As is often the case in uncommonly diagnosed tumors, accurate information
regarding proper management is rare. Randomized trials addressing the
roles of adjuvant treatment, radical surgery, reassessment laparotomy, and
cytoreduction, as well as the most active drugs or proper radiotherapy
are, at best, lacking. Most of the information addressing these
important questions is either from retrospective or individualized
trials or are extrapolated from information gained from the study of ovarian
carcinoma. The difficulty of studying fallopian tube carcinoma
was expressed by Morris and associates,87 who reported on a phase II adjuvant chemotherapy protocol at the MD Anderson
Cancer Center. This study required 9 years to enroll just 18 patients
in a consistent treatment plan. They argued that the issue of similarity
between fallopian tube carcinoma and ovarian carcinoma should
be addressed first so that, if the natural history of fallopian tube
carcinoma was consonant with that of ovarian carcinoma, the standard
treatment of the latter would be appropriate. The available data regarding
surgical goals, adjuvant treatment with radiation and chemotherapy, and
reassessment operations are presented next. Surgical Goals As previously discussed, the natural history and patterns of spread of
fallopian tube carcinoma most closely mimic characteristics of ovarian
carcinoma. Therefore, it is not surprising that the surgical goals recommended
have been patterned after those now purported for patients with
ovarian carcinoma. The surgical goals recommended have been premised
on the sensitivity of ovarian carcinoma to adjuvant therapy. Now that
a formalized and generally accepted staging format has been published, the
surgical goals are clearly to provide enough information to ascertain
a surgical stage.84 In light of the tumor's usual presentation, this most often involves
removal of the uterus, tubes, and ovaries, along with assessment of
the tumor distribution in the peritoneal surfaces and retroperitoneum. On the basis of the previously mentioned propensity for lymphatic metastases, special
attention should be given to proper sampling of the pelvic
and para-aortic lymphatic chains. There is currently no evidence
to suggest that radical hysterectomy or complete lymphatic dissection
adds to progression-free or overall survival unless it contributes
to the primary tumor's extirpation. It is not uncommon
for patients with otherwise stage I or stage II disease to present with
isolated para-aortic metastatic disease. This clinical feature
may suggest that lymphatic involvement may precede intra-abdominal
metastases. In the series by Tamini and colleagues,57 two of eight patients with lymphatic metastases had disease solely in
the para-aortic chain. Upstaging of clinically confined or localized
tumors is common. In the review by Schray and colleagues,58 five of nine patients with clinical stage I disease were upstaged on the
basis of extrapelvic lymphatic involvement; in the series by Klein
and colleagues,59 three of seven stage II cases were upstaged on the basis of lymphatic
metastases. Review of these data underscores not only the importance of
systematic evaluation, but also the impact of accurate disease status
on treatment decisions. One investigator suggested that patients who
have not been properly staged or explored may undergo successful lymphatic
sampling by laparoscopy.88 The role of cytoreductive surgery has been the focus of several reviews
and appears to confer the same progression-free survival enhancement
as is seen among patients with ovarian carcinoma.15,16,17,61,89 Many reports have used differing definitions of optimal cytoreduction, but the most profound and consistent difference is seen
among patients with no residual disease after attempted cytoreduction. Barakat
and colleagues61 noted among 31 stage II to stage IV patients treated with platinum-based
adjuvant therapy, those with no residual disease after a maximal
cytoreductive effort had a 65% 5-year survival, compared
with a 19% 5-year survival in those described as having any residual(Fig. 4). Similarly, in a review of 71 patients treated at the MD Anderson
Cancer Center with platinum-based and nonplatinum-based
chemotherapy and/or radiation therapy, those with no residual disease
had a 5-year survival of 29% compared with 15% for
those with residual disease less than 2 cm and 7% for residual
