The classification of serous neoplasms of the ovary presented in this chapter, unlike the World Health Organization (WHO) classification,1 categorizes the proliferative noninvasive epithelial ovarian neoplasms as atypical proliferative tumors rather than borderline or of low malignant potential. The borderline category of ovarian epithelial tumors was introduced in the early 1970s to describe a group of tumors that did not display overtly malignant features but that occasionally appeared to behave in a malignant fashion.2,3 Their behavior appeared to be intermediate between benign cystadenomas and frank serous carcinomas. The International Federation of Gynecology and Obstetrics (FIGO) committee charged with the development of the classification, which subsequently was adopted by the WHO, stated that this “intermediate” group may be composed of different types of tumors but that the differences could not be discerned.3 The classification was therefore viewed as provisional, but with its continued use over the past 3 decades, the borderline category has become firmly entrenched and is now regarded as a specific entity. Although it has been recognized for many years that the category includes a heterogeneous group of tumors, it is only recent studies that have clearly documented the biologic spectrum encompassed by the borderline category. Noninvasive serous tumors with a papillary architecture in which papillae display a hierarchical branching pattern are termed atypical proliferative serous tumors (APSTs), whereas those displaying a more complex papillary architecture characterized by delicate micropapillae are classified as micropapillary serous carcinomas (MPSCs). The intermediate behavior of tumors in the borderline group results from the inclusion of benign and malignant neoplasms, thereby creating the illusion of intermediate behavior. With the subdivision of the borderline group into benign and malignant tumors, the need for a borderline category disappears. Investigators who prefer to retain the borderline category cite recurrences and deaths in a minority of patients.4 They also maintain that, in at least some, peritoneal implants reflect spread from the ovarian tumors, that microinvasion indicates transformation to bona fide carcinoma, and that some associated lymph node lesions represent metastases.
The literature shows that assessment of the prognosis of APST and MPSC requires evaluation of the peritoneal implants that often accompany serous ovarian tumors. 5 Studies over the past 20 years6 have shown that classifying implants as invasive or noninvasive plays a critical role in determining prognosis. Patients whose tumors are associated with noninvasive implants have a 10-year survival that is close to 100%.6–8 In contrast, patients whose tumors are associated with invasive implants have a mortality rate of 34% after more than 7 years of follow-up.6 The difference in survival for patients with invasive versus noninvasive implants is highly significant and supports the subclassification of implants for clinical management.
Benign Serous Tumors
Benign serous tumors include cystadenomas, adenofibromas, cystadenofibromas, and surface papillomas. These tumors are common, accounting for approximately 25% of all benign ovarian neoplasms and 58% of all ovarian serous tumors. In patients, the peak incidence is in the 4th and 5th decades, and the median age is 41 years. The symptoms and signs are nonspecific and most commonly include pelvic pain, discomfort, or an asymptomatic pelvic mass discovered on routine examination. Bilaterality rates are in the range of 12% to 23%.
Cystadenomas are composed of cysts filled with clear, watery (serous) fluid or thin mucoid material. Occasionally, they contain thick mucus-like material more typical of mucinous neoplasms. The external surfaces of the cysts are smooth and glistening, often with a prominent vascular pattern. Occasionally, small papillary excrescences are found on the external surface of the cyst. The tumors may be unilocular or multilocular and vary in size up to 30 cm, with a median of 9 cm. The lining of the cyst is either entirely flat or may have a varying number of coarse papillary projections. Such papillary excrescences rarely cover the entire inner surface of the cyst. Cystadenofibromas are solid neoplasms composed of tough, rubbery tissue with interspersed glandular spaces.
Normal-sized ovaries often have small papillary projections with a fibrotic stromal component resembling a microscopic adenofibroma or cystadenofibroma arising from the surface; furthermore, simple germinal or cortical inclusions may become cystically dilated. Therefore, it has been suggested that serous neoplasms be diagnosed only if the lesion is greater than 1 cm in diameter.9 This is obviously arbitrary and therefore is unlikely to distinguish true examples of neoplastic growth from simple serous cysts or nonneoplastic hyperplasias of the ovarian cortex.
