Hydatidiform Mole The primary management of women with hydatidiform mole encompasses surgical
evacuation coupled with close monitoring of subsequent hCG levels. Although
the complete and partial hydatidiform moles have distinct cytogenetic, histopathologic, and clinical features, their acute management
is very similar and both should be considered clinically in the same
category. However, there are several differences in the clinical behavior
of these two types of molar pregnancies.24,29 Table 1 is a summary of the cytogenetic, histopathologic, and clinical characteristics
of partial and complete hydatidiform moles. The differences in clinical characteristics of partial and complete hydatidiform
mole can be explained in part on the basis of the differing
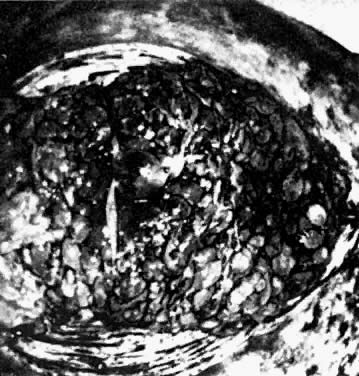
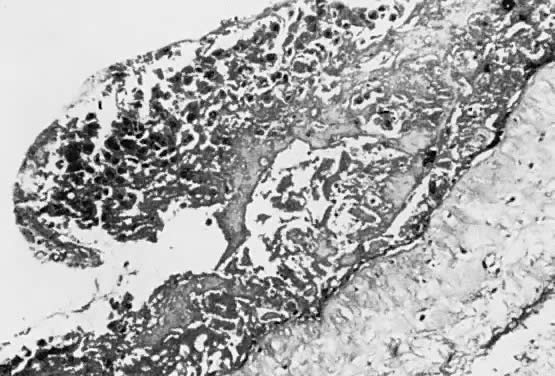
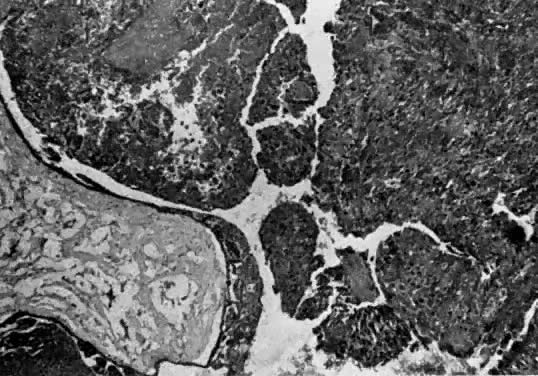
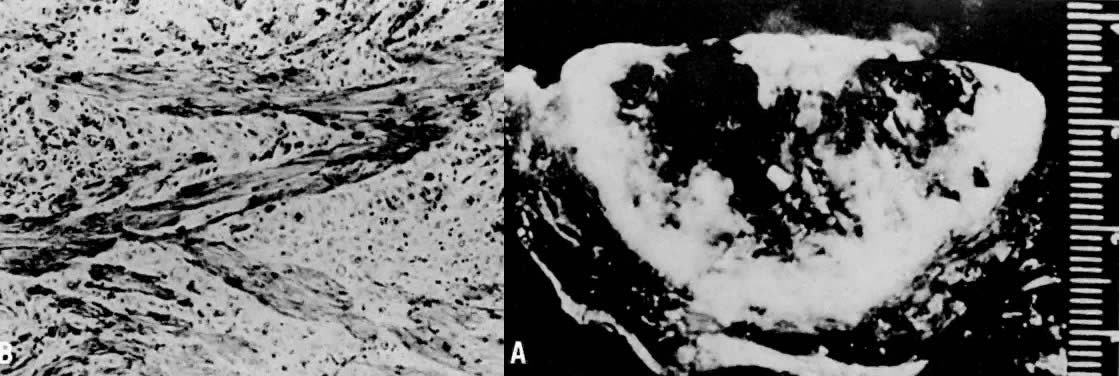
amounts of trophoblastic proliferation in these syndromes.24 Partial hydatidiform moles have focal, irregular hydropic changes of chorionic
villi coupled with focal trophoblastic proliferation and frequently
have an identifiable fetus up to or beyond 8 weeks' gestation. Because
of the only modest increase in placental size and trophoblast
mass, the uterus is usually enlarged to a lesser degree than that of the
anticipated duration of gestation or is compatible with dates. As noted
previously, partial hydatidiform moles are probably underdiagnosed
and may comprise up to 1% to 2% of all clinically recognized spontaneous
abortions. A patient with partial hydatidiform mole usually presents
with clinical and ultrasound features of a missed or threatened spontaneous
abortion. The majority have low pre-evacuation hCG levels and
lack theca lutein cysts. Nonmetastatic postmolar GTT is diagnosed in
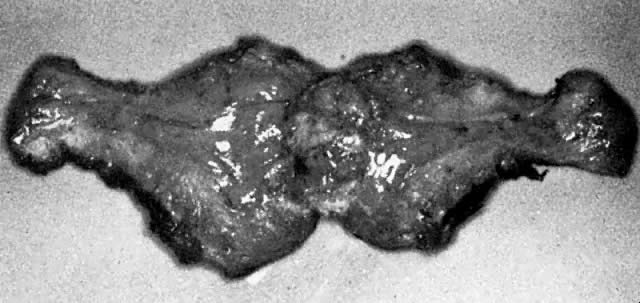
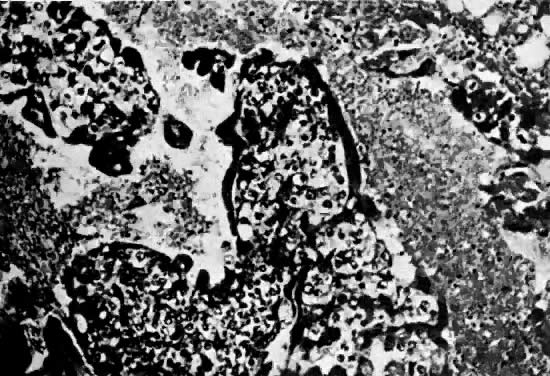
less than 5% to 10% of patients after evacuation of partial moles.29,74 In contrast, complete hydatidiform moles have diffuse, often massive, hydropic
degeneration of chorionic villi with diffuse trophoblastic proliferation
that results in a differing spectrum of clinical signs and
symptoms.24 Vaginal bleeding is the most common presenting symptom in patients with
complete moles, often producing anemia.75 Up to half of all patients with complete hydatidiform mole will have uterine
enlargement beyond the expected gestational age caused by expansion
of the uterus by both molar tissue and intrauterine bleeding.75,76 Unilateral or bilateral ovarian enlargement produced by theca lutein cysts
is clinically detected in one fourth to one third of patients with
complete hydatidiform mole and is usually associated with hCG levels
above 100,000 mIU/ml (Fig. 12).75,76,77,78 Preeclampsia and hyperemesis each occur in approximately one fourth of
patients with complete mole. The majority of patients with these symptoms
also usually have markedly elevated hCG values.75 The development of pregnancy-induced hypertension before 24 weeks' gestation
is almost diagnostic of molar pregnancy. Increases in thyroid hormones
are frequently diagnosed in patients with complete hydatidiform
moles, but clinical hyperthyroidism is detected in less than 10%.79 There is no consistent relationship between serum hCG values and results
of thyroid function tests. Finally, in contrast to partial moles, patients
with complete moles have approximately a 20% incidence of trophoblastic
tumor after evacuation, with 10% to 20% of these having metastatic
disease.76,77,80,81,82,83,84,85,86,87 The majority of those with trophoblastic tumors have invasive or persistent
mole while approximately one fourth to one third have gestational
choriocarcinoma.  Fig. 12. Serum hCG secretion in normal pregnancy. Note the rapid early increase (doubling
every 48 hours through day 70), peak levels of approximately 200,000 mIU/ml
at 8 to 9 weeks, and then declining values to a lower
plateau for the remainder of gestation. The wide ranges of variation should
be recognized.(Modified from Hon EH: A Manual of Pregnancy Testing, Boston, Little, Brown & Co, 1961) Fig. 12. Serum hCG secretion in normal pregnancy. Note the rapid early increase (doubling
every 48 hours through day 70), peak levels of approximately 200,000 mIU/ml
at 8 to 9 weeks, and then declining values to a lower
plateau for the remainder of gestation. The wide ranges of variation should
be recognized.(Modified from Hon EH: A Manual of Pregnancy Testing, Boston, Little, Brown & Co, 1961)
|
The diagnosis of hydatidiform mole is no problem after the patient passes
molar vesicles. Even then, however, ultrasound should be used to exclude
the presence of a fetus (as in partial mole or twin gestation), as
well as to further define the presence and size of theca lutein cysts
of the ovaries (Fig. 13). A variety of other physical and chemical tests have been used over the
years, including amniography, arteriography, computed tomography (CT), and
magnetic resonance imaging (MRI), but few are indicated beyond
standard pelvic ultrasound. Tests for hCG may occasionally be useful
in the differentiation of hydatidiform mole from normal pregnancy. Serum
assays may be used, and the results should be compared with the hCG
levels of normal pregnancy at the gestational age in question. Although
a single result well above normal range for that state of pregnancy suggests molar pregnancy, only the results of serial assays are definitive. Delfs80 has asserted that between days 60 and 100 of pregnancy there is no level
of hCG secretions, however high, that could not be caused by a normal
pregnancy or some variation thereof. Thus, gonadotropin levels in excess
of 100,000 IU to 200,000 IU/24-hr urine collection or their equivalent
serum levels are compatible with molar pregnancy, with the exception
of the peak elevations seen between weeks 9 and 14 of normal pregnancy. Higher
levels may also be associated with multiple gestation or
toxemia of pregnancy. A continued rise in hCG levels after the 14th
week of pregnancy (the hCG level drops at this time in normal pregnancy) is
the best evidence of a molar pregnancy that can be obtained by hCG
assay (Fig. 14). 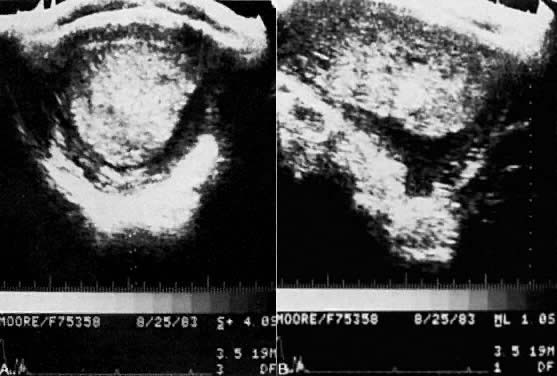 Fig. 13. Pelvic ultrasound of hydatidiform mole in situ. A. Transverse view of the uterus showing mole in situ. B. Longitudinal section of the molar pregnancy.(Courtesy of Dr. James Bowie) Fig. 13. Pelvic ultrasound of hydatidiform mole in situ. A. Transverse view of the uterus showing mole in situ. B. Longitudinal section of the molar pregnancy.(Courtesy of Dr. James Bowie)
|
 Fig. 14. Mean value and 95% confidence limits describing normal postmolar β-hCG
regression curve.(Schlaerth JB, Morrow CP, Kletzky OA et al: Obstet Gynecol 58:478, 1981. Reprinted
with permission from The American College of Obstetricians
and Gynecologists.) Fig. 14. Mean value and 95% confidence limits describing normal postmolar β-hCG
regression curve.(Schlaerth JB, Morrow CP, Kletzky OA et al: Obstet Gynecol 58:478, 1981. Reprinted
with permission from The American College of Obstetricians
and Gynecologists.)
