Under direction of the XX karyotype, the ovary differentiates from the early genital ridge on the posterior wall of the celomic cavity during the sixth week of gestation. The celomic cavity is lined by a mesothelium, which specializes to form the serosal epithelium of the ovary. The mesothelial lining lateral to the genital ridge invaginates, forming the müllerian ducts from which the fallopian tubes, uterus, and upper vagina arise.
The serosal or germinal epithelium extends into the ovarian stroma to form inclusion glands and cysts. This, in addition to the stigmata of ovulation, imparts the characteristic wrinkled surface appearance of the adult ovary. It is generally accepted that the common epithelial tumors of the ovary arise from this single layer of flattened cells referred to as the serosa. Epithelial tumors have various cell types, which reflect the metaplastic potential of the differentiated mesothelial tissue. Cell types in decreasing order of frequency are as follows: (1) serous, resembling Fallopian tube; (2) mucinous, resembling endocervix; (3) endometrioid, resembling endometrium; (4) clear cell, resembling endometrial glands in pregnancy; and (5) Brenner tumors, exhibiting urothelial metaplasia.
Anatomic Considerations
The ovary is an almond-shaped organ that lies on the pelvic sidewall in the shallow peritoneal fossa of Waldeyer, which is marked by the angle formed between the external iliac vein and the ureter. The average dimensions of the ovary in women of reproductive age are 3.5 × 2 × 1.5 cm, decreasing to 2 × 1 × .5 cm in postmenopausal women. It is attached to the uterus by the ovarian ligament, to the posterior leaf of the broad ligament by the mesovarium, and to the pelvic sidewall by the infundibulopelvic ligament. The blood vessels, lymphatics, and nerves exit and enter the ovary at the hilum. The hilum projects into the medulla, which is surrounded by the ovarian cortex.
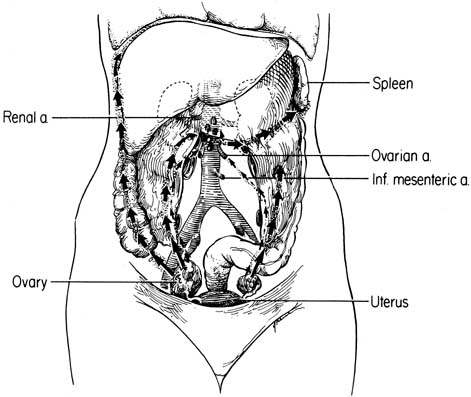
The ovaries have the most extensive lymphatic drainage of all the pelvic organs. Injection of dye into the ovarian stroma outlines a rich lymphatic network that drains the external theca of the follicles and corpora lutea converging on the hilus.2 As the lymphatic channels approach the hilus, they envelop the ovarian veins in a helical pattern. Six to eight collecting lymphatic trunks converge in the mesovarium to form the subovarian lymphatic plexus. The plexus also receives efferent channels from the Fallopian tube and uterine fundus. The lymphatics then follow the ovarian vein in the infundibulopelvic ligament. They traverse the ureter and external iliac artery with the ovarian vessels and continue cephalad, lateral to the ureter. At the lower pole of the kidney they turn medially, cross the ureter, and enter the periaortic nodes at the level of the renal hilus (Fig. 1). Although the primary drainage is the periaortic nodes, accessory channels that traverse the broad ligament are present, draining into the upper interiliac nodes in 25% of patients. Retrograde flow may also occur by the uterine fundal and tubal lymphatics to the inguinal nodes when the normal lymphatic flow is disrupted.
|
A review of the lymphatic drainage of the peritoneal cavity is necessary to explain common sites of involvement in advanced disease. When a tumor cell or particle is injected intraperitoneally into experimental animals or humans, the particle is removed almost exclusively by the lymphatic plexus lining the inferior diaphragmatic surface. In humans, this is densest in the muscular portion of the right diaphragm. The right paracolic gutter is the main pathway of flow from the pelvis to the abdomen. Flow in the left paracolic gutter is impeded by the phrenicocolic ligament that fixes the colonic splenic flexure to the left hemidiaphragm. This cephalad migration is related to negative subphrenic pressure generated with respiration, intestinal peristalsis, and position of the small bowel mesentery. From the diaphragmatic lymphatics, peritoneal lymph is carried by retrosternal lymphatics to the anterior mediastinal nodes. These drain to the right thoracic duct that empties into the right subclavian vein. The right thoracic duct receives 80% of the peritoneal lymph, with the remainder being carried by diaphragmatic lymphatics to the perihilar pulmonary node, thoracic duct, and upper lumbar retroperitoneal nodes.