There is a broad spectrum of epithelial proliferation in benign serous tumors that is manifested by variation in the prominence and complexity of the papillae, from a simple, single layer and blunt papillae to focal epithelial stratification and detachment of cell clusters approaching the degree of proliferation seen in APSTs. Identification of these features in 10% of the histologic material is the boundary between a cystadenoma and an APST. Cystadenomas are generally lined by a single layer of flattened-to-cuboidal cells with uniform basal nuclei. In addition, the epithelial cells can be pseudostratified and tubal in type, with the characteristic elongated (secretory cell) or rounded (ciliated cell) nuclei. In large cysts, the epithelium often becomes attenuated because of the pressure exerted by the cyst contents. Mitoses and atypia are generally absent. Psammoma bodies are present in the stroma in 15% of cystadenomas.
The stroma of benign serous tumors can resemble normal ovarian stroma but is generally more fibrous. When the stroma is highly cellular and fibrous, the tumor can be designated as an adenofibroma.
A variety of benign cysts may occur in and around the ovary and broad ligament and may simulate serous cystadenomas, both grossly and microscopically. These include functional ovarian cysts, endometriotic cysts, hydatid cysts of Morgagni, mesonephric cysts, and mesothelial (peritoneal) cysts. Any of these cysts, if large, may adhere to or compress the ovary, thus suggesting an ovarian origin. Because serous cystadenomas are benign, unilateral salpingo-oophorectomy or ovarian cystectomy is adequate treatment. Recurrence is extremely rare and reflects either incomplete resection or a new primary tumor.
Atypical Proliferative (Borderline) Serous Tumors
CLINICAL FEATURES AND OPERATIVE FINDINGS.
Atypical proliferative serous tumors comprise approximately 10% of ovarian serous neoplasms and 56% of ovarian tumors classified as borderline. The clinical features of patients with APSTs are similar to those for serous cystadenomas, except that the mean patient age is slightly older for APSTs compared to cystadenomas.
Nearly 40% of atypical proliferative serous tumors are bilateral. Exophytic papillae reflecting ovarian surface involvement are common and are more often found in patients who also have peritoneal implants.10
The APSTs are often associated with serous-type lesions involving the peritoneum. These include endosalpingiosis (benign glandular inclusions), found in 40% of patients,11 and noninvasive implants, found in approximately 30% of patients.6 The latter may appear as granular lesions or fibrous plaques.
PATHOLOGY.
Atypical proliferative serous tumors have gross features similar to cystadenomas but tend to have finer, more friable, and more exuberant papillary projections. Papillae are nearly always present on internal surfaces of the cyst and are present on the external surfaces in up to 70% of cases. The adenofibromatous variant of APST is uncommon and grossly resembles its nonatypical counterpart.
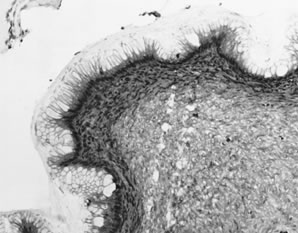
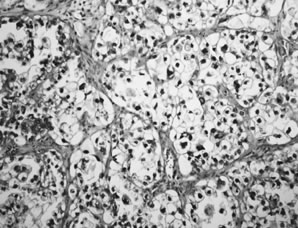
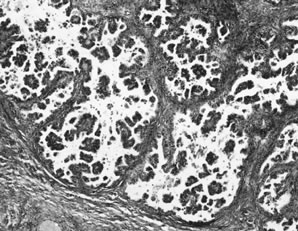
APSTs display extensive epithelial stratification, tufting and detachment of cell clusters, in addition to hierarchical branching with successively smaller papillae emanating from the larger, more centrally located papillae (Fig. 1). The two most easily quantifiable proliferative changes in these tumors are epithelial stratification and the extent of tufting or budding with detachment of cells from the surface. It has been recommended that a serous neoplasm should display stratification and budding in at least 10% of the available material to qualify as an APST.
|
The cells in APSTs show features of epithelial and mesothelial differentiation. Ciliated cells resembling those in the fallopian tube are present in approximately one third of tumors. In addition, cells with abundant eosinophilic cytoplasm and rounded nuclei resembling mesothelial cells are also present, particularly on the tips of the papillae. The nuclei of APSTs resemble those in cystadenomas but tend to display slightly more atypia. Nuclei are basally located and tend to be ovoid or rounded. The chromatin is usually fine, but nucleoli are sometimes prominent. Mitoses are not common and rarely exceed four per 10 high-power fields. Psammoma bodies are present in up to half of APSTs.
