The function of the human placenta is of interest from both a scientific
and a clinical point of view. Unfortunately, in vivo study of the human placenta is very difficult because the methodology
carries with it unacceptable risks to both mother and fetus. Therefore, most
of our knowledge about the function of the placenta has been derived
from animal models. The placentas of higher primates are morphologically
most comparable to that of humans. Suitable primates, however, are
small, with even smaller fetuses. They have little tolerance for
indwelling catheters and often abort or deliver prematurely after intrauterine
surgery. In addition, these animals are prohibitively expensive
and thus have not been used extensively. Placental exchange has most
thoroughly been studied in the rabbit, guinea pig, and rat. The ultrastructure
of their placental barriers is comparable to that of the human (i.e. hemochorial placenta). The most widely used of all laboratory animals
in this regard, however, is the sheep. Pregnant ewes are of comparable
size to humans, with equally large fetuses that tolerate intrauterine
surgery well. The exchange barrier (i.e. epitheliochorial placenta) is quite unlike that of the human, however. There
is no good evidence that the placenta hemodynamics of the sheep
are comparable to those in humans; however, there is also little evidence
to the contrary. Placentas have three functions: the exchange of nutrient and waste materials
between mother and fetus, the manufacture and secretion of hormones, and
the maintenance of an immunologic barrier. Only the exchange
function and the hormone function of the placental barrier are discussed
in detail in this chapter. Because the exchange function is so dependent
on the rates of maternal and fetal placental blood flows, we must
first discuss placental hemodynamics. Hemodynamics The placenta is the only organ in the body with two separate blood supplies, each
coming from a separate organism. We have already discussed
the morphologic organization and ultrastructure of these two circulations. Because
the placenta is a transient organ and the blood flows change
rapidly with each stage of pregnancy, we know less about the regulation
of these blood flows than we do about the regulation of the blood
flow to any other organ in the body. The uteroplacental circulation is a low-resistance system for the maternal
organism. Resistance to blood flow is defined as the ratio of the
driving pressure and flow, where the driving pressure is the difference
between the central arterial pressure and the venous outflow pressure. There
is some question regarding the validity of using central arterial
pressure in the calculation of the driving pressure, however, because
direct measurement of mean pressures in the preplacental arteries
of animals with hemochorial placentas have been found to be approximately 8% to 20% of
the mean central arterial pressures. These findings
indicate that the physiologic regulation of maternal placental blood flow
may be complex and may depend on an arterial resistance to flow at
a site outside the organ itself. As a low-resistance system, the uteroplacental circulation is responsible
for, or at least contributes to, marked changes in maternal cardiovascular
physiology. Uterine arterial blood flow in the nonpregnant state
averages 1% to 2% of the maternal cardiac output. During pregnancy, uterine
blood flow rises markedly until at term it accounts for as much
as 17% of the maternal cardiac output (Table 1; Fig. 9). Some representative measurements of uteroplacental blood flow are listed
in Table 2. Maternal cardiac output per se increases 35% to 40% during pregnancy.15 Heart rate also increases but does so disproportionately with cardiac
output, resulting in a significant increase in stroke volume. There is
a slight fall in mean arterial pressure resulting from a significant
decrease in systemic vascular resistance; this reflects not only the development
of the low-resistance uteroplacental vascular bed but also
generalized systemic vasodilation. This explains the necessity of the 30% to 40% expansion
in blood volume associated with normal pregnancy
to maintain blood flow to other organs. Other maternal physiologic adaptations
to pregnancy are described elsewhere in this text. TABLE 1. Hemodynamic Values in Pregnant, Nonpregnant, and Puerperal Animals
| Pregnant | | Nonpregnant | | Puerperal | |
| No. | Mean | No. | Mean | No. | Mean |
Parameters | Animals | ± 1 SE* | Animals | ± 1 SE* | Animals | ± 1 SE* |
Arterial pressure | 34 | 97 ± 3 | 5 | 99 ± 2 | 5 | 107 ± 2 |
Cardiac Output | 13 | 101 ± 6.8 | 4 | 65 ± 2 | 4 | 82 ± 7 |
Total uterine blood flow | 13 | 17 ± 1.9 | 4 | 1.8 ± 0.9 | 4 | 2.7 ± 1 |
(ml/kg/min†) | | | | | | |
Uterine fraction of cardiac | 13 | 17 ± 2 | 4 | 1.4 ± 0.3 | 4 | 1.2 ± 0.3 |
output | | | | | | |
Total systemic vascular resistance | | 0.96 | | 1.5 | | 1.3 |
Uterine vascular resistance | | 5.7 | | 55 | | 40 |
* Figures represent mean ± 1 SE of several readings taken in the
control period after surgery has been completed.
† Expressed as per kilogram of ewe's weight.