|
A variety of other laboratory studies have been investigated in the diagnosis
of molar pregnancy. These include determination of serum leucine
aminopeptidase level, human placental lactogen, estrogens, and various
quantities and ratios of subunits of hCG. The concentrations of all
of these vary in normal pregnancy, and, as a rule, are not of significant
assistance in the differential diagnosis of normal pregnancy and
molar pregnancy, since the values found in well-differentiated hydatidiform
moles tend to overlap with those of normal pregnancy. In summary, the pertinent diagnostic features in hydatidiform mole are
as follows: - Enlargement of the uterus disproportionate to duration of gestation
- Irregular vaginal bleeding to a modest degree, on occasion profuse, beginning
after the second month of pregnancy
- Absence of fetal parts on palpation or roentgenogram in a uterus of such
a size that one would expect such findings
- Absence of fetal heart tones at a time when, by gestational duration or
size, they would be expected to be audible
- Characteristic ultrasonographic patterns
- Symptoms of preeclampsia in the late first or early second trimester
- Cystic enlargement of the ovaries
- High levels of hCG
- Positive findings on ultrasonography (perhaps the best diagnostic feature (see Fig. 13).
Despite the differences between partial and complete hydatidiform moles, the
initial management and subsequent surveillance of patients with
partial or complete molar gestations are similar. After the diagnosis
has been confirmed, the evaluation of a patient with a molar gestation
is directed toward screening for metastatic disease and stabilization
of the patient for evacuation. Preoperative evaluation consists of a
complete physical examination, baseline serum hCG level, chest roentgenogram, hematologic
profile, renal and liver function tests, and thyroid
function tests. If the uterus is enlarged more than 14 to 16 weeks' gestational
size or the patient has pregnancy-induced hypertension, arterial
blood gases should be measured preoperatively because many of
these patients will develop respiratory insufficiency after evacuation. EVACUATION. Techniques for evacuation of hydatidiform mole have included induction
of a labor with oxytocin or prostaglandins, hysterotomy, cervical dilation
with suction curettage (D&C), and hysterectomy. If the patient
desires sterilization, hysterectomy with the mole in situ is our preferred
method of evacuation. However, the majority of women with hydatidiform
moles can be safely evacuated using suction D&C regardless
of uterine size.75 Suction Curettage. The patient should be hemodynamically stable with correction of preoperative
anemia, stabilization of blood pressure if superimposed pregnancy-induced
hypertension is present, and stabilization of systemic manifestations
of hyperthyroidism with β-blockers. If the uterus is more
than 14 to 16 weeks' gestational size, a central line should be placed
for intraoperative central venous pressure monitoring and rapid administration
of fluid or blood products during the procedure. At least 2 units
of blood and a laparotomy set should be available in the operating
room. After induction of anesthesia, the cervix is dilated gently with Pratt
dilators to allow passage of a suction cannula appropriate for the volume
of molar tissue. An oxytocin infusion is begun after introduction of the suction cannula and initiation of the curettage. A 12- to 14-mm
cannula is introduced into the lower to mid endometrial
cavity. Because the myometrium is often distended and soft, no effort
is made to sound the uterus to the fundus in order to avoid uterine perforation. During
suction curettage, the fundus is massaged to assist
in stimulating uterine contractions and reduce the risk of perforation. The
majority of the molar tissue can be removed by rotating the cannula
to evacuate uterine contents. As the uterine fundus involutes, completion
of evacuation is performed using gentle curettement with the suction
cannula. When the suction evacuation is believed to be complete
and the uterus is well contracted, the endometrium is gently curetted
using a large sharp curette to ensure complete evacuation. The curettings
from suction and sharp curettage should be submitted separately for
pathologic review. Oxytocin infusion is continued for 24 hours after
molar evacuation or until vaginal bleeding is minimal. Hysterectomy. Hysterectomy offers the advantage of simultaneous evacuation of hydatidiform
mole and sterilization for women who no longer wish to bear a child.77,88 Additionally, performance of a hysterectomy decreases the risk of malignant
sequelae to approximately 3.5% from the 20% anticipated after evacuation
with D&C.77However, hysterectomy does not eliminate the potential for malignant sequelae, and
these women must have their hCG levels monitored after hysterectomy. We generally perform a simple total abdominal hysterectomy with the mole
in situ. Because most women with hydatidiform mole are younger than 40 years
of age, the adnexa should not be removed unless the patient
is perimenopausal or there is obvious adnexal metastasis. Theca lutein
cysts usually regress spontaneously after evacuation or hysterectomy
and do not need to be drained or removed unless torsion or intraoperative
rupture with hemorrhage occurs.78 Other Techniques. Induction of labor with oxytocin or prostaglandins carries the potential
increased risk for disseminating trophoblast throughout the systemic
circulation caused by uterine contractions against an undilated cervix. Significant
blood loss and incomplete evacuation often occur, requiring
suction D&C.89 Hysterotomy is also associated with an increased blood loss when compared
with suction D&C. The vertical uterine incision frequently results
in the requirement for cesarean section in subsequent pregnancies. Because
the majority of these patients are in the prime of their reproductive
age group, this is an important consideration. Furthermore, Curry
and co-workers77 and Tow90 reported that hysterectomy for evacuation of hydatidiform mole resulted
in a higher incidence of postmolar malignant sequelae than did suction
D&C. THECA LUTEIN CYSTS. Clinically evident (greater than 5 to 6 cm) theca lutein cysts of the
ovary are detected in approximately one fourth to one third of women with
hydatidiform mole, with additional smaller cysts often detected by
ultrasound alone.76,77,78 Ovarian enlargement correlates with marked elevation of serum hCG levels
greater than 100,000 mIU/ml. Histologically and physiologically these
cysts are similar to iatrogenic ovarian hyperstimulation produced by
exogenous gonadotropin/hCG administration for induction of ovulation. Although
theca lutein cysts are usually detected before molar evacuation, they
often develop within the first week after evacuation.76,78 The mean time for disappearance of theca lutein cysts is approximately 8 weeks. It
is very rare for a patient to develop overt ovarian hyperstimulation
with fluid retention and/or ascites, but an occasional patient
will develop ovarian torsion or rupture and bleeding from the cyst, requiring
oophorectomy.78 Theca lutein cysts are associated with an increased incidence of postmolar
trophoblastic tumor; in particular, Montz and colleagues reported
a 75% incidence of postmolar sequelae among women with bilateral theca
lutein cysts.78 Although theca lutein cysts usually regress spontaneously with falling
hCG levels after molar evacuation, approximately 30% will develop secondary
enlargement in response to rising hCG levels associated with postmolar
sequelae.78 Occasionally, these cysts will persist for several months after hCG level
remission has been achieved. RESPIRATORY DISTRESS SYNDROME. During evacuation of hydatidiform moles there are many potential causes
for respiratory distress, including trophoblastic deportation, high-output
congestive heart failure caused by anemia or hyperthyroidism, preeclampsia, and
iatrogenic fluid overload.91 Pulmonary complications are observed in approximately one fourth of patients
with uterine size more than 16 weeks' gestation. Although the syndrome
of trophoblastic embolization has been emphasized in the past
as an underlying cause for respiratory distress syndrome,92,93 Hankins and associates detected only scanty amounts of trophoblastic cells
in the pulmonary artery blood among a small series of women undergoing
evacuation of large molar pregnancies.94 Furthermore, Cotton and co-workers documented a transient impairment of
left ventricular function during general anesthesia in a small series
of patients studied with invasive central monitoring performed during
suction D&C for molar evacuation.95 This might contribute to the development of pulmonary edema in unmonitored
patients given large volumes of crystalloid during the procedure. In
general, pulmonary complications should be managed with appropriate
ventilator support and central monitoring with a Swan-Ganz catheter
to accurately determine fluid status and the need for fluids, blood products, or
diuresis. All patients should have a chest roentgenogram after
evacuation of hydatidiform mole to rule out significant trophoblastic
deportation, pulmonary metastasis, or development of pulmonary edema. UTERINE PERFORATION. Uterine perforation should rarely occur as an acute complication during
primary suction D&C for hydatidiform mole. If perforation is recognized, the
suction should be immediately discontinued, the cannula removed, and
the rate of oxytocin infusion increased. Laparoscopy or laparotomy
should be performed to access the site of perforation. If hemostasis
is adequate and there is no damage to gastrointestinal organs, curettage
can be completed under laparoscopic visualization. Rarely, uterine perforation occurs during or after suction D&C through
a focus of deep myometrial penetration by invasive mole. Surgical
management should be individualized based on the site and extent of perforation. Although
some patients will require hysterectomy, small series
have suggested that individual patients with invasive moles can be
treated with segmental resection and repair of the affected myometrium.96,97 Most frequently, these will occur in the midline of the uterine fundus. MANAGEMENT OF COEXISTENT FETUS. Rare cases of twin pregnancies consisting of normal conceptus and complete
hydatidiform mole have been reported.98,99,100 It is important that all cases suggesting these entities be carefully
studied both cytogenetically and histopathologically to avoid confusion
with a partial hydatidiform mole. In rare cases, a fetus has been carried
to viability.100 We have been involved in the care of several women in whom the differential
diagnosis has included partial hydatidiform mole versus twin gestation
with coexistent mole and normal pregnancy. In these circumstances, we
recommend a thorough obstetric ultrasound to rule out fetal malformations
and to fully characterize the placenta. On several occasions
the presumed mole has subsequently been confirmed to be either a nonviable
