The causative organism of endemic trachoma, inclusion conjunctivitis, lymphogranuloma venereum, urethritis, and cervicitis has been the subject of much medical literature in recent years. Only since 1965 has there been a relatively reliable, easily performed isolation technique, namely, tissue culture.1 Since that laboratory breakthrough, profuse data have been generated about human disease caused by Chlamydia trachomatis, as well as human and avian disease caused by C. psittaci, the agent of psittacosis. Because of the impact of C. trachomatis as a cause of pelvic inflammatory disease (PID), perhaps the largest portion of recent literature has concerned the urogenital chlamydial syndromes.
Bacteriology
The chlamydiae are obligate intracellular parasites of eukaryotic cells because of their inability to synthesize adenosine triphosphate (ATP). At one time they were considered viruses and given various generic names, including Bedsonia, Miyagawanella, and TRIC agent (trachoma-inclusion conjunctivitis). These organisms are now considered prokaryotic in nature--a special type of bacteria. They are known to have both deoxyribonucleic acid (DNA) and ribonucleic acid (RNA), have a cell wall that stains negatively on Gram stain, divide by binary fission, and be susceptible to antibiotics.
The order Chlamydiales consists of one family, Chlamydiaceae, which is made up of only one genus, Chlamydia. The two species, C. trachomatis and C. psittaci, are differentiated by sensitivity to sulfonamides and production of glycogen (C. trachomatis only).2
C. trachomatis may be separated into multiple serotypes by microimmunofluorescence techniques. Serotypes A, B, Ba, and C cause the syndrome of endemic trachoma. Serotypes D, E, F, G, H, I, J, and K cause neonatal conjunctivitis, neonatal pneumonitis, and a variety of sexually transmitted syndromes (cervicitis, urethritis, epididymitis). Finally, serotypes L1, L2, and L3 cause the venereal disease lymphogranuloma venereum (LGV).3
Although examination of Giemsa-stained scrapings of clinical materials was used successfully for diagnostic purposes in cases of chlamydial conjunctivitis, cell-culture methods are necessary in the urogenital syndromes. Microimmunofluorescent antibody titer studies may also be used.4 However, this method is difficult because the disease may be chronic, so the traditional “acute-and-convalescent” method of titers may be undependable.
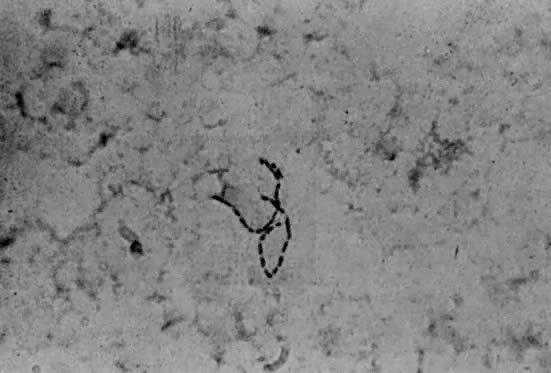
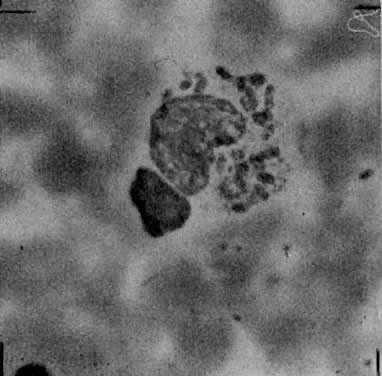
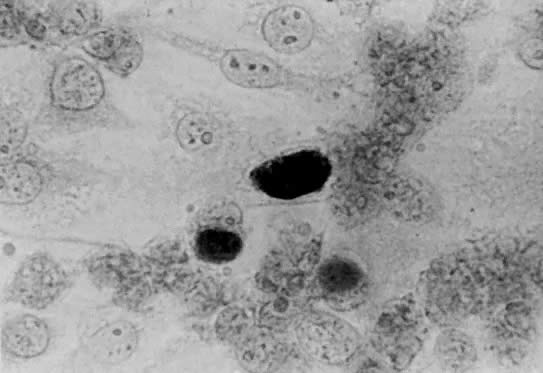
Both LGV and non-LGV strains of chlamydia may be grown in McCoy cells, a heterophile mouse cell-culture line. These cells are first inhibited by irradiation or with 5-iodo-2-deoxyuridine, permitting the chlamydia to more easily compete for cell nutrients. This allows easier recognition of intracytoplasmic inclusions after staining with iodine (Fig. 1).5
|
Since the diagnosis of conjunctival chlamydial infection was at one time made primarily on the basis of cytologic scrapings, investigators have tried to correlate the Papanicolaou smear with urogenital infection, especially of the cervix. Some researchers believe that intracytoplasmic coccoid and inclusion bodies in dysplastic exfoliated cells :are characteristic of chlamydial infection.6 Others have contradicted this claim, finding no regular morphologic features in chlamydia-infected specimens except for nonspecific inflammatory and dysplastic changes.7 The question remains unsettled, although individual cytologists are occasionally confident enough to read a routine smear as “changes suggestive of chlamydial infection.”