The most common type of microinvasion in APSTs is characterized by isolated cells with abundant eosinophilic cytoplasm that appear to be budding from the epithelium into the superficial stromal cores of the papillae.6,12 When carefully searched for, 10% of APSTs contain microinvasion; however, in studies not specifically searching for microinvasion, it has been noted in only 1.3% of cases.6 The survival of 94 patients with microinvasion followed for a mean of 7.4 years was 100%.6 Thus, it is likely that microinvasion is frequently overlooked with no adverse affect on outcome. Although more data are needed, from the standpoint of prognosis and patient treatment, microinvasion at present appears to have no clinical relevance.
The peritoneum in patients with APSTs often contains serous epithelial proliferations displaying a range of proliferative changes: benign glands designated endosalpingiosis, papillary epithelial proliferations, sometimes with stromal desmoplasia, designated, noninvasive implants, and invasive carcinoma, also designated invasive implants. Some patients may have both invasive and noninvasive implants.
Endosalpingiosis, or benign glandular inclusions, may involve the peritoneal surfaces in patients with or without benign or malignant serous ovarian tumors. It is found in 40% of patients with APSTs. These glands typically are lined by simple columnar epithelium, often displaying tubal-type differentiation. The epithelium may display minor degrees of cytologic atypia and form simple papillary structures; psammoma bodies are sometimes present and may persist after degeneration of the associated epithelial structures. Mitotic figures are absent.
Among women with APSTs, 31% have peritoneal epithelial lesions that display a degree of proliferation beyond that usually seen in endosalpingiosis, but that lack features of invasion. These have been designated noninvasive implants and have two morphologic forms: epithelial and desmoplastic. Mixtures of both types are not uncommon.
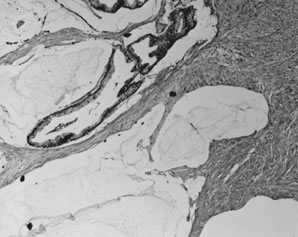
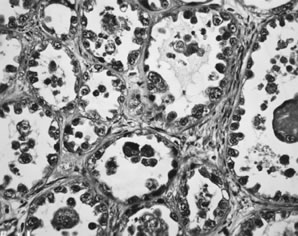
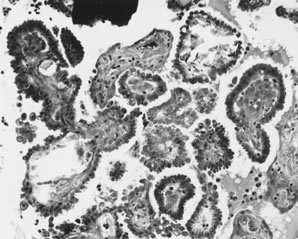
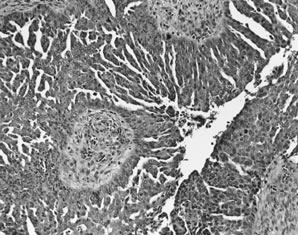
Epithelial implants are papillary and resemble the ovarian APST5,8 (Fig. 2). Mild atypia is often present, and occasionally atypia may be marked. Mitoses are usually absent. Calcification, usually in the form of psammoma bodies, is common and may be extensive.
|
Desmoplastic implants are densely fibrotic lesions that entrap glandlike structures. The characteristic architectural feature of the desmoplastic noninvasive implant is a plaquelike thickening overlying peritoneal surfaces that appears tacked on. They may extend into the septae that separate omental lobules and create a low-power appearance, which is suggestive of invasion. A chronic inflammatory response is usually present, and in 20% of cases, an acute inflammatory exudate overlies the implant. Mitotic figures are usually absent, and psammoma bodies are present in more than 90% of cases.5,8
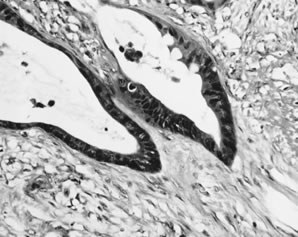
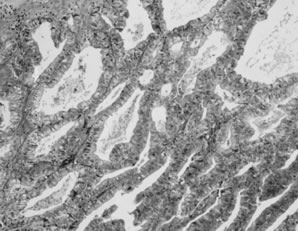
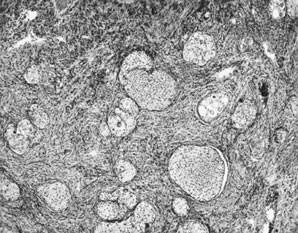
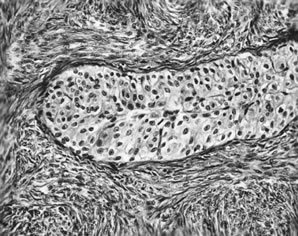
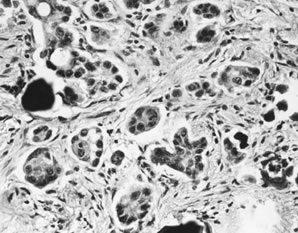
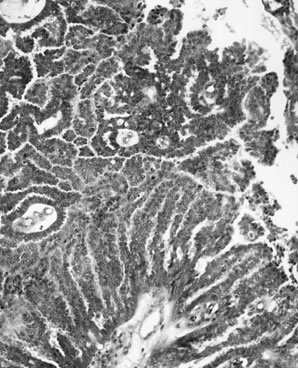