twin, retroplacental hematoma, or other nonmolar placental abnormality. In
patients whose pregnancies appear to consist of a viable fetus
with molar changes in a portion of the placenta, we have attempted
to use either chorionic villous sampling in an effort to prove or disprove
the existence of a triploidy or amniocentesis later in gestation
to assess the fetal karyotype. However, the majority of these cases can
be resolved through a careful ultrasonographic study of the placenta
and histopathologic examination of the products of conception after
delivery or spontaneous abortion. Although the persistence of a marked
elevation (more than 100,000 mIU/ml) in the level of serum hCG is consistent
with the diagnosis of hydatidiform mole, we have observed several
anecdotal cases in which this diagnosis was entertained during the
second trimester of pregnancy and subsequently disproved at delivery. Therefore, we
do not encourage overmanagement of these unusual pregnancies
because the majority of patients in whom this diagnosis is entertained
will not have the diagnosis of twin viable conceptus-molar gestation
confirmed. RISK FACTORS FOR POSTMOLAR GESTATIONAL TROPHOBLASTIC TUMOR. Several clinicopathologic factors have been associated with an increased
risk for the development of postmolar GTT. Many investigators have
reported that increasing maternal age is associated with an increased
risk of trophoblastic tumor.72,76,77 This risk appears to increase as the patient enters the perimenopausal
age range. In contrast, teenagers do not appear to have a consistently
increased risk for the development of postmolar GTT. Likewise, gestational
age at diagnosis of molar pregnancy has been found to have conflicting
associations with the development of postmolar GTT.76,77 Hertig and Sheldon reported that the amount and characteristics of trophoblastic
proliferation observed histologically in the primary mole roughly
correlated with the subsequent development of postmolar GTT.27 However, others have been unable to document an increased risk for patients
with increasing amounts of trophoblastic proliferation.77 Unfortunately, the identification of marked amounts of trophoblastic proliferation
or anaplasia may be, in part, dependent on the number of
histologic sections obtained from the primary mole. Other clinical factors
related to an increased amount of trophoblastic proliferation have
been documented to affect outcome after molar evacuation. Curry and co-workers77 and Morrow and associates76 reported similar adverse effects for uterine enlargement and the presence
of theca lutein cysts. The presence of uterine enlargement beyond
that appropriate for dates was associated with an increased risk of postmolar
GTT to between 25% and 48%, respectively, while the presence of
clinically detected theca lutein cysts increased the risk to approximately 50%.76,77 The combination of these factors identified populations with a risk of
approximately 60% for developing postmolar GTT. Other investigators have
also reported adverse effects of uterine enlargement and theca lutein
cysts. In particular, Montz and associates reported a markedly increased
risk for women with bilateral theca lutein cysts.78 Other clinical risk factors for postmolar GTT have been reported, including
the development of pulmonary complications during molar evacuation
and uterine subinvolution with hemorrhage following evacuation. Although
these clinical features are observed in a minority of patients, they
do identify high-risk subsets of patients. In particular, Morrow and
associates reported that postmolar GTT was subsequently diagnosed in
all six women with postevacuation hemorrhage in their series.78 Although individual clinical factors can be used to identify women at an
increased risk for the development of postmolar GTT, they lack the ability
to predict the course of disease for individual patients. Some
investigators have used clinicopathologic factors to identify high-risk
patients who might benefit from prophylactic chemotherapy. However, even
using multivariate analysis, Parazzini and co-workers were able to
retrospectively assign only 69% of their patients to high- and low-risk
groups.101 The low-risk group had a 4% and the high-risk group had a 32% incidence
of postmolar GTT. Unfortunately, the high-risk group accounted for only 6 (15%) of 39 patients
who developed postmolar GTT in this study.101 This study underlines the necessity for following each individual patient
with serial hCG monitoring, rather than depending on clinical risk
factors to assign therapy. Newer laboratory methods may improve the ability to predict the development
of postmolar GTT. Assays that measure free β-subunits in the
presence of intact hCG have been developed. Khaezaeli and co-workers
reported preliminary evidence to suggest that elevations in the free β-subunit
fraction are observed more frequently at the time of evacuation
in patients with hydatidiform moles destined to develop postmolar
GTT.97 The use of the free β-subunit assays is being prospectively evaluated
in an ongoing Gynecologic Oncology Group study.102 Furthermore, the identification of aneuploidy in the primary mole using
flow cytometry appears to identify patients at higher risk for postmolar
GTT.103,104 PROPHYLACTIC CHEMOTHERAPY. The role of prophylactic chemotherapy, given at or prior to the time of
molar evacuation to prevent postmolar GTT remains controversial. The
rationale for the use of a limited course of methotrexate or dactinomycin
is clear: systemic levels of chemotherapy would theoretically prevent
the establishment of locally invasive disease or metastasis that
might occur as a result of embolization of trophoblast at the time of
D&C and would perhaps increase the rate of regression of molar tissue
in patients with a large volume of disease. Several investigators, however, have
expressed concerns regarding the use of prophylactic chemotherapy
around the time of molar evacuation when anecdotal reports
of deaths caused by prophylactic chemotherapy were reported in the 1970s. 77 Furthermore, large series reported in the early 1970s from Singapore reported
that although the use of prophylactic methotrexate resulted in
a nonsignificant decrease in the incidence of choriocarcinoma following
evacuation of hydatidiform mole there was a paradoxically significant
increase in the mortality rate with one death from drug toxicity and
two from choriocarcinoma among the treated patients.105 Therefore, many investigators have believed that routine application of
prophylactic chemotherapy is not warranted in the management of most
patients with hydatidiform moles. On the other hand, several recent comparative series have reported a significantly
decreased risk of postmolar GTT among patients treated with
prophylactic chemotherapy.75,106,107 Specifically, Kim and associates conducted a prospective randomized trial
using prophylactic methotrexate with folinic acid at the time of molar
evacuation.106 In this series the use of prophylactic chemotherapy reduced the incidence
of postmolar GTT from 47% to 14% in patients with high-risk moles
but did not significantly decrease the low incidence of postmolar GTT
in those with low-risk moles.106 In contrast to other studies using conventional courses of methotrexate
and dactinomycin, the methotrexate/folinic acid regimen appears to have
quite limited toxicity, making it safer for a prophylactic regimen. However, because
methotrexate is the most frequently used agent for
first-line therapy in patients with postmolar GTT, we believe it may be
important to use a different cytotoxic agent for chemoprophylaxis to
prevent the development of drug resistance in patients who fail chemoprophylaxis. Further randomized studies are needed to define the ideal regimens and
patient populations that would benefit from chemotherapeutic prophylaxis
after evacuation of hydatidiform mole. From the available data, patients
with high-risk hydatidiform moles would appear to benefit from prophylactic
chemotherapy, but the risk of postmolar GTT is not eliminated; therefore, these
patients still require surveillance with serial
hCG testing. At present, we cannot recommend the indiscriminate use of
prophylactic chemotherapy after evacuation of hydatidiform mole because
of the nearly universal availability of sensitive hCG assays for monitoring
patients at least in this country. SURVEILLANCE AFTER MOLAR EVACUATION. Surveillance using serial, highly sensitive and accurate quantitative
serum hCG levels is the only reliable means for the early detection of
malignant sequelae after evacuation of hydatidiform mole. One of any
number of sensitive assays employing polyclonal or monoclonal antibodies
to either whole-molecule or total (free and bound) β-hCG fragments
can be used. A baseline level should be obtained within 48 hours
of evacuation and serial levels followed at 1-week intervals until normal
hCG levels are obtained (Fig. 14).75,76,77,81,82,83,84,85,86,87 Levels should then be followed at 1- to 2-month intervals to ensure that
spontaneous remission is sustained beyond 6 to 12 months. Although
some have recommended that patients with partial hydatidiform moles can
stop surveillance after hCG level remission has been achieved, the approximately 5% to 10% incidence of trophoblastic tumor after evacuation
of partial moles74 reported by the New England Trophoblastic Disease Center is of concern; we
generally recommend at least 3 to 6 months of normal hCG levels in
these patients before surveillance is discontinued. It is rare to observe
reelevation of hCG levels caused by postmolar GTT after more than 6 months
of normal hCG levels without an intercurrent pregnancy. Virtually
all cases of postmolar GTT reported in adequately monitored patients
have occurred within the first 6 months after molar evacuation75,76,77,80,81,82,83,84,85,86,87; therefore, we believe that a minimum of 6 months of hCG remission should
be recommended for patients after an evacuation of a complete hydatidiform
mole. Pelvic examinations should be repeated every 2 weeks and chest roentgenograms
every month until the hCG level has declined to less than 1000 mIU/ml. Patients
who have not undergone hysterectomy should use contraception
during the interval of hCG level monitoring until sustained remission
has been documented. This avoids confusion caused by an elevated
hCG level associated with an intercurrent pregnancy. Although studies
from the United Kingdom suggested an increased risk for postmolar GTT
in women who used oral contraceptives,108 several studies from the United States and Canada,109,110,111 including a randomized Gynecologic Oncology Group study,112 have failed to demonstrate any increased risk for postmolar GTT in women
using moderate- to low-dose oral contraceptives. The differing results
may reflect different criteria used to diagnose postmolar GTT or, alternatively, may
reflect use of different formulations of oral contraceptives
in the studies cited. We routinely recommend the use of oral