(Dilts PV jr, Brinkman CR III, Kirschbaum TH et al: Uterine and systemic
hemodynamic interrelationships and their response to hypoxia. Am J Obstet
Gynecol 103:138, 1969)TABLE 2. Maternal and Fetal Placental Blood Flows During the Last Third
of Pregnancy
Species | Flow (mean ± SD) | Reference |
Maternal Placental Blood Flow |
Sheep | 180 ± 86* | Rankin and Phernetton1 |
| 228 ± 68* | Towell and Liggins2 |
| 270 ± 102* | Buss et al3 |
Rabbit | 75 ± 24* | Leduc4 |
Guinea pig | 85* | Symonds et al5 |
Rhesus monkey | 108† | Novy et al6 |
Humans | 149 ± 57* | Metcalfe et al7 |
Fetal Placental Blood Flow |
Sheep | 144 ± 45* | Rankin and Phernetton8 |
| 186 ± 46* | Thornburg et al9 |
| 278 ± 59* | Clapp et al10 |
Rhesus monkey | 208 ± 20* | Behrman et al11 |
Baboon | 104 ± 32* | Paton et al12 |
Humans | 115 ± 11* | Assali et al13 |
| 115 ± 36* | Eik-Nes et al14 |
* Values are ml/min/kg fetus
† Values are ml/min/kg uterus
 Fig. 9. Graph showing average uterine blood flow and uterine fraction of cardiac
output in pregnant, nonpregnant, and puerperal animals. Both rise markedly
during pregnancy.(Dilts PV Jr, Brinkman CR III, Kirschbaum TH et al. Uterine and systemic
hemodynamic interrelationships and their response to hypoxia. Am J Obstet
Gynecol 103:138, 1969) Fig. 9. Graph showing average uterine blood flow and uterine fraction of cardiac
output in pregnant, nonpregnant, and puerperal animals. Both rise markedly
during pregnancy.(Dilts PV Jr, Brinkman CR III, Kirschbaum TH et al. Uterine and systemic
hemodynamic interrelationships and their response to hypoxia. Am J Obstet
Gynecol 103:138, 1969)
|
The fetal placental circulation receives approximately two thirds of the
total fetal cardiac output. Some representative measurements of umbilical
blood flow are listed in Table 2. This high flow rate is important in the transport of oxygen and nutrients
from mother to fetus and is maintained by a number of anatomic differences
in the fetal circulation. Because the fetal lungs do not have
any respiratory function, a high vascular resistance is maintained in
this organ by the mechanical effects of the unexpanded alveoli on the
vessel walls and the vasoconstrictive effect of the low oxygen tension
that prevails in the fetal blood. These two factors combine to shunt
approximately two thirds of the right ventricular output away from the
lungs toward the systemic circulation through the ductus arteriosus, which
is maintained patent by the same low oxygen tension that keeps
the pulmonary vessels constricted. With the large right-to-left shunt, a
high cardiac output (almost twice that of the mother) is created, providing
for a high flow rate across the placental exchange membranes. The controversy over the existence of shunts in the maternal and fetal
placental circulations stems, at least in part, from the inconstant use
of the word shunt.16 If a maternal shunt is defined as that fraction of the uterine blood flow that does not supply
an area where exchange between maternal blood and fetal blood takes
place, about 84% of the uterine blood flow during the last third of
gestation is placental blood flow in most animals. However, the actual
maternal shunt may be greater than the nonplacental blood flow if there
are additional shunts in the placental or preplacental vessels. A fetal shunt may be defined as the fraction of the umbilical blood flow that does not
supply an area where exchange between fetal blood and maternal blood
takes place. In sheep, it has been demonstrated that during the last
third of gestation about 6% of the umbilical flow was not placental flow
but that which perfused the intercotyledonary chorion. We cannot assume, however, that
this value applies to other species, including primates, because
of morphologic differences. As is true with the uterine
circulation, the actual shunt in the umbilical circulation may be even
greater if there are also shunts within the placenta. Regulation of Placental Blood Flows One must consider first whether the pressure in the surrounding tissue
and the adjacent circulation plays a role in the regulation of either
the maternal or the fetal placental blood flow. During labor, uterine
contractions grossly impair maternal placental blood flow, presumably
by distortion or occlusion of the preplacental vessels.2 Whether or not mechanical factors play a role in flow regulation before
labor, however, is open to question. If anywhere along a vessel there is an external “surrounding pressure” that
is greater than the intravascular pressure, the vessel
will collapse at that site. Driving pressure under these conditions
is the difference between arterial pressure and the surrounding pressure. Flow
under these circumstances is called sluice flow.16 With this type of flow, increased uterine vein pressure could result in
impedance of the umbilical circulation. Sluice flow has been observed
in the umbilical circulation only in artificially perfused placental
preparations. Intact, unanesthetized fetal lambs have yielded no evidence
that umbilical vascular resistance was affected by changes in uterine
venous pressure. In species with hemochorial villous placentas in
which the maternal blood flows in the intervillous space surrounding
the fetal villi, sluice flow appears to be anatomically possible, but
as yet there is no physiologic evidence for it. An important question is whether the uteroplacental circulation is able
to autoregulate. Autoregulation is generally defined as the ability of an organ to adjust its vascular
resistance by local control mechanisms in the face of changing perfusion
pressure.17 Thus, the effects of changes in perfusion pressure are minimized, and
blood flow remains constant. From the standpoint of the fetus, autoregulation
in the uteroplacental circulation would seem to be essential. Studies
in pregnant sheep, however, indicate that uterine blood flow varies
directly proportionally with mean arterial pressure and have failed
to demonstrate a system of autoregulation. The presence of autoregulation
mechanisms has been suggested by the maintenance of a constant
flow rate over a wide range of pressures in pregnant rabbits and pregnant
rhesus monkeys, but the evidence is not conclusive. Maternal regulation of uterine and placental blood flows does not appear
to be strong.18 The degree of autonomic innervation to the uterine vasculature during