disease equal to or greater than 2 cm.15 In a review of 18 patients treated at the same institution with platinum-based
chemotherapy, Morris and associates87 noted that among 15 patients with stage II to stage IV disease, five of
six patients (83%) with no residual were without disease
at follow-up (median survival not reached at 96 months) compared
with only three of nine patients (33%) with
any residual at a median 29 months. Considering the small sample
size, disparate adjuvant therapies, and lack of information on biologic
aggressiveness, it is still appreciated that the effect of complete
tumor resection will likely connote a longer progression-free
survival among patients with stage II to stage IV disease. 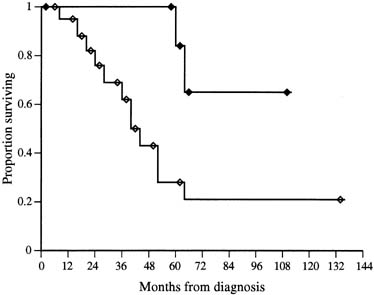 Fig. 4. Survival curves from 33 fallopian tube cancer patients (stages II
to IV) presented by amount of residual disease after a primary surgical
effort. Open diamonds represent patients with any residual disease; closed
diamonds represent patients with no residual disease. These
survival data are significantly different (p = .006). (Adapted from Barakat BR, Rubin SC, Saigo PE et al: Cisplatin-based combination chemotherapy in carcinoma of the fallopian tube. Gynecol Oncol 42:156, 1991.) Fig. 4. Survival curves from 33 fallopian tube cancer patients (stages II
to IV) presented by amount of residual disease after a primary surgical
effort. Open diamonds represent patients with any residual disease; closed
diamonds represent patients with no residual disease. These
survival data are significantly different (p = .006). (Adapted from Barakat BR, Rubin SC, Saigo PE et al: Cisplatin-based combination chemotherapy in carcinoma of the fallopian tube. Gynecol Oncol 42:156, 1991.)
|
Second-look laparotomy has also been evaluated in this patient population (Table 5).15,16,30,57,68,87,90,91,92,93,94,96,97 Guidelines as to use of the procedure and impact on survival are less
well understood and studied than among patients with ovarian cancer. Further, because
of unspecified selection criteria, variant types of adjuvant
therapy, and lack of complete surgical staging data, interpretation
among patients undergoing the operation cannot be precise. Certain
generalizations may be inferred, however, on review of the more than 90 reported
operations performed since 1980. First, findings at this
operation seem to provide some meaningful information about recurrence
and progression-free survival. Among the 58 negative second-look
operations reported, only 12 (20.6%) have recurred. Second, sixty-three percent of the operations were pathologically
negative, although this was most frequently among stage I, grade 1 cases. This
operation is probably not important in this subgroup. The
most consistent prognostic indicator of outcome in this operation
is the amount of residual disease at primary cytoreduction. Third, secondary
cytoreduction on the identification of gross residual disease31,61 probably has little or no effect on overall survival, because no survival
advantage was seen among patients with gross residual disease after
second cytoreduction and those with microscopic residual. Table 5. Outcomes in Second-Look Laparotomy Procedures of Primary
Fallopian Tube Carcinoma
| Author |
No. of Second-Look No. Patients |
No. (%) of Negative Procedures |
No. (%) of Recurrences After Procedures |
Negative Procedure |
| Pectasides et al97 |
017 |
09 |
6 (67)0 |
1 (17) |
| Barakat et al96 |
035 |
35 |
21 (60)00 |
4 (19) |
| Morris et al87 |
018 |
08 |
4 (50)0 |
0 (0)0 |
| Rose et al30 |
064 |
08 |
2 (25)0 |
0 (0)0 |
| Podratz et al16 |
047 |
01 |
0 (0)00 |
0 (0)0 |
| Brown et al95 |
021 |
04 |
4 (100) |
2 (50) |
| Peters et al17 |
046 |
07 |
6 (86)0 |
2 (33) |
| Deppe et al93 |
004 |
02 |
2 (100) |
0 (0)0 |
| Jacobs et al92 |
009 |
03 |
3 (100) |
0 (0)0 |
| Roberts et al91 |
028 |
02 |
2 (100) |
1 (50) |
| Harrison et al90 |
036 |
05 |
1 (20)0 |
0 (0)0 |
| Hirai et al68 |
015 |
01 |
1 (100) |
0 (0)0 |
| Eddy et al15 |
071 |
08 |
5 (63)0 |
2 (40) |
| Tamini and Figge57 |
015 |
01 |
1 (100) |
0 (0)0 |
| Total |
426 |
92 |
58 (63)00 |
12 (21)0 |
In summary, evaluation of disease response to primary therapy may be indicated
on prognostic grounds alone in patients with stage II to stage
IV disease; however, little additional benefit is gained by secondary
cytoreduction among patients without a complete response to primary therapy. Radiation Therapy Supported by early studies suggesting the sensitivity of fallopian tube