contraceptives with a low estrogen content unless there are specific
contraindications to their use, because they are the most effective means
of reversible contraception. DIAGNOSIS OF POSTMOLAR GESTATIONAL TROPHOBLASTIC TUMORS. Approximately 20% of patients undergoing evacuation of a complete hydatidiform
mole will develop postmolar GTT,80,81,82,83,84,85,86,87 70% to 90% of these consist of histologically defined persistent or invasive
moles, while 10% to 30% are choriocarcinomas. Because the historical
mortality for patients with invasive moles ranged around 20%,113 most investigators in the United States have used conservative criteria
for initiating chemotherapy in patients after evacuation of hydatidiform
mole in an attempt to reduce the morbidity caused by local proliferation, infection, and
hemorrhage and to prevent mortality from local
disease or systemic metastasis. The vast majority of patients are therefore
treated on the basis of hCG level regression patterns without a
firm histologic diagnosis. Before the development of effective chemotherapy, Delfs noted that approximately 9% of
patients with molar pregnancies developed proliferative
sequelae and required hysterectomy.80 Series reported since the introduction of chemotherapy have had a wide
variation in the frequency of postmolar GTT (see Table 1), with 6% to 25% of the patients who developed postmolar GTT having metastatic
disease.76,77,80,81,82,83,84,85,86,87 These observed differences in the frequency of postmolar GTT likely reflect
inclusion of partial moles in some series, a different incidence
of metastatic disease in patient populations, or, most significantly, different
hCG level regression criteria used to define postmolar GTT
and assign therapy in the various studies. Before the development of sensitive hCG assays, clinical risk factors alone
were often used to follow patients after evacuation of hydatidiform
moles. Histologic assessment of trophoblastic proliferation can yield
high- and low-risk groups of molar gestations27 but are of little use in determining the need for therapy in the individual
patients.77 Excessive uterine enlargement, theca lutein cysts, development of respiratory
distress syndrome after uterine evacuation, and postevacuation
uterine bleeding are also associated with a higher frequency of postmolar
GTT.75 In contrast, prompt uterine involution and regression of theca lutein
cysts are favorable signs. However, monitoring of hCG levels, as discussed
earlier, is the most sensitive and accurate method for predicting
the development of postmolar GTT. Criteria for the diagnosis of malignant postmolar GTT include high levels
of hCG (serum level > 20,000 mIU/ml) more than 4 months after evacuation
of a hydatidiform mole, progressively increasing hCG values, histologic
evidence of choriocarcinoma or placental site trophoblastic
tumor, or evidence of metastatic disease. Most American centers will
administer chemotherapy to patients who exhibit a plateau of serial hCG
values. Additionally, some investigators have recommended instituting
therapy based on persistence of detectable hCG at some arbitrary interval
following molar evacuation. Bagshawe and colleagues have used extremely conservative criteria for instituting
therapy after molar evacuation and treated only approximately 6% of
their 280 patients.83 Treatment was administered to patients with vaginal or pulmonary metastases
only if the hCG levels rose or the patient developed complications
from metastatic disease. Likewise, patients with an hCG level plateau
were observed for several weeks and were not treated unless the hCG
level actually rose.83 These criteria are in sharp contrast to the more frequent recommendations
that all patients with any metastatic disease, or even a plateau of
hCG level persisting for 3 consecutive weeks, be treated. Kohorn has also suggested that patients with plateauing hCG levels might
be safely followed beyond 2 weeks if reliable hCG follow-up is available.86 Nine percent of 131 patients followed after molar evacuation in his series
had hCG plateaus for more than 2 weeks during surveillance and subsequently
resumed a pattern of declining hCG levels. Six of these achieved
spontaneous hCG level regression. Additionally, five patients who
were started on chemotherapy for an hCG level plateau were subsequently
found to have an immediate pretherapy hCG level fall of more than 25% from
their sustained plateau.86 These data suggest that patients with plateauing hCG levels may be safely
monitored with serial hCG values over several weeks and that a significant
percentage of these patients will enter spontaneous remission. Therapy has usually been initiated if hCG levels remained elevated beyond
an arbitrary length of time after molar evacuation in some series. For
example, Morrow and colleagues instituted chemotherapy if hCG was
detectable at 8 weeks after molar evacuation,76 and Hatch and associates treated most patients if levels were elevated 12 weeks
after evacuation.84 Although these reports may review different patient populations, the proportion
of treated patients is somewhat higher in their studies than
in other reports in which therapy was instituted on the basis of hCG
level alone and not based on time from molar evacuation (see Table 2). TABLE 2. International Federation of Gynecology and Obstetrics (FIGO) Staging
for Gestational Trophoblastic Tumors
Stage | Description |
I | Strictly confined to uterine corpus |
II | Extends outside the uterus, but limited to genital structures |
III | Extends to the lungs with or without genital tract involvement |
IV | All other metastatic sites | (Modified from Pettersson F, Kolstad P, Ludwig H et al: Annual Report on
the Results of Treatment in Gynecologic Cancer, vol 19. Stockholm, International
Federation of Gynecology and Obstetrics, 1985)Before the development of effective chemotherapy, Delfs noted that 22% of
her patients had an elevated hCG level more than 60 days after molar
evacuation and, of these, 42% required hysterectomy.80 Other reports have also observed that 36% to 40% of patients with persistent
hCG elevations more than 60 days after molar evacuation required
therapy.72,87 However, no deaths were observed in the study by Lurain and colleagues
even among patients who had therapy instituted more than 60 days after
evacuation.87 These studies indicate that although patients with hCG elevations persisting
after evacuation of hydatidiform mole are at an increased risk
for postmolar GTT, the majority can be safely followed using serial hCG
testing. We recommend that patients with hydatidiform mole have therapy instituted
according to the following criteria: (1) hCG level rise, (2) hCG level
plateau (± 10%) for three or more consecutive weekly measurements (x, x + 7 days, x + 14 days); (3) appearance of metastases; or (4) histologic
evidence of choriocarinoma, placental site trophoblastic
tumor, or invasive mole. Using these criteria, we have continued
to treat approximately 20% of our patients after molar evacuation. PREGNANCY AFTER HYDATIDIFORM MOLE. A majority of women who have been treated for hydatidiform mole are in
their prime reproductive years, and many desire future child bearing. Physicians
from the New England Trophoblastic Disease Center reported
a large series of women whose reproductive outcomes were studied after
evacuation of complete hydatidiform moles.114 The risk for stillbirth, prematurity, spontaneous abortion, and congenital
malformation was similar to that in the general population. Recurrent
molar gestations were observed in 1.3% of their patients.79 Other series have also reported an increased risk for repetitive complete
and partial moles ranging between 1% and 2%.115,116 Furthermore, the risk of a third molar gestation increases to 28% after
a second mole.117 Therefore, after a woman has had a molar pregnancy, she should be reassured
as to the likely normal outcome of future pregnancies but she should
be aware of the increased risk of a repetitive molar gestation. We
recommend obtaining an ultrasound scan early in pregnancy to confirm
normal fetal and placental development, combined with a chest roentgenogram
to screen for occult metastasis from choriocarcinoma masked by the
hCG level rise of pregnancy. The placenta or products of conception
should be examined histologically at the time of delivery or pregnancy
evacuation. Additionally, an hCG level should be obtained 6 to 8 weeks
after delivery of any future pregnancy to exclude the rare occurrence
of choriocarcinoma. Gestational Trophoblastic Tumors The diagnosis of GTT is established when a woman has rising or plateauing
hCG levels or develops metastatic disease after evacuation of a hydatidiform
mole. The diagnosis of invasive mole, placental site tumor, or
choriocarcinoma is a histologic criterion for GTT. Approximately one
half to two thirds of cases of GTT follow molar pregnancies, while gestational
choriocarcinomas derived from term pregnancies, spontaneous
abortions, and tubal pregnancies account for the remainder.35 Often patients who develop GTT after nonmolar gestations may present with
nongynecologic signs and symptoms, including gastrointestinal or urologic
hemorrhage, hemoptysis, or cerebral hemorrhage.118,119 Irregular uterine bleeding or amenorrhea may also be observed. Under these
circumstances, the diagnosis of GTT is facilitated by a high index
of suspicion coupled with hCG level testing and the exclusion of a normal
pregnancy. It should be stressed that the possibility of metastatic
GTT should be considered in any woman of the reproductive age-group
presenting with metastatic disease involving the lungs or distant sites
from an unknown primary site of malignancy. GTT invade into the myometrium and penetrate small uterine vessels. Venous
metastasis then occurs, resulting in retrograde metastasis to the
lower genital tract through the vaginal venous plexus, with direct spread
to the parametrium and distant spread to the lungs. Usually systemic
hematogenous metastases occur only after pulmonary metastases have
become established.120 Small pulmonary metastases might not be detected by conventional chest
roentgenography but can be detected using computed tomography scans of
the lungs in approximately 40% of patients treated for “nonmetastatic” GTT.121 Therefore, we recommend that all women with GTT should have a complete
metastatic survey before initiating treatment, consisting of chest roentgenography
or CT scan of the lungs and CT scan of the brain, abdomen, and
pelvis. An immediate pretreatment hCG value should be obtained
in addition to performance of a complete blood cell count and renal and
liver function tests. We obtain a pelvic ultrasound to exclude the possibility
of intrauterine pregnancy before beginning chemotherapy. The
role of MRI studies for the evaluation of women with GTT is not yet
fully defined, however, small series of patients indicate that these scans
may help localize small foci of intrauterine disease and identify