Natural History
The natural history of early ovarian cancer is unknown. Early disease is a silent, asymptomatic process, and most cases are diagnosed incidentally. There are no known precursor lesions to ovarian cancer, and the time interval required for disease localized to the ovary to disseminate is unknown. Several authors have noted distinct histologic features in the ovaries considered to be at increased risk for ovarian carcinoma and suggest that this association may represent a precursor lesion similar to other epithelial dysplasia found in the female genital tract. Gusberg and Deligdisch3 identified three ovarian cancer patients with identical twin sisters; the unaffected sisters underwent prophylactic oophorectomy after menopause, and their ovarian surface epithelium was found to have histologic features such as stratification, loss of polarity, and nuclear pleomorphism, which are suggestive of a preneoplastic disorder. Fraumeni and colleagues4 described similar changes in ovaries from ovarian cancer prone families, as did Werness and colleagues5 and Dyck and associates.6 Salazar and coworkers7 and Lu and associates,8 in separate studies, examined the ovaries of women known to be at high risk by either positive linkage analysis to BRCA1 or BRCA2 or strong family history, and not only found these histologic changes but also identified unanticipated microscopic malignant neoplasms. Mittal and associates9 adopted a slightly different tactic, examining the contralateral ovary in patients with unilateral ovarian carcinoma, and found a statistically significantly increased number of inclusion cysts within the normal ovaries of cancer patients compared with age-matched controls. In a retrospective review, Plaxe and coworkers10 found nuclear atypia and cellular atypia in noncancerous tissue adjacent to the primary ovarian tumor in stage I cancers, whereas Zheng and partners11,12 identified molecular characteristics of high-grade carcinomas in histologically benign or low-grade malignant tumors adjacent to high-grade ovarian carcinomas. This association may represent a precursor lesion similar to other epithelial dysplasia found in the female genital tract.
The natural history of early ovarian cancer could alternately be explained by multifocal tumorigenesis, with multiple tumors developing simultaneously in the peritoneal epithelium or unifocal tumorigenesis when the tumor develops in the ovary and spreads to other sites. Woodruff and Julian13 studied a large number of ovarian malignancies thought to be metastatic, but after review of histology and analysis of survival, they reclassified them as synchronous primary lesions. Russell and colleagues14 reviewed 128 cases of primary ovarian carcinoma. They found 8 of 10 (80%) borderline carcinomas and 37 of 75 (49%) invasive serous carcinomas to have evidence of independent primary neoplasia at more than one anatomic site.
Several recent molecular biologic studies indicate that invasive ovarian cancer is indeed unifocal in origin, however. Polymerase chain reaction (PCR)-based methods have revolutionized the ability to copy fragments of nuclear DNA and have allowed much more precise evaluation of cancer tissues than was available to Woodruff and Julian in 196913 or even Russell and coworkers in 1985.14 These fragments of DNA can serve as unique genetic fingerprints that may be used to trace the origin of cells. DNA from cancer specimens, duplicated precisely to measurable quantities, can be analyzed for alterations when compared with specimens of normal controls. Early in the use of PCR techniques, the genome was searched for areas of frequent loss of heterozygosity (LOH); if cancer specimens consistently showed LOH in a specific region and the normal controls did not, this suggested the possible presence of a gene related to tumorigenesis. As the genome has become better understood, a library of such regions has developed. Researchers have shown identical patterns of allelic loss, identical patterns of X-chromosome inactivation, and identical codons involved in the mutation of the p53 gene in stage III serous ovarian cancer collected from the primary tumor and metastatic sites from the same patient.15,16,17 This suggests a unifocal origin of serous ovarian carcinoma in more than 90% of cases. Newer molecular biologic techniques have been employed in papillary serous carcinoma of the peritoneum to determine whether these tumors are unifocal or multifocal in origin. Unlike the published experience with invasive ovarian cancer, papillary serous carcinoma of the peritoneum appears to be multifocal in origin, based on differing patterns of allelic loss, X-chromosome inactivation, and p53 mutation at different tumor sites within the same patient.18,19,20,21
Recent advances in cell biology and molecular genetics have been applied to the study of ovarian cancer to elucidate genetic events involved in the malignant transformation of ovarian epithelium. There appear to be two classes of genes associated with tumorigenesis. Protooncogenes are normal cellular genes involved in regulation of cell growth and differentiation. Protooncogenes may be activated by point mutation, gene amplification, or translocation. More than 60 oncogenes have been described in various tumors. Although oncogenes tend to behave in a dominant manner, activation of a single oncogene is unlikely to result in malignant transformation of the cell. Thus far, no single mutation has been found common to all epithelial ovarian cancers, even when histologic subtypes have been examined separately. The heterogeneity of the genetic mutations involved in ovarian tumorigenesis has further complicated the understanding of the natural history of ovarian cancer. Tumor suppressor genes, which constitute the second class of genes, exert inhibitory effects on normal cell growth and differentiation. Inactivation of tumor suppressor genes leads to unregulated cell growth. These genes usually act in a recessive fashion, requiring inactivation of two alleles before an alteration of the gene product can be realized. This model of gene mutation led to the study of loss of heterozygosity at specific chromosomal sites as a guide to identify potential tumor suppressor genes.