pregnancy varies widely from species to species. Both adrenergic and cholinergic
sympathetic fibers are found in the uteri of most animals. Sacral
nervous influences may be involved in the maintenance of a high
uterine blood flow rate in those species that possess cholinergic innervation (e.g. uterine nerve stimulation in the pregnant guinea pig causes uterine vasodilation). Adrenergic
fibers are present in the uterus of all animals
studied, but histologic examination reveals that pregnancy causes the
complete disappearance of these fibers in the myometrium and a great
reduction in their numbers around the uterine blood vessels. Nevertheless, electrical
stimulation of the sympathetic chain in term pregnant
sheep and dogs results in increased uterine vascular resistance and decreased
uterine blood flow. There are a number of chemical factors that are vasoactive in the uteroplacental
circulation. The results of older studies in anesthetized pregnant
sheep seemed to indicate that hypoxia could increase as well as
decrease uterine blood flow, but experiments with conscious animals have
failed to show any appreciable effect of maternal hypoxia or hyperoxia
on uteroplacental blood flow. The uterine vasculature is also relatively
insensitive to hypercapnia and hypocapnia, although hypocapnia
has been reported to cause a reduction in placental, but not myometrial, blood
flow in rabbits. The results of these studies may have been
influenced by secondary factors such as catecholamine release, however. Thus, the
available evidence strongly suggests that changes in maternal
arterial blood gases are not of physiologic importance for short-term
regulation of uteroplacental blood flow. Intravenous infusion of exogenous epinephrine and norepinephrine causes
a strong dose-dependent decrease in uterine blood flow in both nonpregnant
and pregnant sheep; in the latter, the response was observed in
both the myometrial and the maternal placental blood flows. This seems
to demonstrate the existence of an adrenergic vasoconstrictor mechanism
in the uterine and maternal placental circulations. The vasoconstriction
response of the maternal placental vascular bed to α-adrenergic
receptor stimulation is, by far, the most definite and unambiguous
response of the placenta to any maternal vasoactive agent. The response to β-adrenergic stimulation is not so clear-cut. Although
the vasculature of the nonpregnant uterus responds to β-adrenergic
agonists with vasodilation, there is no evidence for β-adrenergic
activity at all during pregnancy, and specific β-adrenergic
receptor blockade does not alter uterine blood flow. The real role of angiotensin II in the maintenance of the uteroplacental
circulation is also unclear. Angiotensin II is a powerful vasoconstrictor, yet
in various animals the response to angiotensin II infusion
varies from an increase in vascular resistance to a decrease in vascular
resistance in the maternal placental circulation. These conflicting
reports probably reflect differences in dosage and the physiologic state
of the animal preparation. The estrogens, particularly 17β-estradiol, have been found to cause
vasodilation of the nonpregnant uterine vasculature, with blood flows
increasing as much as tenfold. This response is delayed, however, and
the peak response is not attained until about 1.5 hours after the stimulus. Similar
but smaller responses have been observed during pregnancy, suggesting
that the maintenance of a high rate of maternal placental
blood flow may be, in part, due to the endocrine function (estrogen
production) of the placenta. The actions of the prostaglandins in the maternal placental circulation
are also unclear.17 Metabolites of arachidonic acid (eicosanoids), produced by both the cyclooxygenase
and lipoxygenase pathways, are synthesized during pregnancy
and are implicated in the regulation of systemic and local blood flows
in both maternal and fetal vascular systems.18 The actions of these substances on the placental circulation vary not
only by their concentrations, interactions with other vasoactive agents, and
animal species studied but also by the ability of some prostaglandins
to induce uterine contractions, thus occluding the input and output
vessels. Cyclooxygenase converts arachidonic acid to prostaglandin
G2 (PGG2), which is rapidly converted to prostaglandin H2 (PGH2). These short-lived intermediates possess intrinsic biologic activity
which can be inhibited by nonsteroidal anti-inflammatory agents (NSAIDs).19 PGH2 is subsequently converted into thromboxane and prostaglandins F2α, D2, and E2. Thromboxane serves as a potent vasoconstrictor, stimulator of platelet
aggregation, and stimulator of uterine contractility.20 PGF2α has vasoconstrictive properties, whereas PGD2 has vasodilating effects. PGE2 is also a vasodilator, but it causes uterine contractions and decreased
placental blood flow when administered to pregnant sheep. When administered
to the fetus, however, thus bypassing the myometrium, PGE2 causes vasodilation of the maternal placental circulation. Prostacyclin (PGI2), also derived from PGH2, is a vasodilator produced by the pregnant uterus that does not cause
uterine contractions in the near-term sheep. PGI2 infusion results in a slight maternal placental vasoconstriction, but
this response may be secondary to the maternal hypotension and release
of circulating catecholamines. Blockage of prostaglandin synthesis with
indomethacin in near-term pregnant sheep and rabbits causes vasoconstriction
of the placental circulation but not of the myometrium. These
experiments suggest that the placenta synthesizes dilating prostaglandins, probably
PGE2 or PGI2. In addition to their direct role as vasoactive agents, prostaglandins also
can modulate the response to other vasoactive agents. PGE2 infusion depresses the placental vasoconstriction response to norepinephrine; prostaglandin
inhibition with indomethacin causes a potentiation
of the vasoconstriction response of the placental vascular bed to epinephrine. This
indicates that PGE2 suppresses the response of the placental vascular bed to circulating catecholamines
and that there is an endogenous supply of PGE2 that, when eliminated, increases the sensitivity of the placental vascular
bed to catecholamines. It has also been suggested that the estrogen-mediated
increase in uterine blood flow is secondary to prostaglandin