myometrial invasion.122,123 Arteriography is not routinely used for initial radiographic evaluation
since false-negative and false-positive findings are encountered more
frequently than with CT scans. Angiographic changes can persist in the
uterus of women with GTT long after hCG remission has been achieved.124 Therefore, selective arteriography is reserved only as an optional diagnostic
tool to delineate lesions of unclear etiology detected by other
imaging techniques. Before CT or MRI scans of the brain were available, Bagshawe and Harlan
reported that occult central nervous system (CNS) metastases may be detected
using lumbar puncture with simultaneous serum and cerbrospinal
fluid (CSF) hCG level determinations.125 The plasma-CSF hCG level ratio is normally greater than 60:1 in the absence
of CNS metastases from GTD and is usually less than 60:1 in those
patients with CNS metastases.125 However, some investigators have reported falsely lowered plasma-CSF hCG
ratios among women undergoing first-trimester abortions without trophoblastic
disease and in patients with nonmetastatic GTT.126 Because CT scans of the brain with contrast enhancement have excellent
sensitivity and specificity for metastatic disease and can be used in
conjunction with MRI scans to evaluate questionable lesions detected
on CT scans, we have not routinely obtained CSF hCG levels in the initial
evaluation of patients with GTT. Most frequently, we have used CSF
hCG levels to evaluate patients with resistance to chemotherapy who have
an obscure site of persistent disease. Although operative procedures may be useful in the therapy for women with
GTT, they are rarely indicated for staging or diagnosis alone. Although
histologic evaluation of tissue obtained by D&C may yield prognostic
information relating to response to first-line chemotherapy,127 secondary D&C in patients with rising hCG levels after molar evacuation
will rarely result in spontaneous remission when used without chemotherapy.123 The therapeutic routine efficacy of pretreatment D&C combined with
chemotherapy has never been formally evaluated in a randomized study. Berkowitz
and associates127 evaluated routine pretreatment D&C in 37 patients with nonmetastatic
postmolar GTT. Twenty (54%) had no trophoblastic tissue detected by
pretreatment D&C; 19 of these patients developed sustained remission
with limited chemotherapy. Patients having intrauterine disease with
a worsened histology by Hertig and Sheldon criteria27 were at risk for failure of initial chemotherapy.127 None of the patients in this study suffered uterine perforation or other
complications. However, Schlaerth and associates documented an 8.1% incidence
of uterine perforation during D&C performed in this setting, requiring
hysterectomy in two patients.128 The effect of pretreatment D&C on hCG level regression has never been
established. Furthermore, others have documented that results of postevacuation
curettage rarely affect the management of postmolar GTT.129,130 Therefore, we prefer to reserve secondary D&C for patients who experience
significant uterine bleeding during chemotherapy. Laparoscopy, craniotomy, and thoracotomy are rarely justified to establish
the primary diagnosis of GTT since this diagnosis can be made on the
basis of elevated hCG level coupled with radiographic evidence of metastatic
disease after excluding pregnancy. Consideration of the possibility
of GTT in these settings would render the majority of these diagnostic
surgical procedures unnecessary. Although we have found that the vast majority of patients with high-risk
metastases from GTT almost always have radiographic evidence of pulmonary
metastases,131 we remain reluctant to recommend a less than compulsive radiographic evaluation
before initiation of treatment. Selection of the initial therapy
and subsequent survival is largely dependent on identification of
poor prognostic factors in patients with metastatic disease. It would
be a tragedy to miss the diagnosis of a high-risk metastatic site in
a patient with a negative chest roentgenogram who might otherwise be salvaged
with aggressive therapy. CLASSIFICATION AND STAGING. The International Federation of Gynecology and Obstetrics (FIGO) has developed
a staging system for women with GTT that is based on anatomic
site involvement, conforming to FIGO staging systems used for all other
gynecologic cancers (see Table 2).132 Although this system recognizes the stepwise progression of metastases
in GTT, we believe that it fails to take into account other factors that
are important in determining the prognosis for individual patients
with GTT. Assignment of therapy on the basis of anatomic involvement
alone is not warranted: although essentially all of the patients in stage
I have low-risk disease and all of the patients in stage IV have high-risk
disease, there is considerable overlap in stage II and III, with
a substantial minority of patients in these groups who have significant
risk factors beyond the anatomic site of involvement. This aspect
of GTT has long been recognized, and several prognostic classifications
have been used for grouping patients with GTT. After the development of single-agent methotrexate and actinomycin therapy
and initial reports of successful chemotherapy in patients with GTT, it
was observed that essentially all patients with nonmetastatic disease
could be cured with single-agent chemotherapy but that certain patients
with metastatic disease were at higher risk for failure of treatment
with these agents. In 1965, the National Institutes of Health (NIH) group
identified several factors in patients with GTT that predicted
resistance to single-agent chemotherapy, including high pretreatment
hCG level, prolonged duration of disease, brain or liver metastases, and
previous failed or inadequate therapy.133 In the late 1960s and early 1970s, Hammond and co-workers134 and others135 recognized that patients with these risk factors were more likely to be
cured if they were treated initially with combination rather than single-agent
chemotherapy. A clinical classification system based on these risk factors is most frequently
used in the United States to determine initial treatment and
report results (Table 3).134 Gestational trophoblastic tumors are divided into three categories: nonmetastatic, low-risk/good-prognosis metastatic, and high-risk/poor-prognosis
metastatic. Essentially all patients with nonmetastatic GTT can
be cured using initial single-agent chemotherapy; therefore, they are
not assigned to a prognostic category and are all initially treated
with single-agent chemotherapy. The presence of any single high-risk factor
in a patient with metastatic GTT places her in the high-risk/poor-prognosis
metastatic GTT category. A similar system is used at the Memorial
Sloan-Kettering Cancer Center, which, however, subdivides patients
into low-, moderate-, and high-risk groups based on the criteria
used in the clinical classification system.136 This system recognizes that patients who have high pre-treatment hCG levels
or long duration of disease as the only prognostic risk factors
are at lesser risk of treatment failure than patients with metastases
involving the brain and/or liver or those who have failed prior chemotherapy. TABLE 3. Clinical Classification of Gestational Trophoblastic Tumors
- Nonmetastatic: No evidence of disease outside uterus
- Metastatic
- Good prognosis
- Short duration of symptoms (<4 months)
- Low hCG level (<40,000 mIU/ml serum β-hCG)
- No metastases to brain or liver
- No antecedent term pregnancy
- No prior chemotherapy
- Poor prognosis (any high-risk factor)
- Long duration of symptoms (>4 months)
- High pretreatment hCG level (>40,000 mIU/ml serum β-hCG)
- Brain or liver metastases
- Antecedent term pregnancy
- Prior chemotherapy (unsuccessful)
Compiled from multiple sources134,143,144,168
The main virtue of the clinical classification system is that it allows
prompt identification of patients who would be likely to be successfully
cured using simple forms of chemotherapy and identifies patients who
would be unlikely to be cured using single-agent treatment. In the
past, the majority of patients who were treated with combination chemotherapy
received methotrexate, dactinomycin, and chlorambucil (or cyclophosphamide) combinations, commonly referred to as MAC.134,135,136 With the development of other agents active against GTT and of combinations
that are perhaps more active against GTT than MAC, several investigators
have reported on the failure of the clinical classifications
system to identify patients at risk for failing MAC-type regimens. A more complicated prognostic scoring system has been adopted by the World
Health Organization (WHO, Table 4).137 This system is based on Bagshawe's experience at the Charing Cross
Hospital in London during 1957 to 1973.138 Multiple factors were found to have prognostic significance when analyzed
separately, including patient age, parity, type of antecedent pregnancy, time
interval between antecedent pregnancy and development of GTT, pretreatment
hCG level, paternal and maternal blood type, number and
site of metastases, size of largest tumor, and treatment with prior
chemotherapy. The WHO prognostic index score applies a weighted score
to each factor; each factor is assumed to act independently, and the
sum of individual component scores is used to determine the individual
patient's risk. Patients with a score of 4 or less are considered
low risk, those with a score of 5 to 7 are intermediate risk, and those
with scores 8 or greater are high risk.137 Unfortunately, paternal blood type is not uniformly available for many
patients treated in the United States; therefore, several investigators
have modified this system to omit blood group information.139,140,141 Using modifications of the WHO prognostic index score, several researchers
have reported that the WHO prognostic index score correlates with
survival in patients with high-risk disease by the clinical classification
system who are treated with MAC-based chemotherapy.139,140,141 It is important to consider the individual prognostic factors and their
impact on the survival of patients with GTT. TABLE 4. World Health Organization Prognostic Index Score for Gestational
Trophoblastic Tumors
| Score* |
Prognostic Factors | 0 | 1 | 2 | 4 |
Age (yr) |  35 35
| >39 | | |
Antecedent pregnancy | Hydatidiform mole | Abortion | Term | |
Interval† | <4 | 4–6 | 7–12 | >12 |
hCG (IU/liter) | <103 | 103-104 | 104-105 | >105 |
ABO groups (female × male) | | O × A | B | |
Largest tumor, including uterine tumor | | 3–5 cm | >5 cm | |
Site of metastases | | Spleen, kidney | Gastrointestinal tract, liver | Brain |
Number of metastases identified | | 1–4 | 4–8 | >8 |
Prior chemotherapy | | | Single drug | Two or more |
* The total score for a patient is obtained by adding the individual scores
for each prognostic factor.
Total score 0–4 = low risk, 5–7 = intermediate risk, >8 = high
risk.
† Interval: time (months) between end of antecedent pregnancy and start
of chemotherapy.