Invasive implants have been reported in association with advanced stage APSTs in approximately 6% of cases. In contrast, they are found in association with nearly half of advanced stage MPSCs (see Micropapillary serous carcinoma below). The characteristic architectural feature of an invasive implant is a haphazard infiltrative growth pattern (Fig. 3). A confluent or cribriform glandular pattern may be present. An exophytic micropapillary pattern, as described below (see Micropapillary serous carcinoma below), also qualifies for the designation of invasive implant (Fig. 4),8 but more often, micropapillae are nonbranched, embedded in fibrous stroma, and surrounded by a clear space or cleft. Sometimes, micropapillae are present within glands and may fuse with one another to create a weblike appearance. Invasive implants often display only mild cytologic atypia, but occasionally atypia is moderate and rarely marked. Mitotic figures are occasionally present. The distinction of desmoplastic implants from invasive implants (carcinoma) may be very difficult at times, but is important since it is this feature that is the best predictor of outcome for tumors with extraovarian disease.
|
|
Lymph node involvement has been reported in approximately 63 cases of APSTs.6 Excluded from consideration is endosalpingiosis involving lymph nodes, which are nonneoplastic glandular inclusions of müllerian type that occur in pelvic lymph nodes of 5% to 14% of unselected women and in 45% to 65% of women with borderline ovarian tumors. The most common type of metastatic lymph node lesion that has been associated with APSTs is characterized by individual cells and clusters of cells with abundant eosinophilic cytoplasm in the sinuses, predominantly subcapsular sinuses. The nature of these cells is unclear, but recently it has been suggested that they may be mesothelial in origin. Similar cells are nearly always present on the surface of primary APSTs and are often present in the stroma of noninvasive desmoplastic implants. It is plausible that these cells exfoliate and are filtered from the peritoneal fluid by regional lymph nodes—so-called deportation.
Identification of lymph node metastases of APSTs has been cited as evidence of malignant potential for APSTs (borderline tumors). However, this conclusion is not supported by the data since the survival rate of 43 reported patients with lymph node metastases is 98% after a mean follow-up of 6.5 years.6
Ovarian epithelial tumors are often heterogeneous, and carcinomas may have benign-appearing areas resembling a cystadenoma or an APST. It should therefore come as no surprise that approximately 20% to 30% of ovarian epithelial tumors diagnosed as atypical proliferative (borderline) at the time of frozen section examination prove to be carcinomas on further sampling. Because 15% of unilateral tumors are associated with extraovarian disease, it is important that the surgeon perform a thorough exploration when the frozen section is diagnosed as an APST, but formal staging is not necessary for a unilateral ovarian tumor unless suspicious peritoneal lesions are found. In contrast, 56% of bilateral tumors are associated with extraovarian disease, and therefore staging in this setting is advisable.10
BEHAVIOR.