formation, based on the fact that indomethacin pretreatment depresses
this response. There is no more conclusive evidence to support this
hypothesis, however. The lipoxygenase enzymes catalyze the formation
of hydroperoxyeicosatetraenoic acids (HPETEs) from arachidonic acid. HPETEs
are then converted to either hydroxyeicosatetraenoic acids (HETEs) or
leukotrienes (LT). The physiologic functions of placental lipoxygenase
metabolites during pregnancy or in the placenta are not known, but
the HETEs, as well as the HPETEs and LTs, do exert biologic actions (i.e. leukocytic chemotaxis and enhancement of vascular permeability in nonplacental
tissues) that may be important to placental function and pregnancy.19 The maternal placental blood flow does not appear to be under strong maternal
control.21 The mother seems to be able to shut down the placental circulation by α-adrenergic
receptor stimulation, but there is little response to
other circulating vasoactive agents. Teleologically, the mother's
only control is in the ability to sacrifice the fetus under certain
circumstances. Regulation of the fetal placental circulation is also poorly understood.17 The evidence for autonomic innervation of the umbilical circulation is
conflicting. Whereas histochemical methods have been unable to demonstrate
either adrenergic or cholinergic fibers in the human placenta and
umbilical cord, methylene-blue-staining fibers have been found in the
umbilical arteries and the placenta of lower primates. Both adrenergic
and cholinergic fibers are evident in the intrafetal umbilical vessels
in the guinea pig. As with the maternal placental circulation, most
of our understanding about the chemical control of the umbilical circulation
comes from studies in pregnant sheep. Blockade of α-adrenergic
or angiotensin receptors has no effect on the resistance of the
umbilical vascular bed, and this is taken to imply that the maintenance
of normal tone in this vascular bed is not under the control of angiotensin
or circulating catecholamines. Exogenously administered angiotensin
and catecholamines both produce umbilical vasoconstriction, but
their role in the normal physiologic state is still questionable. Estrogens
have been shown to dilate the umbilical artery, and in most species, estrogen
levels tend to increase near parturition, but it is not
clear whether they play a role in regulation of the umbilical circulation. The
influence of prostaglandins on the umbilical circulation is quite
different from that on the maternal placental circulation. The umbilical
vascular bed is unresponsive to exogenous PGI2, but PGE2 produces a greater degree of vasoconstriction than the maximal response
to angiotensin, norepinephrine, or any other chemical substance. However, indomethacin
causes vasoconstriction in the fetal placental circulation, which
argues against the existence of an endogenous prostaglandin
vasoconstriction mechanism. There is no compelling evidence that
any of these agents are involved in the regulation of the umbilical blood
flow. Before leaving the discussion of uteroplacental blood flow regulation, one
other possibility must be considered. If maternal placental blood
flow is not controlled by the mother, could it be under fetal control?17 Recently, it has been demonstrated that the perfusion-perfusion ratios
in the sheep placenta are extremely evenly distributed at the macroscopic
level. Such a similarity in blood flows and their distributions argues
for the presence of a regulating mechanism. In such a system, a
reduction of maternal flow would be accompanied by the synthesis of a
fetal vasoconstrictor and maternal vasodilator, thereby maintaining the
perfusion-perfusion ratio. PGE2 has been shown to cause vasodilation in the maternal placental vascular
bed when given by way of the fetal circulation, and it also has a vasoconstricting
effect on the umbilical circulation. Some evidence also
suggests that fetal vessels synthesize PGE2. The existence of such a chemical link between mother and fetus is suggested
by experiments in both sheep and rabbits in which occlusion of
the umbilical blood flow causes a fall in uterine blood flow. The evidence
for fetal control of the maternal placental circulation is by no
means conclusive, but the lack of evidence for strong maternal control
makes it an attractive possibility. Placental Transfer Throughout pregnancy, the placenta retains the primary role of all biologic
membranes (i.e. selective permeability).16,22,23 With particulate matter such as blood cells and macromolecules, transfer
is severely restricted, providing a “placental barrier.” At
the other end of the spectrum, the transfer of many essential nutrients
is accelerated by a variety of transport mechanisms. The ideal blood flow in a transport system such as that represented by
the placenta is a countercurrent flow, in which the two bloodstreams flow in directions exactly opposite to
each other (Fig. 10). With this flow, the widest possible gradient for exchange between the
two bloodstreams exists over the entire length of the exchange membrane. This
is important in the exchange of materials that cross the placenta
by simple diffusion, because the only driving force is the concentration
gradient. Concurrent flow, in which the two bloodstreams flow in the same direction (i.e. parallel to each other), is the least efficient for transfer. In the human
placenta, a compromise probably exists in that maternal blood flows
randomly in all directions with respect to the fetal circulation. This
is known as crosscurrent flow, or pool flow. The villi are bathed continually by a fountain of maternal
blood with completely variable combinations of flow directions (see Fig. 6). Some transport efficiency is obviously lost by this distribution.  Fig. 10. Diagram of countercurrent and concurrent flow between maternal and fetal
circulations. The two flows are randomly distributed in the human.(Shapiro NZ, Kirschbaum T, Assali NS. Mental exercises in placental transfer. Am
J Obstet Gynecol 97:130, 1967) Fig. 10. Diagram of countercurrent and concurrent flow between maternal and fetal
circulations. The two flows are randomly distributed in the human.(Shapiro NZ, Kirschbaum T, Assali NS. Mental exercises in placental transfer. Am
J Obstet Gynecol 97:130, 1967)
|
As an organ of gas exchange, the placenta is less efficient than the lung. It