(Modified from World Health Organization Scientific Group on Gestational
Trophoblastic Disease. Technical Report Series No. 692. Geneva, World
Health Organization, 1983)Nonmetastatic Disease. The majority of patients in this category have GTT diagnosed after molar
evacuation. This category is probably heavily weighted toward those
patients with proliferative moles or invasive moles rather than true
choriocarcinoma. Virtually all series of patients reported since Hammond
and associates142 described the use of methotrexate and dactinomycin in the treatment of
these patients have essentially 100% sustained remission rates after
primary treatment with single-agent regimens. Therefore, we do not assign
patients with nonmetastatic GTT to prognostic risk groups. hCG Levels. With the exception of placental site trophoblastic tumors, hCG is a sensitive
and specific marker for the monitoring of patients with GTT. Levels
presumably reflect the total body burden of viable tumor. It should
be specified that all of the classification systems use the immediate
pretreatment hCG level to assign treatment, rather than the hCG level
at the time of molar evacuation. Ross and colleagues initially reported
that women with metastatic GTT who had hCG levels more than 100,000 IU/24 hr
urine collection had a remission rate of 41% versus 91% in
those with lower levels.133 This finding has been confirmed in several subsequent studies.135,138 In particular, Bagshawe noted a graduated risk associated with increasing
levels of serum hCG, ranging from 4% when the hCG level was less than 10,000 mIU/ml
to 61% when the level was greater than 1 million mIU/ml.138 However, when analyzing patients with metastatic GTT who had not received
previous treatment, we noted that hCG level alone did not predict
outcome.143 This undoubtedly reflects the fact that almost all patients with high
hCG levels in this report were initially treated with combination chemotherapy
regimens,143 thus negating the prognostic importance of the hCG level alone that was
observed among patients treated with single-agent therapy. Duration of Disease. The duration of GTT, as measured by time from termination of the previous
pregnancy or duration of symptoms until the initiation of treatment, indirectly
reflects the potential for the development of spontaneous
drug resistance and tumor growth. Ross and colleagues first reported
a worse outcome in patients with a duration of disease in excess of 4 months.133 Bagshawe found a progressively increasing fatality rate with time, ranging
from 3% at less than 3 months to 63% at more than 24 months.138 Significantly lower remission rates for patients with lengthy duration
of disease have also been reported by other investigators,135,139,143,144,145 even among previously untreated patients who receive combination chemotherapy
for high-risk factors. Metastatic Site. Detailed studies by Sung and co-workers have documented that the progression
of GTT proceeds initially into the myometrium with pulmonary and
vaginal metastases occurring earlier and brain metastases or other disseminated
metastases occurring later in the progression of disease.120,146 As noted previously, the absence of metastases is a favorable prognostic
factor. Metastatic sites form the basis for the anatomic FIGO staging
system.132 Site of metastatic involvement is an important prognostic factor in determining
survival. Several studies have documented the high-risk nature
of brain, liver, and renal metastases. However, when initial treatment
is individualized, the effect of initial metastatic site of involvement
appears to be lessened.143 Type of Antecedent Pregnancy. The type of antecedent gestation probably has two indirect effects on
outcome. First, patients who are treated for GTT after a nonmolar pregnancy
almost always have choriocarcinoma while those treated after evacuation
of hydatidiform mole may have persistent mole, invasive mole, or, less
commonly, choriocarcinoma. Several series have documented that
a clinicopathologic diagnosis of choriocarcinoma imparts a worse prognosis
for patients with metastatic GTT when compared with a clinicopathologic
diagnosis of invasive mole.135,143 Second, women with GTT after a nonmolar pregnancy often experience a delay
in diagnosis that allows establishment of metastatic disease.143 Bagshawe reported a graded effect of antecedent pregnancy with patients
who had spontaneous abortions and ectopic pregnancies having an intermediate
prognosis between those with GTT following hydatidiform mole
and term pregnancies.138 On the other hand, in our review of patients who presented for primary
treatment of metastatic GTT, patients with an antecedent spontaneous
abortion or ectopic pregnancy had a risk similar to that of patients with
an antecedent term pregnancy.143 A prolonged interval from pregnancy termination to therapy was seen in
the majority of women with nonmolar antecedent pregnancy.143 Other studies have also confirmed that GTT following a term pregnancy
has a worse outcome than GTT following other types of pregnancy, and most
patients often have other high-risk characteristics.147,148 Because of the frequent association of antecedent term pregnancy with
high-risk disease, we include GTT following term pregnancy in the poor
prognostic group. ABO Blood Type. Bagshawe documented a worse outcome among women with blood type B or AB, or
maternal/paternal pairings of type O × A or A × O.138 However, Azab and associates did not confirm a prognostic effect for ABO
blood type in their patient population.149 As mentioned earlier, because reliable information regarding paternal
ABO blood type is lacking for many patients with GTT, several investigators
have modified the WHO scoring system to exclude ABO blood type information. Tumor Size and Number of Metastases. In addition to hCG level, tumor burden should be reflected by the size
of the largest tumor and number of metastatic sites or number of identifiable
metastases. However, in GTT both the primary tumor and metastatic
sites may be composed partially of hemorrhage or necrotic tissue. This
is particularly true for uterine sites of persistent or invasive
moles and metastatic sites of choriocarcinoma. Therefore tumor volume, as
identified on examination or radiographic studies, may not correlate
precisely with actual tumor burden. However, Bagshawe reported that
increasing tumor size had an adverse effect on outcome.138 Several studies have also noted that increasing numbers of identifiable
metastatic sites or increasing numbers of anatomic sites involved with
metastases increase the risk for failure of therapy.139,141,143,149 Prior Chemotherapy. Failure of primary chemotherapy is, arguably, the single highest risk
factor in patients with GTT. Hammond and colleagues reported a 14% salvage
rate with multiagent chemotherapy for patients with high-risk disease
who had failed primary chemotherapy versus 70% among those with high-risk
disease who are treated initially with multiagent chemotherapy.133 Since this report, numerous other series have reported that failed previous
chemotherapy is a high-risk factor.138,139,140,141,143,144,145,149 This undoubtedly is caused by multiple factors, including inappropriate
initial therapy, failure to initially diagnose high-risk sites of metastatic
involvement, emergence of drug-resistant tumor because of drug-induced
resistance or spontaneous mutations imparting resistance, alteration
of host-tumor immunologic relationships, and development of metastatic
foci that are relatively impervious to chemotherapy because
of surrounding fibrosis. Unfortunately, inclusion of patients who have
failed primary chemotherapy in several reports investigating prognostic
factors undoubtedly confounds analysis because the majority of these
patients have long duration of disease and other high-risk factors at
the time they are treated with salvage therapy. Nonetheless, these patients
are the most challenging group to treat, requiring intense therapy
and often integrating components of chemotherapy, surgery, and radiation
therapy in an attempt to optimize survival. TREATMENT. Therapy for Nonmetastatic Tumors. Before effective chemotherapeutic regimens were widely available for GTT, surgical
therapy for even nonmetastatic disease was generally unsatisfactory. Brewer
and colleagues reported a poor survival rate when hysterectomy
was used as the only treatment for choriocarcinoma.150 Since the introduction of methotrexate chemotherapy for GTT, most centers
have reported almost 100% cure rates for patients with nonmetastatic
disease using single-agent regimens. Therefore, we do not use the prognostic
factors to assign treatment of patients without evidence of
metastatic disease at the time of pretherapy metastatic survey. Methotrexate and dactinomycin have been the principle agents used for treatment
of nonmetastatic GTT; however, 5-fluorouracil and oral etoposide
have been used with excellent results. Despite the high rate of success
using primary chemotherapy, hysterectomy is still used in the treatment
of selected patients with nonmetastatic GTT and should be considered
in those who desire concurrent sterilization. Currently, many centers
are investigating options of chemotherapy that would retain a high
remission rate for this disease and reduce toxicity. Results of representative
studies using chemotherapy for nonmetastatic GTT are reviewed
in Table 5. TABLE 5. Results of Treatment for Nonmetastatic Gestational Trophoblastic
Tumors
| No. of | Remission (%) |
Chemotherapy | Patients | Primary | Overall |
Dactinomycin | | | |
5 day | | | |
Goldstein et al162 | 12 | 84 | 100 |
Petrilli and Morrow163 | 13 | 77 | |
Bolus | | | |
Petrilli and Morrow163 | 5 | 80 | |
Twiggs164 | 12 | 100 | 100 |
Petrilli et al165 | 31 | 94 | 100 |
5-Fluorouracil | | | |
Sung et al166 | 69 | 93 | |
Etoposide (VP-16), oral | | | |
Wong et al167* | 60 | 98 | 100 |
Methotrexate | | | |
5 day, intramuscular | | | |
Hammond et al142 | 47 | 93 | 98 |
Smith et all156 | 39 | 92 | 100 |
5 day, oral | | | |
Barter et al151 | 15 | 87 | |
Methotrexate/folinic acid | | | |
Berkowitz et al154 | 163 | 90 | 100 |
Smith et al156 | 29 | 72 | 100 |
Wong et al157* | 68 | 76 | 100 |
Mutch et al121 | 39 | 75 | 100 |
Bolis et al158 | 51 | 88 | 100 |
Bagshawe et al159* | 348 | 74 | 99.7 |
Weekly | | | |
Homesley et al161 | 63 | 81 | 99 |
* Includes patients with low-risk metastatic gestational trophoblastic
tumors.
