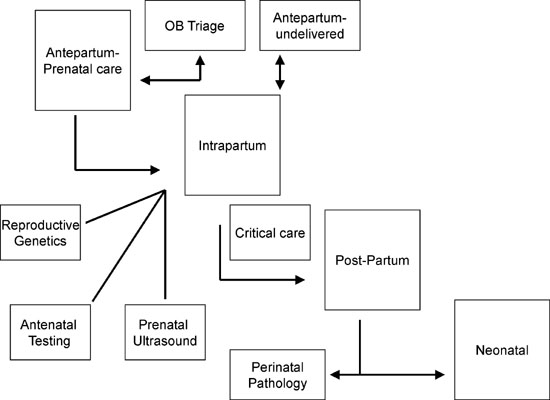
Regardless of the technology used, careful planning must be done to ensure that the perinatal EMR, whether purchased as an off-the-shelf product or developed as a “home-grown product,” has adequate performance and features to justify the large financial commitment that is often required. In the following section, we describe the architecture and framework for one section of our perinatal EMR (Fig. 1) to illustrate key concepts. Beginning in 2001 we have been in the design and development phase of the WIND (Woman, Infant, and Neonatal Database) System. It is a comprehensive Web-based EMR that only requires the user to have access to a Web browser. Security is handled with password protection, role-based navigation, and data encryption with secure socket layering. The two modules that we describe are within the Reproductive Genetics portion of our EMR. They include a First Trimester Genetic ScreeningModule and Multidisciplinary Dysmorphology Database Module We have chosen these as examples because they combine several aspects of data (clinical, biochemical laboratory results, ultrasound images) and are important for both clinical patient care and research.
|
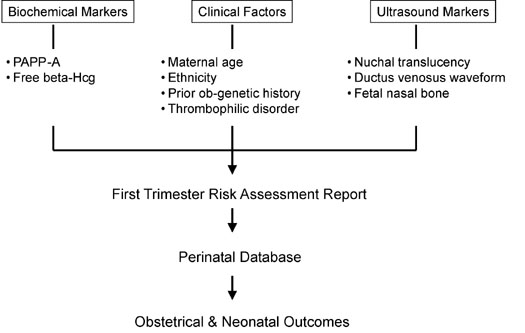
There is significant interest in the combined use of biochemical and ultrasound markers in the first trimester for the detection of aneuploidy. Results from several large multicenter trials suggest that research in this area will continue and clinical practice has already changed with widespread use of nuchal translucency measurements. In order to continue to prospectively collect useful research data, as well integrate the available clinical information, we created within our Perinatal EMR an “Integrated” First Trimester Genetic Screening Module. This module combines maternal demographic and clinical data, maternal biochemical markers, first trimester ultrasound markers, and results of invasive genetic tests (Fig. 2). It will display maternal age, maternal serum free β-human chorionic gonadotropin (β-hCG) and pregnancy-associated plasma protein–A levels, ultrasound images of nuchal translucency measurement, ductus venosus waveform, and fetal profile for identification of the nasal bone in one report. It will also provide risk assessment based on these individual markers or in combination, as well as normative and/or adjusted values. For both quality-control purposes, a digital image of each ultrasound marker will be part of the report. Finally, it will have the ability for easy expansion and incorporation of new tests as they are developed.
|
Integration and dissemination of this information to genetic counselors, reproductive geneticists, maternal-fetal medicine specialists, and sonographers will continue to promote collaboration between these disciplines and improved patient care. As more data are collected from ongoing clinical trials and clinical strategies are evaluated, this Integrated Genetic module will serve as a computer-based clinical support system that provides a specific patient risk which is based on ethnicity, maternal age, serum screening tests, and ultrasound markers.
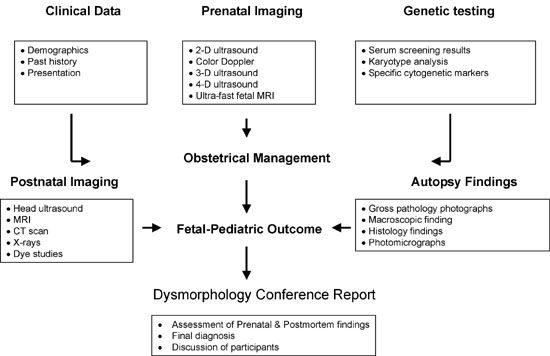
The second example is our Multidisciplinary Dysmorphology Database. This Web-based database combines data input from maternal-fetal medicine, prenatal imaging, reproductive and pediatric genetics, pediatric dysmorphology, and perinatal pathology (Fig. 3). For each case, clinical information and cytogenetic results are linked with prenatal images from 2D ultrasound, 3D/4D ultrasound, and ultrafast fetal magnetic resonance imaging (MRI). Finally, perinatal pathologists contribute autopsy data including photographs of gross pathology, results of other postmortem imaging studies (radiography, dye studies, MRI), and histology findings. All cases are electronically archived and users with permission are able to search cases by ultrasound and/or cytogenetic findings, by diagnosis, and finally by key word(s). Interesting or difficult cases are presented at a monthly Dysmorphology Conference. This interdisciplinary approach has been successful at other institutions.5
|