is generally believed that the gases O2 and CO2 cross the placenta by simple diffusion, the driving force being the concentration
difference on each side of the membrane. As nonpolar, lipid-soluble
molecules, both O2 and CO2 are capable of diffusing rapidly through the lipid portion of cell membranes. Early
attempts to determine the mean O2 gradient across the placental barrier used arterial and venous PO2 measurements (Table 3). These studies indicated that the O2 diffusion capacity was rather low, suggesting that O2 delivery to the fetus was partially limited by diffusion resistance of
the membrane. It is now known that these estimates are in error because
O2 tensions in the uterine and umbilical veins are not necessarily representative
of those in the end-capillary placental bloods, and the placenta (and
the uterus) itself consumes a significant fraction of the O2 removed from the maternal blood. Using the diffusion characteristics of
CO, the diffusion capacity for O2 has been estimated to be four times greater than that estimated from partial
pressure gradients in the uterine and umbilical veins. Thus, it
has been determined that O2 equilibrates completely in the maternal and fetal end-capillary bloods
during a single pass of these bloods through the placental exchange vessels. Transfer
of O2 is thus maximal, and such transfer is termed “flow-limited,” although
what is really meant is “not limited by the membrane
characteristics.” TABLE 3. Human Material and Fetal Blood Constituents
 There are several factors that influence O2 transfer across the placenta. The fetus compensates for low O2 levels with a higher blood concentration of hemoglobin (see Table 3), which has a greater affinity for O2. The fetal hemoglobin O2 dissociation curve is shifted to the left of that for maternal blood, which
means that for any given O2 tension, fetal blood contains a greater amount of O2 than maternal blood. Furthermore, the release of fetal metabolites into
the maternal blood results in a fall in the pH of maternal blood, which
shifts the maternal O2 dissociation curve even further right, automatically increasing the mass
transfer of O2 to the fetus (i.e. Bohr effect). There is some evidence that O2 may be transferred across the placenta by facilitated diffusion with cytochrome
P-450 as the carrier; however, this has not been confirmed. It
could be argued that the O2-diffusing capacity of the placenta computed from the known CO-diffusing
capacity fully accounts for the observed transplacental fluxes of O2; thus, postulation of a carrier is unnecessary. Carbon dioxide transfer between mother and fetus has been studied less
extensively. The diffusion constant of CO2 is 20 times higher than that for O2; therefore, membrane resistance is clearly not a factor. Most reports
indicate that there is a narrow gradient across the placenta in favor
of the fetus. Although CO2 is present in the blood in the form of dissolved gas (CO2), carbonic acid (H2CO3), bicarbonate ion (HCO3-), carbonate ion (CO2-), and carbaminohemoglobin, experimental evidence indicates that placental
transfer of carbon dioxide is in the form of CO2 and that the transfer of the other forms is comparatively negligible. The fetus requires a continuous influx of fuels for combustion and of building
materials for growth. In addition, the fetus requires vitamins, trace
elements, and, perhaps, hormones as cofactors and regulators of
the metabolic processes. In animals and humans, the concentration of
glucose, the principal metabolic fuel, is higher in maternal than in
fetal plasma (Table 4). It is also known that fetal glucose is derived from maternal plasma. These
observations are compatible with a purely diffusional process for
glucose transport. However, studies in animals have demonstrated that
transport of D-glucose occurs much faster than that of molecules of
comparable molecular weight such as mannitol or L-glucose. Furthermore, the
transport of 3-0-methyl-D-glucopyranose (3MeG) is considerably
greater than predicted by its molecular weight; its transfer is also inhibited
by the presence of D-glucose. These observations strongly suggest
the presence of a shared carrier mechanism for 3MeG and D-glucose. This
process, known as facilitated diffusion, involves a membrane carrier
that, when combined with glucose, increases the solubility of glucose
in the lipid bilayer portion of the membrane, thus speeding its
diffusion across the barrier. There is no evidence that energy is required (i.e. active transport), however. TABLE 4. Composition of Amniotic Fluid and Maternal and Fetal blood
 Fructose is present in the plasma of both mother and fetus in small quantities (see Table 4). It is not used as a fetal fuel or as a building material in significant
amounts, except perhaps during periods of fetal hypoglycemia. The
placental barrier is almost totally impermeable to fructose, and this
sugar is apparently synthesized from D-glucose by the placenta. Lactate
is also produced by the placenta from D-glucose, and there is apparently
no transfer back to the mother. There is presumptive evidence for
placental transfer of acetate, but the mechanism is unexplored. Although free fatty acids do not cross the placenta of sheep easily, they
readily cross the hemochorial placentas of the rabbit, guinea pig, and
rhesus monkey and participate in the synthesis of fetal lipids. This
strongly suggests that they also cross the human placenta. The mechanism
by which these substances cross the placenta is unexplored. Triglycerides
are carried in the plasma in chylomicrons, which are too large
to travel in the interstitial spaces of the placenta. They do not cross
the placenta to any significant degree. Cholesterol is carried in
the plasma, mostly in the esterified form as lipoprotein, and it is extremely
unlikely that cholesterol can cross the placenta in this form. Maternal
cholesterol does reach the fetus; however, the mechanism involved
is unknown. Amino acids are delivered to the fetus mainly for protein synthesis, but
they also contribute to the requirements for fetal energy. The fetal
plasma concentration is higher than the maternal plasma concentration
for all amino acids except citrulline (Table 5). The placental tissue also concentrates a large number of amino acids
intracellularly from maternal plasma. The fetal uptake of amino acids
may depend to some extent on this concentrating capacity of the placenta. Uptake