Some oncogenes encode for growth factors or growth factor receptors that may act as self-stimulants (exhibiting autocrine control), or stimulants of nearby cells (paracrine control), or stimulants of distant cells (endocrine control). Other oncogenes perform critical roles in intracellular signal transduction. Protooncogenes studied in ovarian cancer include K-ras, Her-2/neu, epidermal growth factor receptor, c-fms, and c-myc. K-ras is the most commonly identified proto-oncogene in human carcinomas.22 Mok and coworkers showed that K-ras mutations are found in borderline and invasive ovarian tumors but noted a nonuniform distribution of mutations when compared by histologic classification.23,24 In both borderline and invasive ovarian tumors, K-ras mutations occurred more commonly in mucinous than in serous tumors. K-ras mutation was observed in approximately 50% of mucinous tumors, regardless of grade or stage, whereas most ras mutations identified in tumors of serous differentiation were found in stage II or III invasive disease.25,26,27 These data suggest that the K-ras mutation may be involved in mucinous differentiation of ovarian epithelial tumors. Given the relatively small prevalence of mucinous ovarian cancers, ras abnormalities are overall less frequent among invasive ovarian cancers (<20%) than among cancers that arise at other sites, such as the pancreas (>90%).
The amplification and overexpression of the Her-2/neu proto-oncogene in approximately 30% of ovarian cancers were first reported by Slamon and associates.28 This was shown to be associated with poor survival rates not only in association with ovarian cancer but also in cervical, vaginal, vulvar, and breast cancer.28,29,30,31,32 Expression of EGF-R occurs in normal ovarian epithelial cells. Continued expression of EGF-R in advanced ovarian carcinoma has been associated with a poor prognosis.33 Experiments with EGF-R ligands have attempted to define a possible autocrine loop that may regulate ovarian cancer growth.34 The c-fms protooncogene codes for the colony-stimulating factor-1 (CSF-1) receptor. An in situ hybridization study of 23 benign and malignant tumors showed that c-fms expression was associated with high-grade advanced stage tumors.35 Amplification and overexpression of the c-myc protooncogene has been demonstrated in ovarian cell lines and tumor biopsy specimens.36,37 No chromosomal rearrangement of c-myc has been demonstrated.38,39
Cytokines in the ovarian stroma, follicular fluid, and tumor-associated macrophages might affect growth of ovarian cancer cells through paracrine regulation. Tumor-associated macrophages produce interleukin-1 (IL-1), IL-6, and tumor necrosis factor (TNF), all of which can stimulate a fraction of ovarian cancers.40 Both IL-1 and TNF induce endogenous production of TNF by ovarian cancers,41 which is associated with increased proliferation in 20% to 40% of cancers.42 TNF can stimulate, inhibit, or fail to affect growth of ovarian cancers among different persons.
