made by both hysterosalpingogram
and diagnostic laparoscopy. This will exclude the possibility of an arcuate
or bicornuate uterus, which does not necessitate surgical intervention. Resection of a uterine septum can be performed with various instruments, including
scissors, resectoscope, and Nd:YAG laser. Operative hysteroscopy
is performed in conjunction with laparoscopy. This allows a more
uniform depth of incision throughout the septum and warns the operator
when a perforation is imminent. The Nd:YAG laser fiber is usually set at 40 W and used by the touch technique, as
if one were using a scalpel. The laser tip must be oriented
so that it incises the septum at the midline and does not deviate from
this line of incision (Fig. 33). This will ensure a relatively bloodless field of incision and avoids
injury to the myometrium. The laser incision is continued until there
is uniformity in light transmission throughout the fundus as observed
by laparoscopy, or until bleeding from the fundal myometrium is visualized. The
advantage of the laser fiber technique over the scissor technique
is primarily one of diminished bleeding. The procedure usually
takes 20 to 30 minutes, with gratifying results such as a 70% to 80% delivery
rate, and it is similar to the more classic Tomkin's and
Jones' intra-abdominal approach to metroplasty. The main advantages of
operative hysteroscopy compared with the abdominal approach include quickness
of surgery, minimal blood loss, no abdominal or uterine scar, minimal
morbidity, no reduction in intrauterine volume, and diminished
costs. In addition, patients are allowed to deliver vaginally.  Fig. 33. A and B. Uterine septum treated with Nd:YAG laser. Fig. 33. A and B. Uterine septum treated with Nd:YAG laser.
|
Intrauterine Adhesions Lysis of intrauterine adhesions can be readily accomplished with the Nd:YAG
laser. Unlike curettage, with hysteroscopy one can selectively cut
the scar tissue, limiting trauma to surrounding normal tissue. An IUD
or pediatric Foley catheter is left in the cavity for a few weeks while
the patient takes exogenous estrogens and antibiotics. Complications with Hysteroscopic Laser Complications inherent to hysteroscopy include uterine perforation, bleeding, fluid
overload, and, very rarely, infection. The use of a sapphire
tip with the Nd:YAG laser is contraindicated because its use with
CO2 gas for cooling has been implicated in several deaths due to gas emboli. |