of amino acids from the maternal plasma by the placenta occurs
by diffusion and active transport involving a carrier.24 The transport carriers are stereospecific, transporting the L-amino acids
more rapidly than the D-amino acids. Recent evidence also indicates
that placental amino acid transport is dependent on a process requiring
protein synthesis, suggesting that the carriers are integral membrane
proteins, which must be synthesized. Additionally, the active transport
of amino acids is mediated by several pathways that are specific
for several groups of amino acids. Three separate placental transport
systems have been described for the neutral amino acids (Table 6): the A, or alanine-preferring system; the L, or leucine-preferring system; and
the ASC, or alanine-serine system. Each system preferentially
transports certain neutral amino acids, but there is considerable overlap
among the systems. The overlap may be of considerable importance
in ensuring the fetus receives an adequate supply of amino acids in the
face of decreased maternal concentrations. In addition, regulation
of fetal amino acid uptake may be, in part, the result of changes in the
relative activity of these separation transport systems. It is also
likely that additional, unidentified transport pathways are present for
the acidic and basic amino acids as well. TABLE 5. Placental, Maternal and Fetal Free Amino Acids
| Placental* | Maternal† | Fetal† |
Taurine | 10,300 | 60 | 135 |
Glutamate | 5,626 | 103 | 135 |
Aspartate | 3,446 | 20 | 21 |
Alanine | 1,772 | 258 | 415 |
Glycine | 1,503 | 142 | 231 |
Glutamine | 934 | 325 | 445 |
Threonine | 617 | 158 | 258 |
Serine | 651 | 104 | 149 |
Lysine | 170 | 103 | 304 |
Valine | 166 | 101 | 206 |
Arginine | 242 | 43 | 91 |
Leucine | 212 | 59 | 117 |
Tyrosine | 173 | 29 | 59 |
Phenylalanine | 112 | 36 | 72 |
Asparagine | 38 | 157 | 209 |
Isoleucine | 56 | 34 | 68 |
Citrulline | 100 | 14 | 13 |
Histidine | tr† | 66 | 261 |
Methionine | tr | 25 | 32 |
Ornithine | | 48 | 95 |
* mmols/liter intracellular water
† mmols/liter plasma
† TR = trace
(Adapted from Lemons JA: Fetal-placental nitrogen metabolism. Semin Perinatol 3:177, 1979)TABLE 6. Placental Transport Systems for Amino Acids
A | L | ASC |
a-Aminoisobutyric acid | Leucine | Alanine |
Glycine | Isoleucine | Serine |
Proline | Valine | Threonine |
Alanine | Phenylalanine | Glutamine |
Seine | Alanine | |
Threonine | Serine | |
Glutamine | Threonine | |
| Glutamine | | (Adapted from Lemons JA: Fetal-placental nitrogen metabolism. Semin Perinatol 3:177, 1979)The fat-soluble vitamins are transported in the plasma bound to proteins, sometimes
in lipoprotein complexes. The mechanisms and ease of release
to the placenta are unknown, and transfer is believed to be by simple
diffusion. Levels of the fat-soluble vitamins in the fetal blood are
lower than those in maternal blood. The water-soluble vitamins are
found in the fetal blood at levels higher than those in maternal blood, indicating
that transfer may be by active transport. The mechanisms
are uninvestigated, however. Most cations and anions are transported with relative ease. The fetal concentrations
of total Ca2+ are higher than the maternal plasma concentrations, and there is a net
flux of Ca2+ across the placenta, as evidenced by fetal uptake. Calcium occurs in plasma
in the protein-bound form and the free ionized form. If we assume
that Ca2- crosses the placenta only in the free ionized form, either there is a
sufficiently large electrical potential difference across the exchange
membrane to account for the higher fetal than maternal concentrations
or there is active transport of Ca2+ across the placenta. The concentrations of phosphates are also much higher
in fetal than in maternal plasma. As with Ca2+ , there must be either a transplacental potential difference or active
transport to explain this difference. Iron is transferred preferentially
to the fetus by active transport and achieves a higher concentration
there than in the mother. In maternal plasma, iron is bound to a protein, transferrin, that
binds to receptors on the trophoblast. The iron
is then removed, leaving an empty molecule (apotransferrin) that returns
to the maternal circulation to acquire more iron. The unbound iron
then is actively transported to the fetal side, where it is taken up
by fetal transferrin. There does not seem to be a retrograde transfer
of iron from the fetus to the mother. Copper crosses the placenta with
relative ease; zinc apparently is transferred much more slowly. The
mechanisms of transfer are unknown. Despite their large molecular size, maternal plasma proteins also appear
in the plasma of the fetus. The mechanisms by which passive immunity
is conferred to the developing fetus are the most thoroughly studied
aspects of placental protein transfer. Differences in transfer rates among
proteins cannot be explained by molecular size, because γ-globulins, specifically γG and γA, are more than twice the
size of albumin but are transferred to the fetus at a rate faster than
that of albumin. Several hypotheses have been proposed to explain the
mode of selection and transport of immunoglobulins, but all involve a
combination of binding of immunoglobulins to specific receptors in the
placental membrane and pinocytosis, a process somewhat analogous to
phagocytosis by macrophages. Pinocytosis is an active cell process, like
active transport, it requires the input of energy. Although these processes
have been studied most extensively in the yolk sac placenta of
rabbits, guinea pigs, and rats, the same events apparently occur in
the chorioallantoic placenta. Immunoglobin receptors have been demonstrated
on human placental membranes, although they have not been chemically
characterized. Albumin, glycoprotein, and mucoprotein cross the placental
barrier quite slowly and in proportion to their molecular weights. Thyroxine
and triiodothyronine both cross in small amounts, although
enough may be present to depress the fetal thyroid. The placental
transfer of glucagon, growth hormone, insulin, follicle-stimulating hormone (FSH), luteinizing
hormone (LH), and prolactin is too slow to be
of physiologic significance. In addition to CO2, the fetal wastes (i.e. urea, bilirubin, and small amounts of creatinine), must be eliminated. Urea
apparently crosses to the maternal circulation by simple diffusion. Bilirubin
