The Bony Pelvis
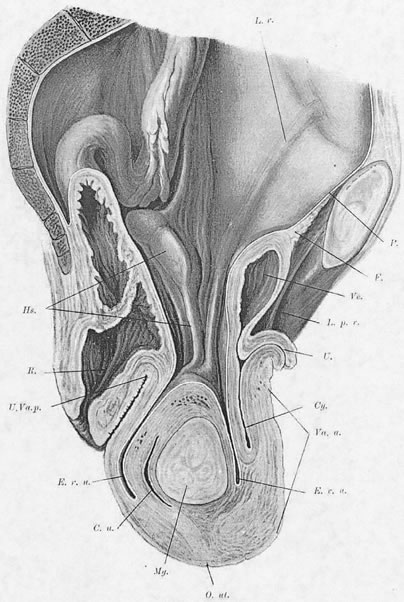
In the erect posture, which exaggerates the symptoms of pelvic relaxation, the plane of the pelvic inlet is slanted approximately 50° degrees from the horizontal. The axis of the superior pelvic strait, projected cephalad, meets the anterior abdominal wall at the level of the umbilicus. The inferior strait also is inclined anteriorly (Fig. 1). As a result, the uterus in normal anteversion is directed toward the sacrum and coccyx by any increase in intra-abdominal pressure. During pregnancy the uterus enlarges beyond the confines of the pelvis, and its weight is supported largely by the pubic rami and the anterior abdominal wall. In neither instance is the weight of the uterus directed toward the pelvic outlet.
|
The Pelvic Diaphragm
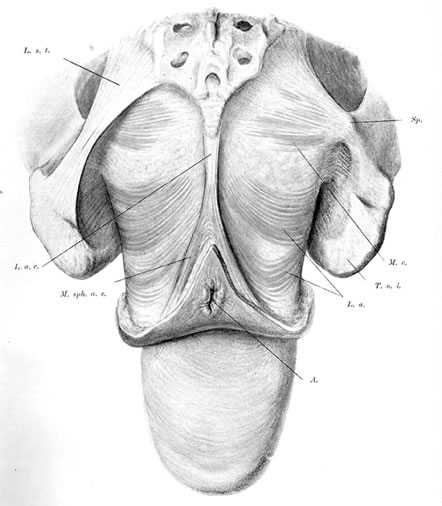
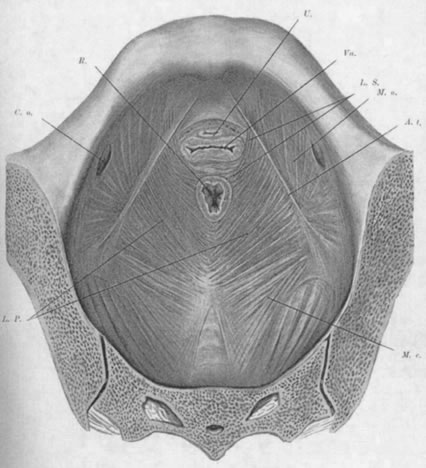
The pelvic diaphragm, or levator ani muscles, consists of the ischiococcygeal, iliococcygeal, and puborectalis muscles. The latter play an important role in the physiology of the pelvic floor and usually are better developed in the female, being stretched across a wider pelvic outlet. The puborectalis muscles bilaterally arise mainly from the lower surfaces of the pubic bones and from various levels of the obturator fascia; the muscle fibers run posteriorly and caudad, surround the rectum, and unite with fibers from the opposite side, forming a sling around the posterior surface of the rectum. That portion of the muscle posterior to the rectum is called the levator plate; it is distinct from the two lateral levator crura and constitutes the main portion of the levator diaphragm. The free medial edges of the puborectalis muscles are deflected inferiorly and join the rectum and urogenital tract for a short distance in their downward course.
The genital hiatus is the oval opening between the levator crura, through which pass the vagina and urethra. The configuration of the genital hiatus depends on the degree of contraction of the levator ani muscles.
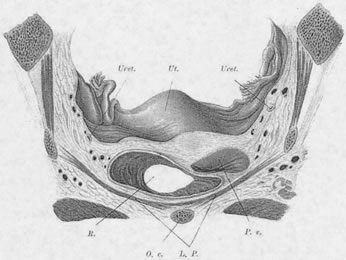
Viewed from above, the pelvic musculature resembles a concave plate. In sagittal section, the nadir of this plate is situated at a point posterior to the genital hiatus and overlying the coccyx. The genital hiatus thus lies not in the deepest portion of the pelvic floor but rather in the anterior, ascending segment (Fig. 2).