The disease-specific survival rate of patients with APSTs confined to the ovaries after a mean of approximately 6.7 years, based on more than 2000 reported cases, exceeds 99.5%.6 As indicated above, survival of 94 reported patients who had tumors that showed microinvasion is 100%, and survival of 43 reported patients with lymph node involvement was 98%.6 In six prospective, randomized trials including approximately 373 patients with serous borderline tumors followed for a mean of 6.7 years, the survival was 100%.6 The behavior of APSTs with extraovarian disease is based on the type of implants that are present. The survival rate of patients with APSTs with noninvasive implants is 95% to 100% after a mean follow-up of 7.4 years.6–8 Recurrences and deaths reported in the literature are poorly documented in the majority of cases.6 When carefully documented, most deaths are either treatment related or are the result of complications from adhesions and bowel obstruction rather than carcinoma. Finally, in a literature review of more than 18,000 borderline tumors, we were unable to identify a single well-documented case of an APST with noninvasive peritoneal implants of which primary ovarian tumor had been adequately sampled to exclude invasion (one section per centimeter of maximum tumor diameter) that had progressed to documented invasive carcinoma,6 although it is conceivable that a noninvasive peritoneal implant can undergo alignant transformation on rare occasions. Among 27 cases that reportedly progressed to invasive carcinoma, none were documented to have been adequately sampled for pathologic examination.6
In general, the noninvasive serous tumors associated with invasive implants are MPSCs, not APSTs. Based on a literature review of 467 noninvasive serous tumors, which included both invasive and noninvasive implants, the survival rate for patients with invasive implants was 66% after a mean follow-up of 7.4 years compared to 95% for patients with noninvasive implants. The difference was highly significant (p < .0001).6 The finding of invasive implants in association with an APST is very unusual and is probably because of inadequate sampling and reflects foci of occult invasion in the primary tumor.
Malignant Serous Tumors
MICROPAPILLARY SEROUS CARCINOMA.
In 1979, Russell and Merkur13 described a noninvasive serous tumor, the morphology of which closely approached the degree of proliferation displayed by low-grade carcinomas but lacked invasion and, therefore, fulfilled the WHO criteria for serous borderline tumor. They designated these tumors as “grade IV proliferating serous tumors.” This pattern was also recognized by others around the same time.14 But despite numerous studies of ovarian borderline tumors or “tumors of low malignant potential” in the ensuing 2 decades, little data on this variant were published until 1996, when two series appeared, 8,15 followed by a third in 1999.7 At this time, some investigators observed that these tumors, despite no apparent evidence of invasion, behaved like low-grade carcinomas in contrast to the other tumors in this group, and therefore proposed that they be designated “micropapillary serous carcinoma”8,15; other investigators preferred the term serous borderline tumor with a micropapillary pattern.7
Because the published data on MPSC are limited to only a few large studies, much of the data describing the clinical presentation, behavior, and treatment of this tumor are preliminary. MPSCs that do not display destructive infiltrative growth are considered noninvasive for purposes of this discussion, although it is conceivable that the complex exophytic micropapillary pattern is a form of invasion.
CLINICAL FEATURES AND OPERATIVE FINDINGS.
The mean age of patients with the noninvasive form of MPSC is 42 years. The most common presentation is an asymptomatic pelvic mass, but abdominal pain, fullness, and distention are common symptoms in advanced stage cases. Sixty-five percent of tumors are bilateral. Forty-seven percent of patients are stage I and the remainder are stages II and III. The mean tumor size is 8.2 cm. Surface involvement is present in 54% of cases.
PATHOLOGY.
Because these tumors are very well differentiated, they tend to have a papillary and cystic gross appearance like APSTs and little, if any, necrosis in contrast to many typical serous carcinomas, which often have solid areas and extensive necrosis. Noninvasive MPSC is a proliferative serous neoplasm that displays a high degree of epithelial proliferation and complexity but is morphologically intraepithelial because diagnostic features of invasion are not present. Some investigators believe that the association of MPSC with invasive carcinoma and a high mortality rate warrants classification of this variant as a well-differentiated papillary serous carcinoma, thus the designation MPSC. In either case, this variant displays a characteristic pattern of papillary branching (Fig. 5). The distal papillary branches are thin and delicate with minimal fibrovascular support and emanate abruptly from thick, more centrally located papillae without intervening branches of successive intermediate sizes, unlike the hierarchical branching pattern of APSTs. The papillae often fuse to form a cribriform pattern. Because micropapillary and cribriform areas may be focally present in APSTs, a 5-mm-in-diameter area of a confluent micropapillary pattern is required for the designation of MPSC; anything less than this, in the absence of other features of invasion, should be classified as an APST. Extensive sampling of the ovarian tumor may be necessary to resolve difficult cases. MPSC displays no apparent invasion of the stromal cores of the papillae. High-grade malignant nuclear features, even in the presence of the typical micropapillary patterns, warrant a diagnosis of ordinary papillary serous carcinoma. Invasion is recognized by a haphazard infiltrative growth composed of solid nests or complex glandlike structures displaying micropapillae or a confluent pattern. The nests, glands, and glandlike structures are often surrounded by a clear space or cleft. Psammoma bodies may be numerous in either the MPSC or invasive areas. The distinguishing morphologic features of serous neoplasms, including the invasive and noninvasive variants of MPSC, are shown in Table 2.