exists in two forms: the unconjugated form, which is carried
in the plasma bound to plasma albumin, and the conjugated form, which
is water soluble and carried in the plasma as such. The unconjugated
form dissociates from albumin easily and diffuses rapidly from fetus
to mother across the placenta. Conversely, the conjugated form is so
lipid insoluble that it is restricted to the interstitial spaces of
the placental barrier; therefore, it diffuses across only slowly. The
placental transfer of creatinine has not been investigated. Intact fetal red blood cells are found in the maternal bloodstream, apparently
transfused through small disruptions in villi into the intervillous
space. As much as 0.5 ml of fetal cells may be found in the maternal
bloodstream. Fetal and maternal platelets and leukocytes interchange
freely, but there is no documentation of maternal red cells in the
fetal bloodstream. Placental Hormones At one time the placenta was thought to function almost exclusively as
a transport organ; however, it is known now to possess many other functions, not
the least of which is the production of hormones.25,26 From the earliest days of pregnancy, trophoblastic cells produce a variety
of hormones; in fact, both gonadotropin and steroid synthesis have
been demonstrated in rabbit preimplantation blastocysts. PROTEIN HORMONES. The protein hormones made by the placenta are remarkably similar to their
pituitary counterparts. The two most important protein hormones produced
by the placenta are human chorionic gonadotropin (hCG), and human
placental lactogen (hPL). hCG is a glycoprotein in which the carbohydrate
portion represents approximately 30% of the molecule. Like other
glycoprotein hormones (i.e. FSH, LH, and thyroid-stimulating hormone [TSH]), hCG consists
of two noncovalently bonded subunits, α and β, with molecular
weights of 18,000 and 28,000, respectively. The α subunit is nearly
identical to the α subunits of other glycoproteins. The β subunit
is specific to hCG and has a 30-amino acid residue at the carboxyl
end that is not present in β subunits of the other glycoprotein
hormones. The preparation of antibodies to the α subunit is
the basis of the radioimmunoassay specific for hCG, which is useful in
the diagnosis of pregnancy. Several facts support placental origin of
this hormone. The highest concentration of hCG is found in the placenta, and
removal of all chorionic tissue eliminates hCG from maternal plasma. hCG
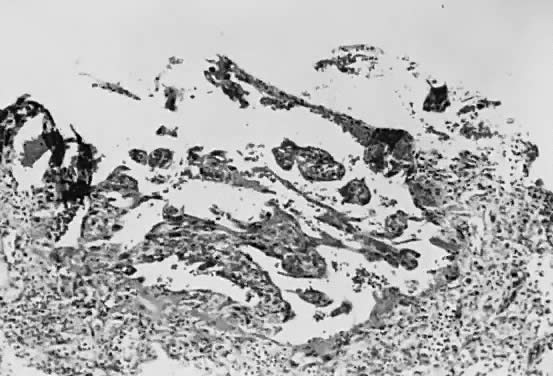
is produced in molar pregnancies in the absence of a fetus, i.e. incomplete mole. The site of hCG production is more difficult to evaluate. Classic studies
indicate that hCG is produced by the cytotrophoblast and that the decline
in levels at midpregnancy coincides with the disappearance of cytotrophoblast
cells, as shown on light microscopy. Electron microscopic
studies indicate that the cytotrophoblast does not disappear but is
attenuated or thinned during the last half of pregnancy. There is well-developed
endoplasmic reticulum in the syncytiotrophoblastic cells, indicating
an ability to synthesize proteins. Immunologic studies have
demonstrated the presence of hCG in the syncytiotrophoblast of both early
and full-term placentas, but this does not prove that it is produced
there. The regulation of hCG synthesis is the subject of intense investigation. It
has been observed that cyclic adenosine monophosphate
stimulates its production by trophoblastic cells in culture. hCG can be detected in serum as early as 10 days after conception. There
is a marked rise 10 to 14 days later, with a peak at 45 to 60 days after
conception (Fig. 11). Serum levels then drop abruptly to low levels, which persist to term. Urine
hCG levels closely parallel serum levels. Urinary excretion of
hCG is the basis for all of the current qualitative tests for pregnancy. Modern
immunoassay techniques make it possible to detect hCG as early
as 7 days after conception, when it is indistinguishable from LH. If
ovulation is late during the study cycle, this lack of specificity
can be confusing.  Fig. 11. Serum concentration of human chorionic gonadotropin (HCG) during pregnancy. Urinary
excretion is similar.(Danforth DN. Textbook of Obstetrics and Gynecology. New York, Har-per & Row, 1968) Fig. 11. Serum concentration of human chorionic gonadotropin (HCG) during pregnancy. Urinary
excretion is similar.(Danforth DN. Textbook of Obstetrics and Gynecology. New York, Har-per & Row, 1968)
|
The function of hCG is confusing. Corpus luteum function definitely is
prolonged by the action of hCG. However, many studies have shown that
bilateral oophorectomy may be performed in the first few weeks of pregnancy
with no ill effects. hCG concentrations reach a peak at a time when
the hormone no longer is needed. hCG stimulates placental estrogen
production, but there is no evidence that it is necessary for it. Small
amounts of hCG reach the fetus and may play a role in the early development
of steroid synthesis in the fetal adrenal and testes. It has been found that hCG inhibits the in vitro lymphocyte-stimulating effect of phytohemagglutinin. This has been interpreted
by some as indicating a partial suppression of immunity and as
affording a means by which the fetus, which is immunologically foreign
because of inherited paternal antigens, avoids rejection as a foreign
body. However, there is little other supportive evidence for these
speculations. hPL is a single polypeptide chain with a molecular weight of approximately 20,000. It
is similar to human growth hormone; about 80% of the amino
acid residues are identical in the two molecules. The term human placental lactogen, like the term human chorionic gonadotropin, applies to biologic activity rather than to the hormone itself. hPL is produced by the trophoblast. It disappears from maternal serum within
a few hours after delivery of the placenta. Immunofluorescence studies
localize hPL in the syncytiotrophoblast; polysomes and messenger
RNA isolated from the syncytiotrophoblast tissue and incubated in vitro have synthesized hPL. The regulation of hPL synthesis also remains an
enigma. In general, the amount of hPL formed is related to placental size, but
other factors, such as ionic environment and nutrient variables, may
also contribute. It is of interest that rapid intravenous infusion
of glucose decreases hPL, whereas intravenous arginine raises plasma