cancers to radiation, this modality had been considered a principle asset
of adjuvant therapy.83,98 Several delivery mechanisms have been evaluated, including intraperitoneal
radiocolloids, external orthovoltage and megavoltage radiotherapy, brachytherapy, and
radiotherapy with chemotherapy. Much of the information
regarding individual therapies comes in the context of inconsistent
staging information, palliative versus curative goals, and variable
treatment fields (whole abdomen vs. pelvic). In addition, although
this disease is sensitive to the effects of radiation, this
modality may not prevent tumor recurrence. Generalizations regarding the
role of radiotherapy can be made, but specific recommendations as to
the modern treatment of fallopian tube carcinoma are difficult given
the lack of information. As the natural history of fallopian tube carcinoma becomes clearer, it
is reasonable to assume that radiotherapy will fail in all stages, except
in cases in which the disease is completely resected or limited. Among
this group of patients, intraperitoneal radiocolloids and pelvic
radiation therapy have been popular, albeit with mixed response results. After administering adjuvant intraperitoneal 32P with or without pelvic
radiotherapy, Phelps and Chapman98 reported eight long-term survivors out of nine stage I/II patients. Likewise, Schray
and colleagues,58 using adjuvant intraperitoneal 32P alone, reported long-term survival
in two patients with stage I/II disease. Other trials have
not consistently reflected these earlier encouraging results. For example, in
a report from the Mayo Clinic, Podratz and colleagues16 found recurrence in four of six patients with stage IA, IB, and IIA disease
after pelvic radiation and in five of five patients with stage IC, IIB, and
III disease after whole-abdominal radiation. Further, in
a review of 115 fallopian tube cancer patients, 39 of whom had stage
I disease, no survival benefit could be established with the use
of adjuvant radiation over surgery alone.17 This effect held true for stage II patients as well, although there was
a clear treatment bias among this high-risk group. Likewise, in
the review from the M.D. Anderson Cancer Center, no benefit could be
demonstrated in the use of adjuvant radiotherapy over surgery alone
in 20 stage I and stage II patients.15 Morbidity from therapy was significant: of 43 patients, seven required
hospitalization, three underwent intestinal resection, and one died of
intestinal perforation. Despite these observations, the high rate of
recurrence in this group of patients calls for some form of adjuvant
therapy. These authors agree that patients with intra-abdominal
risk or gross intra-abdominal disease should, in general, be treated
with systemic chemotherapy. Only selected patients with microscopic
extrapelvic disease should be considered for adjuvant therapy with
whole-abdominal radiation. Chemotherapy Much of the recent advancements in the treatment of fallopian tube carcinoma
has come from the evaluation of adjuvant single and multi-agent
platinum-based chemotherapy. Although chemotherapy has been
implemented in this disease since its advent, little success was achieved
in early trials. Many of these regimens consisted of single-agent
alkylating or anthracycline-based combinations and were
administered for recurrent or rapidly progressing disease, often after
adjuvant radiation therapy. Table 6 depicts trials of noncisplatin-based treatment regimens in the
adjuvant setting for advanced disease. Although a few partial responses
were seen, long-term survivals were rare, ranging from 0% to 29%. The
most extensive experience among the single-agent
adjuvant trials were the alkylators, such as melphalan, cyclophosphamide, chlorambucil, and thiotepa. Combination regimens reported
often added doxorubicin to cyclophosphamide. In one series, the benefit
of a multi-agent nonplatinum-based regimen over single-agent
therapy was clear, demonstrating a three-fold increase
in 5-year survival, from 9% to 29%.94 Table 6. Summary of Series Reporting Responses to Nonplatinum-Based
Chemotherapy in Stage II to Stage IV Fallopian Tube Carcinoma
| Author |
5-Year No. Patients |
Survival (%) |
| Denham and MacLennan14 |
39 |
18 |
| Eddy et al15 |
32 |
5 |
| Muntz et al67 |
1 |
0 |
| Peters et al94 |
7* 23 |
9*29 |
| Pfeiffer et al10 |
17 |
6 |
| Podratz et al16 |
18 |
19 |
| Roberts et al91 |