Methotrexate. Methotrexate has been used in the treatment of GTT since the 1950s and
has resulted in almost 100% cure rates in patients with nonmetastatic
diseases. Methotrexate administered in a dose of 0.4 mg/kg intramuscularly
for 5 days with cycles repeated every 12 to 14 days was used as
primary therapy in 58 patients with nonmetastatic disease at NIH.133 Only four patients (7%) had tumors resistant to this first-line therapy, and
three of these were salvaged with second-line therapy with dactinomycin. Toxicity
from this regimen includes essentially universal alopecia, mucositis, significant neutropenia, and cutaneous toxicity in
approximately 70%; gastrointestinal toxicity in approximately 50%; thrombocytopenia
in approximately 40%; and symptomatic sterile inflammation
of the pleura or peritoneum in approximately 30% of patients. There
were no therapy-related deaths.134 Additional reports have documented excellent cure rates of nonmetastatic
GTT using single-agent methotrexate, but alternative methotrexate regimens
have also been designed to reduce toxicity. Barter and associates reported that 5-day cycles of methotrexate given
orally could be substituted for parenteral methotrexate.151 Thirteen (87%) of 15 patients who were treated exclusively with oral methotrexate
achieved remission. Although their retrospective review revealed
that this outpatient form of administration produced minimal toxicity,151 we have been reluctant to recommend oral methotrexate. Compliance may
be unreliable, and erratic absorption of oral methotrexate might produce
subtherapeutic or toxic levels in individual patients. Therefore, we
prefer parenteral regimens for chemotherapy for women with GTT. Bagshawe and Wilde first proposed methotrexate with folinic acid rescue
as therapy for GTT.152 The rationale for folinic acid administration is to “rescue” the
normal tissues from the dihydrofolate reductase block induced by
methotrexate, allowing a higher dose of methotrexate to be administered
with the rescue of normal tissues by folinic acid. Rotmensch and colleagues
evaluated serial methotrexate levels during both single-agent
daily methotrexate and alternating methotrexate-folinic acid therapy
for patients with GTT.153 They observed that alternate-day dosing with methotrexate resulted in
higher peak concentrations but also resulted in subtherapeutic and subtoxic
trough levels more frequently than did conventional daily methotrexate.153 This finding alone might account for the observed therapeutic effect and
diminished toxicity of this regimen compared with daily methotrexate
without any need for postulating an effect of folinic acid rescue. Various methotrexate-folinic acid schedules have been used. The New England
Trophoblastic Disease Center has reported considerable experience
with intramuscular methotrexate, 1 mg/kg, on days 1, 3, 5, and 7 alternately
with intramuscular folinic acid, 0.1 mg/kg, on days 2, 4, 6, and 8.154 A single cycle of chemotherapy was given for nonmetastatic GTT, and hCG
regression patterns were followed. If a patient had a progressive decrease
in hCG levels and entered remission, no further therapy was given. If
hCG levels plateaued for more than 3 weeks or became reelevated, patients
were re-treated. Alternate therapy with dactinomycin was used
for salvage. In the experience at this center, 147 women with nonmetastatic
and 22 with low-risk metastatic GTT have been treated with this
approach.154 One hundred twenty-one patients (82%) with nonmetastatic disease achieved
remission with one cycle of chemotherapy, whereas the remainder required
two or more cycles to achieve remission. Sixteen (10%) required
alternative therapy. Patients with nonmetastatic disease were more likely
to respond to this regimen than those with metastases. Likewise, patients
with hCG levels greater than 50,000 mIU/ml responded less frequently
than those with lower hCG levels. Toxicity was minimal, with significant
myelotoxicity observed in less than 6% and hepatic toxicity
in 14% of patients.154 Increasing the methotrexate dose to 1.5 mg/kg alternatively with folinic
acid, 0.15 mg/kg, did not improve the response rate but did increase
both significant hepatic and hematologic toxicity.155 Methotrexate-folinic acid has also been administered as repetitive cycles
until remission is achieved. Smith and associates156 and Mutch and co-workers121 used repeated courses of methotrexate, 1.0 mg/kg, on days 1, 3, 5, and 7, alternating
with folinic acid, 0.1 mg/kg, given 24 hours after each
dose of methotrexate. Wong and associates used the same schedule but
administered folinic acid rescue 30 hours after each dose of methotrexate.157 In these reports, cycles were usually repeated at 14-day intervals until
remission was achieved as determined by hCG measurements. Smith and
associates reported a higher failure rate with the cyclical methotrexate-folinic
acid regimen than with conventional 5-day methotrexate (27.5% vs. 7.7%).156 However, 4 (10%) of 39 patients treated with single-agent methotrexate
had therapy changed to dactinomycin because of significant toxicity. All
patients in their report who failed initial methotrexate-folinic acid
or methotrexate therapy were salvaged using alternative single-agent
chemotherapy.156 Mutch and colleagues, reporting from the same institution, confirmed a 26% failure
rate for cyclical methotrexate-folinic acid as primary chemotherapy
for nonmetastatic GTT.121 Eight of 10 patients who failed initial methotrexate-folinic acid chemotherapy
had small pulmonary metastases detected by pulmonary CT scanning
but not by conventional chest roentgenograms. This feature was identified
to be a poor prognostic factor for the success of this regimen, but, again, all
patients were salvaged with alternative treatment with
dactinomycin.121 Wong and co-workers likewise compared their experience with single-agent
methotrexate and methotrexate-folinic acid regimens in patients with
nonmetastatic or low-risk metastatic GTT.157 They observed a lower failure rate for methotrexate-folinic acid than
for single-agent methotrexate in similar groups of patients but noted
significantly increased hepatic toxicity in those treated with the methotrexate-folinic
acid regimen. Their protocol differed somewhat from
that used by Smith and co-workers156 in that folinic acid was administered 30 hours after methotrexate rather
than 24 hours. Additionally, they noted a high endemic rate of hepatitis
in their patient population. Bolis and colleagues reported approximately an 89% complete remission rate
among 51 women with nonmetastatic GTT who received a median two courses
of methotrexate-folinic acid to achieve normal hCG values.158 Only three (50%) of six patients with low-risk metastatic disease achieved
remission; however, all patients who failed the methotrexate-folinic
acid regimen were salvaged with alternative therapy. Bolis and colleagues
also found higher failure rates among women with pretreatment
hCG levels greater than 10,000 mIU/ml, uterine enlargement suggestive
of deep myometrial invasion, and a histologic diagnosis of choriocarcinoma.158 The largest experience with methotrexate-folinic acid was recently reported
by Bagshawe and co-workers.159 Between 1974 and 1986, 348 women with nonmetastatic and low-risk metastatic
GTT received methotrexate-folinic acid chemotherapy. Overall, 74% achieved
remission with this regimen, while 20% required alternative
therapy because of drug-resistance and 6% changed therapy because of
drug-induced toxicity. The sustained remission rate for this group of
women was 99.7%.159 Berkowitz and associates compared therapy with 300 mg/m2 methotrexate intravenous infusion over 12 hours followed by folinic acid “rescue” as
primary therapy for 32 women with nonmetastatic
GTT with their previous experience using the 8-day intramuscular
methotrexate-folinic acid regimen.160 The primary complete remission rate of approximately 69% with the methotrexate
infusion was significantly worse (p < 0.01) than their experience with the 8-day regimen toxicity. Toxicity, however, was
minimal and all patients whose disease was resistant
to the methotrexate infusion were salvaged with alternative therapy. Although
this regimen had a higher failure rate then 8-day methotrexate-folinic
acid, they believed that the shortened duration of chemotherapy
and minimal toxicity offered advantages over many other regimens.160 Holmesley and co-workers evaluated a unique regimen using weekly intramuscular
administration of methotrexate in women with nonmetastatic GTD.161 Initial therapy consisted of 30 mg/m2, with the dose progressively accelerated to 50 mg/m2 in responding patients. Eighty-two percent of their patients achieved
remission with a median of seven cycles of therapy. All nonresponders
were salvaged with alternative single-agent therapy, and no significant
toxicity was observed. The investigators concluded that this regimen
represented efficacious therapy for nonmetastatic GTT that was minimally
toxic and cost-effective. Unfortunately, all of the patients in this
series were treated for GTT diagnosed after molar evacuation.161 Although we use this regimen for patients with postmolar nonmetastatic
GTT, there is insufficient evidence of efficacy to recommend its use
in treatment of women with nonmetastatic GTT arising after nonmolar gestations. Unfortunately, no prospective randomized trial has evaluated
any of the methotrexate regimens in the treatment of women with nonmetastatic
GTT. Dactinomycin. Following the reports that patients with metastatic GTT could achieve
primary and secondary remissions with single-agent dactinomycin, Goldstein
and colleagues reported on their experience with dactinomycin given
intravenously in doses of 9 to 13 μg/kg/day for 5 days, recycled
at 14-day intervals as primary therapy in 12 patients with nonmetastatic
GTT.162 Two patients with the disease resistant to dactinomycin were salvaged
with methotrexate therapy, and all patients eventually achieved sustained
remission. The most common toxic effects included nausea and vomiting (reported
in two thirds of patients), alopecia, and transient bone
marrow depression.162 Petrilli and Morrow reported similar results with this regimen.163 There were no therapy-related deaths in either report. Because of the
more frequent gastrointestinal toxicity, alopecia, and potential for extravasation
injury, most investigators have reserved 5-day dactinomycin
as salvage therapy for patients with nonmetastatic GTT after failure
of initial methotrexate regimens. Petrilli and Morrow first proposed using a single intravenous bolus of
dactinomycin (40 μg/kg = 1.25 mg/m2) administered as a pulse every 2 weeks.163 Their rationale was that dactinomycin has a long half-life and that the
total dose administered was equivalent to the more traditional 5-day
courses. In comparative analysis, 3 of 13 patients failed 5-day dactinomycin
versus 1 of 5 patients treated with the dactinomycin bolus.163 Toxicity was similar in both regimens. Twiggs subsequently treated 12 patients
with this regimen and reported that all patients entered remission
after an average of 4.8 cycles of chemotherapy.164 There was one episode of significant thrombocytopenia in his patient population. Likewise, a
Gynecologic Oncology Group study reported on 31 patients
treated with this regimen.165 Twenty-nine (94%) achieved remission after an average 4.4 cycles of chemotherapy. There
was no grade 3 or 4 hematologic or hepatic toxicity
and only a 10% incidence of grade 3 gastrointestinal toxicity, which responded
to conventional antiemetics.165 Thus, bolus dactinomycin also represents cost-effective chemotherapy with
an acceptable remission rate but slightly higher toxicity than weekly