hPL levels. hPL secretion may be regulated to some extent by some
placental factor analogous to the hypothalamic factor controlling growth
hormone release by the pituitary. hPL has lactogenic activity in animals and puerperal humans and luteotrophic
action in the rat. There has been some evidence that it has growth
hormone-like activity; it may potentiate the ability of growth hormone
to cause growth of the tibial epiphyses in hypophysectomized rats. Evidence
of its growth hormone-like activity is limited, however, and
is subject to question. hPL has also been shown to suppress the in vitro phytohemagglutinin-induced lymphocyte response, but the significance of
this phenomenon is not clear. Small amounts of hPL do appear to reach
the fetus, although the role of this hormone, if any, in fetal development
is unknown. hPL has been used as an index of placental and therefore
fetal well-being, because concentrations in plasma rise as term
approaches (Fig. 12).  Fig. 12. Serum concentration of human placental lactogen (HPL) during pregnancy. The
shaded area shows normal range. Lines are from patients with chronic
placental insufficiency.(Saxena BN, Emerson K Jr, Selenkow HA. Serum placental lactogen [HPL] levels
as an index of placental function. N Engl J Med 281:255, 1969) Fig. 12. Serum concentration of human placental lactogen (HPL) during pregnancy. The
shaded area shows normal range. Lines are from patients with chronic
placental insufficiency.(Saxena BN, Emerson K Jr, Selenkow HA. Serum placental lactogen [HPL] levels
as an index of placental function. N Engl J Med 281:255, 1969)
|
Other protein hormones have been reported to be produced in the placenta: human
chorionic thyrotropin (hCT), human chorionic follicle-stimulating
hormone (hCFSH), and human chorionic corticotropin (hCC). Like hCG
and hPL, they are named for their biologic activity and are similar
to their counterparts produced in the pituitary. Their functions in pregnancy
are unknown. STEROID HORMONES. During pregnancy, there is a gradual increase in the urinary excretion
of progestins and estrogens. This change in steroid metabolism with gestation
is secondary to the biosynthesis of steroid hormones by the placenta
and fetus. Three estrogens are produced by the placenta: estrone, 17β-estradiol, and
estriol (Fig. 13). The primary evidence for their production by the placenta is the fact
that placental fragments incubated in vitro synthesize estrogens from neutral C-19 steroids. The fetus and placenta
must be present for the production of the large amounts of maternal
estrogen normally found in serum and urine during pregnancy; thus, the
term fetoplacental unit was coined. The placenta aromatizes the androgens dehydroepiandrosterone, androstenedione, and
testosterone, produced by the fetus, to estrogens. This
process takes place in the placental microsomes and is catalyzed
by cytochrome P-450. The synthesis of estrogen is known to be stimulated
by hCG and hPL, and the placenta may regulate its own estrogen
synthesis.  Fig. 13. Structures of estrone, 17β-estradiol, and estriol. Fig. 13. Structures of estrone, 17β-estradiol, and estriol.
|
The function of the elevated estrogen level during pregnancy is unknown, except
that it seems to stimulate growth of the uterus, particularly
the myometrium and its vascular supply, as well as the breasts. However, the
elevated levels of estrogen, which rise progressively to term, form
the basis for the best clinical test available for assessing fetoplacental
well-being. Most of the estrogens formed are excreted in the urine bound to glucuronate
or sulfate. Excreted estrogens are estriol, 80%; estrone, 15%; and
estradiol, 5%. In the biosynthesis of estriol, one of the steps, 16α-hydroxylation, takes
place only in the fetal adrenal gland. Therefore, absence
of the fetal adrenal gland (as in anencephaly) or chronic
maternal illness causing fetoplacental deprivation lowers the amount
of estriol, and thus total estrogen, excreted in maternal urine. Maternal 24-hour
urinary estriol excretion is a valuable screening test for
fetal well-being in patients with diabetes mellitus, chronic renal disease, and
hypertension (Fig. 14). It is also helpful in estimating fetal maturity.  Fig. 14. Urinary estriol excretion. Shaded area represents normal range. I: Normal
excretion. II: Borderline excretion. III: Normal with fall near term. IV: Consistently
abnormal values.(Greene JW Jr, Beargie RA, Clark BK et al. Correlation of estriol patterns
of pregnant women with subsequent development of their children. Am
J Obstet Gynecol 105:730, 1969) Fig. 14. Urinary estriol excretion. Shaded area represents normal range. I: Normal
excretion. II: Borderline excretion. III: Normal with fall near term. IV: Consistently
abnormal values.(Greene JW Jr, Beargie RA, Clark BK et al. Correlation of estriol patterns
of pregnant women with subsequent development of their children. Am
J Obstet Gynecol 105:730, 1969)
|
Progesterone is also synthesized in large amounts by the placenta, using
maternal blood cholesterol as the principal substrate, whereas the fetus
contributes very little to the total progesterone production. Progesterone
and its metabolites (Fig. 15) are found in maternal serum and urine as long as the placenta is in situ and functioning. Near term, the human placenta produces about 250 mg of
progesterone daily, of which about 75 mg are delivered to the fetus
for adrenal biosynthesis of steroid hormones. The mechanism regulating
progesterone synthesis is unknown. Pregnanediol is the primary urinary
excretion product; however, it is unreliable as proof of progesterone
level, because it can also be derived from other sources such as deoxycorticosterone. The function of progesterone is unclear. It apparently aids in ovum transport
through the fallopian tube and definitely prepares the endometrium
for implantation. However, these events happen before progesterone
levels begin to rise during pregnancy. Progesterone inhibits uterine
muscle contractility and may have a major role in blocking the onset of
labor. Progesterone promotes gland development in the breast and has
an antialdosterone effect on the kidney. Normal levels fluctuate so much
that this action is of questionable importance. Urinary pregnanediol
levels have been used in the clinical assessment of pregnancy but are
less reliable than estriol levels. |