Loss and inactivation of tumor suppressor genes in epithelial ovarian cancer also have been reported. Most research has focused on the p53 gene because it currently is the most commonly detected genetic lesion in human cancer.43,44 The p53 gene codes for a nuclear protein that is normally found at low levels in virtually all cells. In general, the mutant p53 gene codes for a variant p53 protein, causing a conformational change that prolongs the half-life from minutes to hours.45,46 This accumulation of p53 protein is an approximate indicator of altered p53 function. Kohler and colleagues,47 Millner and associates,48 and Berchuck and coworkers,49 using immunostaining of the p53 protein, demonstrated overexpression of the p53 protein in 0% (none of 17) of benign tumors, in 4% (2 of 49) of borderline tumors, and in 16% of early-stage (stage IA/IB) epithelial ovarian cancers. Using DNA sequencing, Marks and associates50 showed p53 mutations in 44% (29 of 66) of invasive epithelial ovarian carcinomas; however, analysis of the distribution of point mutations has not identified a particular mutation site. The pattern of mutation differs from that observed in colorectal, hepatocellular, and lung cancer, in association with which it has been possible to identify a statistically significant increase in specific transitions or transversions of the p53 gene.43,51,52 The progression of increase in p53 mutation or overexpression in epithelial ovarian neoplasms implicates p53 in the malignant transformation of ovarian cancers, whereas it may not be important for the development of borderline histologic changes.53
An alternate approach to the identification of genetic changes involved in the pathogenesis of ovarian cancer is to examine differentially expressed genes from normal ovarian epithelium compared with those from ovarian carcinoma cells. Mok and coworkers,54 using a RNA-fingerprinting approach, cloned two cDNA fragments (DOC-1 and DOC-2) that were present in normal ovarian surface epithelial cells but absent in most ovarian cancer cell tissues. The potential functional role of these genes represents an area of active research. The introduction of cDNA array technology has allowed simultaneous investigation of many potentially differentially expressed genes and may facilitate the search for clues to ovarian carcinogenesis.
Malignant transformation of normal ovarian epithelium may be multifactorial; some factors that may increase angiogenesis are separate from those factors that allow for invasion of cells through the basement membrane, which in turn are distinct from factors affecting apoptosis. Taken together, these factors may affect pathogenesis of an individual ovarian cancer. Some researchers have examined the matrix metalloproteinases (MMPs),55,56,57,58 a group of proteins that increase the invasive potential of a cancer by breaking down the basement membrane, using immunohistochemical techniques. MMP expression has been noted to increase in invasive ovarian cancer. It is also thought that to be able to invade, a cancer may also need to emit signals increasing local angiogenesis; such signals are an active area of research, because their identification carries implications for therapeutic intervention. Those particular factors that bring about or allow the overgrowth of cells as well as the invasion of these cells across tissue planes continues to be a focus of intense molecular research.
Dissemination
Spread patterns of ovarian cancer have been well established by careful surgical assessment of the extent of disease by exploratory laparotomy. Spread most commonly occurs by direct extension to the serosal surfaces of other pelvic organs or by exfoliation of cells into the peritoneal cavity with secondary implantation of viable cells. Expression of certain adhesion molecules (e.g., CD44H) by ovarian cancer cells can be important for adhesion of ovarian cancer cells to the peritoneal mesothelium.59 Malignant cells can be exfoliated even when the ovarian capsule appears uninvolved.60 Knowledge of the transport of particles from the peritoneal cavity explains the high frequency of diaphragmatic metastasis. Rosenoff and coworkers61 at the National Cancer Institute performed laparoscopy within 1 month of exploratory laparotomy in 49 consecutive patients as part of a pretreatment evaluation. Seven of 16 (stages I and II) patients were found to have diaphragmatic metastasis. In a prospective study of stage I to III patients by the Gynecologic Oncology Group,62 the commonest sites of visceral metastasis were the rectosigmoid (22.4%), the uterine serosa (11.2%), the small intestinal serosa (9.6%), and the serosa of the bladder (4.3%). This study highlighted the poor correlation between clinical impression and pathologic findings in early-stage disease. Clinical impression of omental disease was inaccurate in 45% of the specimens sampled. Similar inaccuracy of clinical impression was reported for metastatic diaphragmatic disease (50%), pelvic nodes (71%), and para-aortic nodes (96%). Patients reexplored for staging in the Gynecologic Oncology Group study increased in stage in 13 of 58 (22.4%) procedures. This highlights the importance of accurate surgical staging at the time of initial exploratory laparotomy.
The commonest surgical finding is advanced disease with extensive metastatic implants involving the intestinal serosa, omentum, colonic gutters, and peritoneum. Peritoneal dissemination is common; in an autopsy series, this occurred in 75 of 86 (87%) patients.63 Gastrointestinal dysfunction commonly results from diffuse serosal involvement that may encase intestinal loops. Involvement of the mesentery tethers the bowel in addition to disrupting the myenteric plexus, further impairing intestinal motility. Ascites aggravates gastrointestinal dysfunction through external compression of intestinal loops, even further limiting mobility. Inanition is a common terminal event.