31 |
6 |
| Total |
168 |
13.2 |
*Single-agent protocol versus a multiagent noncisplatin-based
protocol
With the advent of cisplatin and the promising results seen in early trials of patients with epithelial
ovarian cancer, renewed interest developed in treating patients with
fallopian tube carcinoma. The first documented complete responses
with this agent were credited to Deppe and colleagues,93 who documented a complete response in two of four patients with advanced, measurable
disease. Since this report, several retrospective series
have been published studying cisplatin-containing regimens in
the adjuvant setting, with response rates ranging from 21% to 91% and 5-year survival ranging from 14% to 51% (Table 7). This is comparable with responses seen in similarly staged patients
with ovarian carcinoma. There has been only one prospective trial
reported, which took 9 years to accumulate 18 patients.87 Information supporting the relationship of specific responses to cisplatin-based
chemotherapy with residual tumor volume is lacking, but
such a relationship was suggested by Barakat and associates.61 In their review, 5-year survival among 14 stage II to stage IV, cisplatin-treated
patients with no measurable disease was superior
to that of patients similarly staged and treated, but with measurable
residual disease (83% vs. 29%). Most reported
regimens incorporating cisplatin commonly add an alkylator, such as cyclophosphamide alone or in combination with an anthracycline. Data supporting the use
of adjuvant chemotherapy in low-risk patients (i.e., those with stage IA or stage IB disease) are lacking and insufficient
for recommendations. Criteria for treatment in this subgroup will
likely follow that of ovarian carcinoma, although it is important to
recognize the lack of association of grade and the importance of muscularis
penetration in making decisions for adjuvant therapy. Table 7. Summary of Series Reporting Responses to Platinum-Based
Chemotherapy in Stage II to Stage IV Fallopian Tube Carcinoma
| Author |
No. Patients |
Overall Response (%) |
5-Year Survival (%) |
| Barakat et al61 |
31 |
60 |
51 |
| Gurney et al89 |
10 |
80 |
18 |
| Maxson et al59 |
12 |
92 |
27 |
| Morris et al87 |
18 |
53 |
46 |
| Muntz et al67 |
12 |
71 |
50 |
| Pectasides et al97 |
11 |
91 |
48 |
| Peters et al94 |
16 |
81 |
15 |
| Rose et al30 |
14 |
21 |
14 |
| Total |
124 |
68.5 |
36.1 |
More recently, with the introduction of carboplatin and its gradual replacement of cisplatin in ovarian cancer treatment, interest in carboplatin in fallopian tube carcinoma has arisen. Many ovarian cancer trials, of
all phases, studying carboplatin-containing regimens also include
fallopian tube carcinoma. They show excellent response rates (81%) but
most often there is no subgroup analysis of fallopian
tube carcinoma available.99,100 Unfortunately, there is a high incidence of hypersensitivity to carboplatin (5% to 67%), which increases with the number of
cycles. As platinum-containing regimens seem to be the most active
in this condition there is considerable interest in retreating patients
with a platinum agent after carboplatin hypersensitivity. Multiple studies have demonstrated the feasibility and
safety of readministeration in this setting.101,102 Future trials will certainly incorporate the new taxanes, such as paclitaxel and docetaxel, and newer topoisomerase I inhibitors, such as topotecan
and camptothecin, because these agents have recently demonstrated promising
data among patients with advanced ovarian carcinoma.104,105 A review of 23 patients who received primary paclitaxel-containing
regimens, the majority also received a platinum agent, revealed overall
median progression-free survival of 27 months.103 A phase I trial of paclitaxel, melphalan, and cisplatin in patients with advanced fallopian tube cancer has been reported and
is entering phase II study.106 Hormonal Therapy Use of hormonal therapy in both the adjuvant and salvage setting has been
reported in many series, although not independently.14,15,16,23,30,107 The rationale is supported by information relating the cyclic influence
of hormones on tubal epithelium. The routine use of these agents cannot
be advocated currently, however, because of the lack of association
between estrogen and progesterone receptor status and prognosis and the low responses observed clinically
with the use of megestrol acetate or medroxyprogesterone acetate.85 |