|
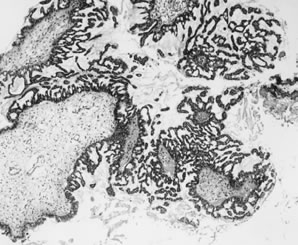
Table 2. Distinguishing Morphologic Features of Serous Ovarian Neoplasms
|
| Stratification and | Micropapillary | Stromal |
Diagnosis | Atypia | Detachment | Pattern | Invasion |
Serous cystadenoma | Absent, or | Absent, or present | Absent | Absent |
| present in <10% | in <10% |
|
|
APST | Present in >10% | Present in >10% | May be present, | Absent |
|
|
| <5 mm of |
|
|
|
| confluence |
|
MPSC, noninvasive | Present | Usually present | Present, >5mm | Absent |
|
|
| of confluence |
|
MPSC, invasive | Present | Usually present | Present | Present |
Serous carcinoma | Present | May be present | May be present | Present |
APST, atypical proliferative serous tumor; MPSC, micropapillary serous carcinomas.
(Seidman JD, Russell P, Kurman RJ: Surface epithelial tumors of the ovary. In Kurman RJ [ed]:Blaustein's Pathology of the Female Genital Tract, pp 791–904, 6th ed. New York, Springer-Verlag, 2002)
The peritoneal implants associated with MPSC are frequently invasive (i.e., carcinoma). Among 39 reported cases of advanced stage noninvasive MPSC, 19 (49%) of the implants were invasive7,8,15 in comparison to 6% of the implants associated with APSTs.8
BEHAVIOR.
Despite the apparent absence of destructive infiltrative growth in the noninvasive variant of MPSC, the limited available data indicate that it behaves as a low-grade serous carcinoma. Stage I MPSC appears to be cured by adnexectomy alone, although only a small number of stage I tumors have been reported. Based on relatively limited data from three studies, the 5- and 10-year survival rates for patients with advanced stage MPSC are approximately 84% and 58%, respectively.7,8,15 Documented recurrences of invasive carcinoma have been reported in 34% of advanced stage MPSCs. One invasive recurrence from an inadequately sampled primary ovarian MPSC that was reportedly stage I but for which slides of the omentum were not reviewed by the authors has been reported. Insufficient data are available on the invasive variant of MPSCs to comment on their behavior.
Invasive Serous Carcinoma
CLINICAL AND OPERATIVE FINDINGS.
Serous carcinoma is the most common type of ovarian cancer and accounts for approximately 50% of malignant ovarian neoplasms. The peak age group is 45 to 65 years, and the mean age is 57 years.16 Inasmuch as 70% to 84% of patients present in advanced stage (FIGO stage II or higher) with tumor disseminated throughout the abdominal and pelvic cavities, common presenting symptoms are abdominal pain and distention due to ascites or bulky abdominal tumor. Gastrointestinal symptoms are also common. Other symptoms may include urinary frequency, dysuria, and vaginal bleeding. Stage I tumors usually present as an asymptomatic mass on a routine pelvic examination.
Two thirds of cases involve both ovaries. For stage I cases, approximately 40% are bilateral. Nearly all advanced stage ovarian carcinomas spread along peritoneal surfaces, including the pelvic peritoneum (stage II), the surfaces of the bowel, and other abdominal organs (stage III). Both pelvic and abdominal spread can be by direct extension or metastasis. For example, direct extension to the rectosigmoid, broad ligament or uterus can occur by contiguous growth, or exfoliation of malignant cells can result in seeding of the peritoneal surfaces of the bowel or pelvic peritoneum. Tumor rupture before or during surgery may occur and warrants assignment of a stage I or II tumor to stage IC or IIC, respectively. Assessment of the character of the external surface is an important component of staging for tumors that are confined to the ovaries. This is best done by the surgeon but should also be evaluated by the pathologist. Grossly exophytic papillary tumor on the surface of an ovarian neoplasm that is confined to the ovaries warrants a stage of IC. Intracystic neoplasms without gross or microscopic tumor on the external surfaces do not qualify for surface involvement unless tumor cells invade through the full thickness of the cyst wall and are thus exposed to the peritoneal cavity. Dense adhesions to pelvic structures or bowel are reassigned to FIGO stage II or III.