Ovarian carcinoma is the commonest cause of malignant ascites in women. Ascites results from disruption of the fine equilibrium between the formation and reabsorption of peritoneal fluid. This has been shown to be causally related to the obstruction of diaphragmatic lymphatics by tumor thrombi in the murine ovarian carcinoma model.64 Coates and associates65 studied the pathogenesis of malignant ascites by mediastinal lymphoscintigraphy with labeled sulfur colloid. In normal patients, after intraperitoneal injection of labeled sulfur colloid, diaphragmatic and retrosternal lymphatics were identified clearly on gamma scans. In 21 of 23 patients with malignant ascites, complete diaphragmatic lymphatic obstruction was demonstrated by lack of colloid activity above the diaphragm after intraperitoneal injection of labeled colloid.
Distant spread is relatively uncommon because ovarian cancer tends to remain within the abdominal cavity throughout most of its natural history. The largest autopsy series of 381 patients with epithelial ovarian cancer by Rose and coworkers66 revealed distant metastasis to be associated with nodal metastasis. The commonest sites of distant metastases in decreasing order were the liver (48%), lung (38%), pleura (28%), bone (12%), skin (5%), and brain (3%). Since the introduction of platinum-based chemotherapy and, hence, improved survival, incidence of extra-abdominal metastases has increased, particularly to the lung and brain.67,68 In patients presenting with distant metastases, the clinician must exclude other possible primary sites.
Preoperative Evaluation
Taking the history and physical examination remain the first steps in the evaluation of patients with possible ovarian cancer. Asymptomatic enlargement of the ovary is common, with pain developing only as a complication related to torsion, infection, or infarction. With progressive increase in ovarian volume, symptoms related to compression of adjacent organs develop insidiously. Since the 1960s, there has been minimal variation in the presenting signs and symptoms of patients with ovarian carcinoma. The American College of Surgeons' national survey of 12,316 ovarian cancer patients identified the commonly found presenting symptoms to be abdominal pain (53%), abdominal swelling (45.8%), bloating or dyspepsia (22%), and pelvic pressure (18%).69 Similar symptoms were reported by Kent and Mckay70 in their survey of 349 ovarian cancer patients at the Boston Hospital for Women in 1960. In both surveys, approximately 50% of patients had ascites or an abdominopelvic mass. In the national survey,69 other signs included abdominal mass (37%), ovarian mass (18%), and pleural effusion (14%). The prevalence of abnormal vaginal bleeding has long been debated, ranging from 5% to 36%.71 Vaginal bleeding occurred in 14% of current patients and may represent concurrent endometrial pathology or activation of the endometrium by hormone-secreting ovarian tumors.69 Patients dying of ovarian cancer were found to have delayed seeking evaluation for symptoms for an average of 13 months; the physicians' delay in diagnosing the cancer was an average of 1.6 months.72 Such delay may occur because of the insidious onset of symptoms and the very common occurrence of similar symptoms in functional disorders. To avoid a delay in diagnosis, health care providers must maintain a high index of suspicion of ovarian cancer in women between the ages of 40 and 60 with unexplained gastrointestinal symptoms.
After a pelvic or abdominal mass has been discovered, evaluation is focused on the exclusion of other possible primary lesions and the preparation of the patient for surgery. Preoperative testing should include a complete blood count, liver function tests, blood urea nitrogen, creatinine, urinalysis, stool guaiac, a chest radiograph, and a baseline electrocardiogram. None of these tests is diagnostic of ovarian cancer, but they do help screen patients for coexistent medical disease that may increase operative risks. The need for further radiologic testing should be individualized based on the patient's history and physical examination. Pelvic ultrasound may be used to confirm the presence of a mass and may be able to localize its origin, but it does not obviate the need for surgery. In patients with no discernible pelvic mass but with ascites or omental caking or both, abdominal computerized tomographic scanning is useful to assess the upper abdominal organs and the gastrointestinal tract to exclude gastrointestinal, liver, pancreatic, renal, or adrenal primary sites. Diagnostic paracentesis is rarely indicated because cytology may be falsely negative and because a positive finding of adenocarcinoma does not provide any information about the primary site. Mammography may be useful in a search for a primary lesion but, again, it may not obviate the need for surgery even with positive findings. Breast cancer patients who present with new findings of an adnexal or pelvic mass are more likely to have a new ovarian or tubal malignancy than metastatic breast cancer by a ratio of 3:1.73 The diagnosis of ovarian cancer is established through exploratory laparotomy, with pathologic and histologic examination of the ovarian primary or metastatic lesions.