|
Normally, In the erect posture, a projection of the axis of the cervix meets the pelvic floor in the deepest portion of the levator plate, immediately anterior to the coccyx. The greatest part of an anteverted uterus lies posterior to the genital hiatus, resting on the levator plate. Anatomically, the lowest portion of the uterus is situated approximately at the interspinal line; the posterior rim of the genital hiatus lies 6 to 7 cm more anteriorly (Fig. 3).
|
The Perineal Membrane (Urogenital Diaphragm)
The perineal membrane, a fibromuscular triangular plate lying between the pubic rami, extends posteriorly to the anterior rectal wall. It lies inferior to the levator ani muscles and closes the genital hiatus. With the exception of the deep transverse perineal muscles, the urogenital diaphragm contains few muscle fibers. The diaphragm is most susceptible to injury at the point at which it is traversed by the vaginal canal. Because it is composed mostly of fibrous connective tissue, it cannot accommodate well to the distention and dilation that occur during delivery. The levator muscles that surround the genital hiatus are exposed to the same stress but, if intact, can resume normal position and dimensions within a short time. As a result of childbirth, a transient widening of the genital hiatus occurs, while damage to the perineal membrane is more permanent. DeLancey10 best describes the interactions between muscles and connective tissues in the posterior compartment.
Endopelvic Connective Tissue
The space between the pelvic peritoneum and the upper fascial sheaths of the levator ani muscles contains a fibroareolar connective tissue in which are embedded the blood vessels, lymphatic channels, and nerve fibers of the pelvis. In several places this tissue is condensed into thick, fibrous bands identified as pubocervical, cardinal, or sacrouterine ligaments. Strictly speaking, these structures are neither “fascia” nor “ligaments.” The material of which they are composed is not dense but loosely arranged and areolar.11 A preferable term would be endopelvic connective tissue (ECT).
Berglas and Rubin12 demonstrated the absence of ligamentous material in the ECT of two nulliparous cadavers. The region corresponding to the cardinal ligaments contained a plexus of veins embedded in loose areolar connective tissue. It was noted that if these veins were not injected postmortem with latex, they would collapse, causing the muscular walls and fibrous coats of the vessels, on histologic section, to resemble ligamentous structures.
Connective tissue contains fibroblasts that, under inflammatory or mechanical stress, are capable of proliferating into collagenous fibrous tissue. Gestation may accelerate this process in the ECT. If the pelvic floor loses its capacity to support the pelvic viscera, the areolar connective tissue responds by forming fibrous bands along the lines of greatest mechanical stress. By the time of surgery for uterine prolapse, the ECT usually has undergone marked hypertrophy and elongation. Clinically, the degree of connective tissue proliferation is directly proportional to the duration and extent of the prolapse. Normally, the ECT functions only to sheathe vessels and nerves, fill empty spaces, and provide a cover for the pelvic organs; it does not provide appreciable support but acts principally to limit mobility of the uterus within wide physiologic bounds. Connective tissue does not have the functional capacity to resist prolonged and repeated stress (i.e., increases in intra-abdominal pressure) and is invariably permanently deformed thereby.
Anatomic observations at the time of surgical repair, or on cadavers, are subject to misinterpretations. Collapsed veins may give a band of tissues a more “ligamentous” histologic appearance. Breaks in tissue integrity may result from dissections intended to expose the tissues for repair.
Debate continues concerning the composition and function of the ECT: shall we call it fascia or connective tissue? Further, the individual variability in the composition of the ECT often is not appreciated. For example, in a nulliparous woman the ECT may be relatively thin and appear sparse, although functioning well with large components of elastic tissue. In older, parous women with degrees of pelvic organ prolapse, the connective tissues are usually thickened by formation of collagen and reduction of elastic tissue . The density of the ECT represents the body's attempt to compensate for a lack of support. The changes in the ECT are comparable to the changes found in the transversalis fascia adjacent to peritoneal protrusions, as in inguinal or umbilical hernias. The layer of ECT is continuous with the transversalis fascia along the rising anterior abdominal wall.
Berglas and Rubin12 have stated explicitly, based on their histologic studies of these tissues, that there is no recognizable point of attachment of the ECT to the pelvic sidewall. Richardson and associates,13 in cadaver dissections, not only found direct attachment of these tissues to the arcus tendineus but also described recognizable separations of the fascial layers, or tears, which led them to recommend their repair at the time of surgery, with favorable results.
The question of the attachment of the ECT to the sidewall of the pelvis remains unresolved. Does a discrete attachment exist at the arcus tendineus, or is the ECT merely adherent laterally up the pelvic sidewall, over a wide area, along the course of the pelvic blood supply? While the firmness of attachment of one tissue to another cannot be stronger than the weaker of the two tissues, tissues broadly adherent may behave as if they are attached.