Patients with stage III disease usually have omental involvement which, in advanced cases, is manifested by a solid tumorous mass (omental cake). Pelvic and para-aortic lymph node metastases are found frequently, with a direct relationship to the extent of disease. Rarely, inguinal lymph nodes contain metastatic tumor. Patients with tumors that otherwise appear to be stage I have lymph node metastases in 4% to 14% of cases; the corresponding figures for stages II, III, and IV are 36%, 41% to 68%, and 88%, respectively. Liver metastases usually manifest as studding of the peritoneal surface of the liver. Parenchymal liver metastases are rarely present, and very rarely, splenic metastases are found, necessitating splenectomy.
In 8% to 12.5% of women with advanced stage papillary serous carcinoma, the ovaries are small and display predominantly surface involvement; occasionally, the ovaries are completely uninvolved by tumor. These findings warrant a diagnosis of primary peritoneal serous carcinoma.
PATHOLOGY.
Serous carcinomas range from microscopic (referred to as early de novo carcinoma) to approximately 20 cm in diameter. They are typically multilocular and cystic, with soft, friable papillae filling the cyst cavities and containing serous, turbid, or bloody fluid. The external surfaces may be smooth or bosselated and sometimes display surface papillae. Tumors are often solid, pink to gray with less-obvious papillae, and may be soft or firm depending on the character of the tumor stroma. Hemorrhage and necrosis are often present. Omental metastases are characterized by firm nodules of variable size with white or gray cut surfaces, which may coalesce into an omental cake. If the omentum is grossly normal, microscopic omental metastases are found in 22% of cases.
Well-differentiated serous carcinomas are discussed above (see micropapillary serous carcinomas above). Typical serous carcinomas display complex papillary and solid patterns and marked nuclear atypia (Fig. 6). A frequently encountered and quite characteristic pattern is a lacelike or labyrinthine pattern. This pattern may be focal but often predominates and is characterized by extensive bridging and coalescence of papillae, resulting in slitlike spaces between the papillae. Areas of solid growth are common. A glandular pattern is not necessarily diagnostic of endometrioid differentiation, and the distinction of a high-grade endometrioid carcinoma from a serous carcinoma may be difficult. The cells may be small and uniform with grade 2 nuclear atypia, but more often are large, pleomorphic, and display obviously malignant cytologic features.
|
Serous carcinomas that display extensive solid areas are usually composed of uniform sheets of cells with high-grade nuclear atypia and may display isolated bizarre mononuclear giant cells or syncytial-like aggregates. Mitoses, including abnormal mitoses, are usually numerous and necrosis is often pronounced. Areas with grade 2 nuclei often merge with areas of grade 3 nuclei. Nuclear grade is subjective and not very reproducible; we therefore designate these tumors as “high grade.” Usually there are focal areas with papillary architecture that permit the diagnosis of a serous carcinoma as opposed to an undifferentiated carcinoma. Psammoma bodies are present in 25% of cases. A completely solid carcinoma without any evidence of glands or papillae warrants a designation of undifferentiated carcinoma.
When faced with a neoplasm in the ovary, particularly when bilateral, the physician should always consider the possibility of metastatic tumor to the ovary. Although metastatic carcinomas to the ovary most often mimic mucinous or endometrioid ovarian carcinomas, metastases may display a variety of patterns.
Serous carcinomas may invade the fallopian tubes, and on occasion, the distinction of an ovarian from a primary tubal carcinoma may be difficult. Meticulous dissection of the fallopian tube, which is nearly always dilated and filled with tumor when primary, can be of value. Microscopically, the presence of carcinoma in situ in uninvolved tubal epithelium is also helpful.
Grossly normal-sized ovaries with microscopic surface involvement or no involvement by serous carcinoma are classified as peritoneal carcinomas. From a practical standpoint, the distinction is not critical since the behavior and treatment of serous carcinomas of the ovary and peritoneum are similar.
BEHAVIOR.
Stage I patients who have been carefully staged have a 5-year survival rate that exceeds 90%.17 Survival for stages III and IV is generally very poor. Some of the older literature overestimates the survival rate for stage III patients because of the inclusion of borderline tumors. Stage II tumors are uncommon (8% of serous carcinomas) and represent an intermediate group, which, depending on other factors including completeness of surgical removal and substage, can have widely varying survival and cure rates. Early de novo carcinoma, despite its small size, is associated with recurrence and death in approximately a third of cases, usually with widespread peritoneal disease.18