Clinical Features
C. trachomatis is causative, or at least implicated, in a variety of human disease syndromes, which are listed below:
Nongonococcal urethritis
Postgonococcal urethritis
Acute urethral syndrome
Acute salpingitis
Chronic salpingitis
Postabortal pelvic infection
Post-cesarean section infection
Endemic trachoma
Neonatal conjunctivitis
Neonatal pneumonia
Abortion
Stillbirth
Prematurity
“Late” postpartum endometritis
Reiter's syndrome has been associated with chlamydial urogenital infection.8 Chlamydial myocarditis has been described,9 as has endocarditis.10 The majority of investigation now concerns urogenital chlamydial syndromes.
Initially it was noted that a “sterile” form of acute mucopurulent conjunctivitis, similar to trachoma in that inclusions were noted in the cellular secretions, occurred in newborns. Interestingly, some parents exhibited those same inclusions in cells shed from areas of urethritis or cervicitis.11 In recent years, a distinct pneumonia syndrome in children under 6 months of age has been associated with colonization by chlamydia in the nasopharynx and trachea.12 These discoveries led to investigation of adult genital carriage of the organism, presumably as a reservoir for neonatal inoculation.
It is now fairly well accepted that C. trachomatis is one of the most frequently isolated sexually transmitted pathogens. C. trachomatis was first implicated in male nongonococcal urethritis (NGU) in 1966.13 By 1975, this relationship was firmly established by finding chlamydia in 42% of men with NGU, as opposed to 19% of men with gonococcal urethritis.14 Now C. trachomatis is recognized as a major cause of the female urethral syndrome (sterile pyuria and dysuria).15, 16 C. trachomatis and Neisseria gonorrhoeae have been found to coexist in more than 50% of patients with gonorrhea. Therefore, treatment of the gonorrhea with drugs unsuitable for treatment of chlamydia may result in “postgonococcal” urethritis.17
C. trachomatis is one of the most common causes of acute salpingitis, especially in Europe.18, 19, 20 Chlamydial salpingitis differs clinically from gonococcal disease in that the course is more protracted and symptoms more vague, although severe inflammatory changes occur in the internal female genitalia.21 Associated perihepatitis, the Fitz-Hugh--Curtis syndrome, has been reported in cases of chlamydial salpingitis.21, 22 The organism has subsequently been found in the peritoneal cavity of women undergoing tubal surgery to correct postinflammatory tubal infertility.23
The pregnant patient has recently become the object of attention in chlamydia research. Carrier rates of 2% to 23% have been reported.24, 25 Recent studies suggest that poor pregnancy outcome, such as abortion, stillbirth, and prematurity, may be up to ten times more frequent in pregnancies complicated by maternal chlamydial infection.26 Pelvic infection after elective abortion has been associated with C. trachomatis colonization.27 Colonized women delivered by cesarean section may subsequently suffer severe pelvic infection,27 and colonized women delivered vaginally are at risk for development of late (up to 6 weeks) postpartum endometritis due to C. trachomatis.28
The three serotypes of C. trachomatis that are responsible for LGV are inherently more invasive than non-LGV strains. The initial lesion on the genitalia is usually overlooked, and the organism ascends to the regional lymph nodes, causing a suppurative regional adenopathy with constitutional symptoms 2 to 6 weeks after initial exposure. The inguinal nodes are most often affected, whereas the hypogastric and iliac nodes may be involved in anorectal disease; obturator and iliac nodes may be affected after upper vaginal or cervical infection. The nodes are usually painful and may suppurate and become confluent and matted if left untreated, ultimately forming multiple draining fistulas. Sequelae include perirectal abscess, fistula in ano, and rectovaginal, rectovesical, and ischiorectal fistulas. Rectal strictures, keloid formation, and lymphedema are late complications.
The initial vesiculoulcerative lesion in LGV, if seen, is difficult to differentiate clinically from other ulcerative genital lesions. Early inguinal adenopathy must be differentiated from pyogenic adenopathy (secondary to distal infection due to staphylococci or streptococci), granuloma inguinale, secondary lues, chancroid, lymphoma, and miscellaneous infectious diseases such as bubonic plague, brucellosis, and cat-scratch disease.29
Diagnosis
The cornerstone of diagnosis of chlamydial infection is cell culture. Specimens collected by swab from the urethra and cervix should be immediately immersed in sucrose-phosphate transport medium and inoculated as soon as possible into McCoy cell monolayers.30 Refrigeration (not freezing) is preferable if inoculation is to be delayed. It should be emphasized that swabs of infected areas are necessary for reliable recovery of this organism; since C. trachomatis is a cell-associated pathogen, fluid cultures (e.g., culdocentesis fluid) are much less reliable than swab cultures (e.g., swab of fallopian tube), which are more apt to yield appropriately infected epithelial cells.
Even optimal laboratory facilities may take up to a week or more to report results, since this is a tissue culture procedure. In addition, tissue culture laboratories are not always available. Therefore syndromes associated with chlamydia may frequently be diagnosed either clinically or by less effective methods.
In patients with disease associated with chlamydia (e.g., salpingitis), failure to respond to therapy not directed against chlamydia (e.g., penicillin) should alert the physician to the possibility of chlamydia as the causative agent. Negative bacterial cultures (e.g., in urethritis) may also be a warning.
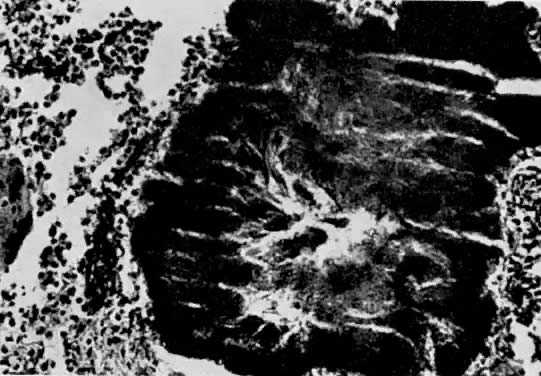
Chlamydial cervicitis has a distinctive presentation (Fig. 2). A follicular, exophytic cervicitis with mucopurulent endocervical discharge is classic.31, 32 This colposcopic appearance and a Papanicolaou smear showing inflammatory atypia or even dysplastic changes should suggest the possibility of chlamydial infection.
|

Serologic diagnosis of chlamydial infection by the acute-and-convalescent titers method is possible by microimmunofluorescent technique, although interpretation must be made with caution. The benefits of this method are that individual serotypes may be identified. Conversely, if the appropriate type-specific antibody is not included in the particular testing serum, seroconversion may be missed or inaccurate because of incomplete cross reactivity with the infecting serotype.
In general, a high index of suspicion and a thorough knowledge of the types of disease entities caused by C. trachomatis are the best weapons the clinician has against this organism.
Therapy
One of the early characteristics that led researchers to believe that C. trachomatis was not a virus was its sensitivity to antibiotics. In vitro studies have demonstrated C. trachomatis to be sensitive to the tetracyclines, erythromycin, sulfonamides, and rifampin.29, 33 Of interest to the obstetrician-gynecologist, however, are the reports that the popular new penicillin and cephalosporin drugs are inactive against this organism.34
The Centers for Disease Control in Atlanta, recommends treatment of proven chlamydial disease with tetracycline, 500 mg orally, four times/day, for at least 7 days. Alternatively, doxycycline, 100 mg twice a day, may be used. In patients with contraindications to tetracycline therapy, including pregnant women, erythromycin, 500 mg four times/day, is effective. If untoward gastrointestinal side-effects occur with this dose of erythromycin, the dosage may be halved (i.e., 250 mg four times/day), but the therapy must be extended to 14 days.35 Alternative therapy proven effective for urethritis includes a 10-day course of sulfonamides36 or 10 days of trimethoprim-sulfamethoxazole.37
Chlamydial conjunctivitis in the newborn may be prevented by erythromycin ointment ocular prophylaxis instead of the usual 1% silver nitrate solution; this regimen is accepted by the American Academy of Pediatrics38 and the National Society to Prevent Blindness.39 Topical therapy may not prevent nasopharyngeal infection or subsequent pneumonia.40 Established chlamydial newborn conjunctivitis or infant pneumonia should be treated with oral erythromycin syrup, 50 mg/kg/day in four divided doses, for at least 3 weeks.35
LGV is treated much the same as other C. trachomatis infections except for duration of therapy. Tetracycline, doxycycline, or erythromycin may be used but must be continued for 2 to 3 weeks. In addition, sulfamethoxazole, 1 g twice a day for 2 to 3 weeks, may be used. It is important that any buboes be aspirated through adjacent normal skin to prevent rupture; incision and drainage should be avoided, since it will delay healing. Any late sequelae, such as rectal stricture, must be dealt with appropriately after the acute infection is controlled.29, 35