methotrexate. 5-Fluorouracil. Sung and associates used 5-fluorouracil 28 to 30 mg/kg/day, as a slow
intravenous infusion over 10 days to treat patients with metastatic and
nonmetastatic GTT.166 Cycles were repeated at 24- to 31-day intervals. Sixty-four (93%) of 69 patients
with nonmetastatic GTT entered sustained remission with 5-fluorouracil. Toxicity
during the first cycle of 5-fluorouracil 212 previously
untreated patients included an 11.3% incidence of severe nausea
and vomiting, 4.2% incidence of stomatitis, and 7.5% of hepatoxicity. Approximately 20% suffered diarrhea, with 15 patients developing pseudomembranous
colitis. The incidence of severe hematologic toxicity was
low, and significant toxicity was stated to be less than in the investigators' previous
experience with bolus administration of 5-fluorouracil.166 Experience with 5-fluorouracil as therapy for GTT has been limited in
reports from Western countries, but the drug must be considered an active
agent in the treatment of GTT. The 10-day hospitalization required
for the infusions and high rate of significant toxicity, however, do
not make it an attractive agent for patients with nonmetastatic disease. Etoposide. Etoposide (VP-16) has been established as an active single agent in the
therapy for GTT. Wong and colleagues used oral etoposide in doses of 200 mg/m2 for 5 days, recycled at 12- to 14-day intervals.167 Fifty-nine (98%) of 60 patients with nonmetastatic and low-risk metastatic
GTT entered remission with the regimen. One patient was changed to
methotrexate-folinic acid chemotherapy because of intolerable gastrointestinal
toxicity. All patients developed alopecia, and 25% suffered
mild to moderate myelosuppression, with only one episode of significant
neutropenia less than 1000 cells/mm3. All patients reported some degree of nausea, but only 5 required antiemetic
therapy.167 Because of the cost of oral etoposide and universal alopecia related to
this drug, most investigators in the United States have preferred to
use methotrexate or dactinomycin regimens as initial treatment for women
with nonmetastatic GTT. Surgical Therapy. Surgery alone was available as therapy for invasive mole or nonmetastatic
choriocarcinoma before the availability of methotrexate. Brewer and
colleagues reported only a 40% 2-year survival rate for women with nonmetastatic
choriocarcinoma and 15% survival for those with metastatic
choriocarcinoma who were treated with hysterectomy alone.150 In contrast, Wilson and associates locally excised intrauterine foci of
invasive mole in five patients who wished preservation of fertility.96 None of their patients received chemotherapy, and all subsequently entered
sustained remission. Since the advent of effective chemotherapy, surgical treatment of nonmetastatic
GTT has assumed a lesser role but is still helpful in managing
selected patients. Hammond and associates evaluated their experience
with surgery integrated into the treatment of patients with GTT.168 One hundred thirty-nine patients with nonmetastatic GTT were evaluated
in this report: 122 patients were treated with primary chemotherapy, whereas 17 were
treated with chemotherapy and primary hysterectomy. Hysterectomy
during the first cycle of chemotherapy significantly reduced
the number of cycles of chemotherapy necessary to produce remission
and shortened the total duration of therapy. One hundred and six (87%) of
the 122 patients treated primarily with chemotherapy achieved remission
without requiring additional forms of therapy, whereas 13 required
surgery and 3 required pelvic infusion of chemotherapy. Therefore, 89% of
patients with nonmetastatic GTT who desired preservation of fertility
were able to retain child-bearing capacity.168 We have performed primary or secondary hysterectomy under the coverage
of chemotherapy and have not observed unusual toxicity.168 Lewis and co-workers initially advocated the coverage of surgical extirpation
of GTT coordinated with a chemotherapy “umbrella” and
likewise noted no increase in wound complications or infection.169,170 The rationale for this combined approach is that chemotherapeutic coverage
destroys microscopic metastases that are undetected at the time of
surgery and also prevents establishment of any trophoblastic elements
that might be embolized intraoperatively. We generally perform an abdominal hysterectomy with preservation of the
adnexa unless there is evidence of adnexal metastases or the patient
is in the perimenopausal age-group. This allows abdominal exploration
to exclude the possibility of occult extrauterine metastases. However, we
have performed standard vaginal hysterectomies in a few patients with
nonmetastatic GTT without noting an increased rate of complications
or failure of therapy. Hysterectomy may remove foci GTT that can become relatively drug resistant
on the basis of surrounding tissue fibrosis.168 Occasionally, patients with invasive mole are found to have diffuse disease
in the endometrial cavity. In those treated with secondary hysterectomy, an
intrauterine nodule of choriocarcinoma or invasive mole is
often found to be encased in dense fibrosis that might be expected to
reduce tissue perfusion and limit exposure of neoplastic tissues to chemotherapy. General Management. Our general approach to the management of patients with nonmetastatic
GTT is outlined in Table 6. We usually use either the weekly methotrexate or 8-day methotrexate-folinic
acid regimens as initial chemotherapy and reserve dactinomycin
for salvage therapy. TABLE 6. Suggested Management of Gestational Trophoblastic Tumors
Nonmetastatic |
Initial therapy: | Single-agent methotrexate; primary hysterectomy if patient desires sterilization (only) |
Salvage therapy: | Single-agent dactinomycin; combination chemotherapy, if needed; secondary
hysterectomy |
Low-Risk/Good-Prognosis Metastatic |
Initial therapy: | Single-agent methotrexate; primary hysterectomy if patient desires sterilization (only) |
Salvage therapy: | Single-agent dactinomycin; combination chemotherapy, if needed; secondary
hysterectomy |
High-Risk/Poor-Prognosis Metastatic |
Initial therapy: | MAC* or EMA/CO† regimens; consider brain or liver irradiation for metastases |
Salvage therapy: | Individualized combination chemotherapy; specific surgical extirpation
as indicated |
* MAC = methotrexate, dactinomycin, and chlorambucil or cyclophosphamide
† EMA/CO = etoposide, methotrexate, dactinomycin/cyclophosphamide, vincristine
Therapy for Low-Risk/Good-Prognosis Metastatic Tumors. The majority of patients with low-risk/good-prognosis metastatic GTT by
the clinical classification criteria have low- or medium-risk WHO prognostic
index scores. Dating from the 1965 report by Ross and associates, which
reported a 95% complete remission rate in women with metastatic
GTT having short duration of disease and low hCG levels,133 numerous investigators have reported excellent results using either methotrexate
or dactinomycin as the initial therapy for patients with low-risk, good-prognosis
metastatic GTT. In general, the remission rates
for 5-day cycles of either agent are comparable and patients who fail
initial therapy with one agent can be salvaged with the alternative single
agent. In our experience, approximately one third of patients with
low-risk metastatic GTT will require a change from 5-day methotrexate
to dactinomycin; roughly equal numbers of patients are treated with
alternative therapy because of toxicity or the development of drug-resistant
disease, as evidenced by the development of new metastases or
nonresponse of hCG levels to initial chemotherapy. As noted earlier, patients with low-risk metastatic disease have been treated
with methotrexate and folinic acid. Complete remission rates of 50% to 68% have
been reported for patients with low-risk metastatic disease
treated with this regimen.121,154,157,158,159 All patients with resistant disease were subsequently cured with 5-day
dactinomycin or combination chemotherapy. Because of the slight lower
remission rates with methotrexate-folinic acid regimens, we have continued
to use 5-day methotrexate therapy for patients in this disease category. Pulsed dactinomycin has also been used to treat a few patients with low-risk
metastatic GTT. Petrilli and Morrow treated five patients with low-risk
metastatic disease using the pulsed dactinomycin regimen described
for patients with nonmetastatic GTT.163 All achieved remission. The major toxicity resulting from this schedule
is gastrointestinal. Further experience is needed to confirm the efficacy
of this schedule in the treatment of patients with low-risk metastatic
GTT. Both 5-fluorouracil infusional therapy166 and oral etoposide167 have been successfully used in the treatment of patients with low-risk
metastatic GTT. However, since 5-fluorouracil requires a prolonged infusion
given daily for 10 days and has significant mucosal and gastrointestinal
toxicity and etoposide causes universal alopecia, these agents
are unlikely to replace methotrexate or dactinomycin as initial therapy
for patients with low-risk metastatic GTT. Surgery. In part because of the dismal results of treatment with surgical therapy
of metastatic GTT, results of combined therapy were reported only sporadically
in the 1970s. Hammond and co-workers reviewed a series of
patients treated for GTT at our center and reported on hysterectomy applied
to therapy for patients with good-prognosis metastatic GTT.168 Approximately 13% of 40 patients with good-prognosis metastatic disease
treated initially with chemotherapy required hysterectomy to achieve
sustained remission. Additionally, performance of primary hysterectomy
in conjunction with chemotherapy reduced the time required to induce
remission and limited chemotherapy requirements compared with treatment
alone. Fifteen patients who underwent primary hysterectomy and chemotherapy
required an average of only 3.8 cycles of chemotherapy versus 5.9 cycles
among patients treated primarily with chemotherapy.168 Therefore, there is a rationale for combining primary hysterectomy with
chemotherapy in patients with limited extrauterine metastasis who desire
sterilization. General Management. Our recommended approach to patients with low-risk/good-prognosis metastatic
GTT is outlined in Table 6. We generally use 5-day intramuscular administration of methotrexate as
the initial chemotherapeutic regimen. Therapy for High-Risk/Poor-Prognosis Metastatic Tumors. As previously noted, Hammond and co-workers first reported that patients
with metastatic GTT who had one or more high-risk/poor-prognosis factors
benefited from initial multiagent chemotherapy, rather than waiting
for drug resistance to single-agent therapy to initial multiagent
treatment.134 Subsequently, most American centers have treated patients with high-risk
metastatic GTT with multiagent chemotherapy, based largely on the clinical
classification system discussed previously.136,139,140,141,143,144,145 However, not all patients with this designation have high-risk disease
by the WHO prognostic index score. Although the overall success for multiagent
chemotherapy of patients with high-risk/poor-prognosis metastatic
GTT ranges between 63% and 80% using methotrexate- and dactinomycin-based
combinations,134,136,139,140,141,143,144,145 several groups have reported that women with medium-risk disease by WHO
prognosis index score are often cured with single-agent therapy and
almost always cured with combination chemotherapy, compared with 40% to 50% among
those with high WHO prognostic index scores.138,139,140,141 Most of these series have analyzed patients treated with modifications
of MAC combination chemotherapy; recent reports have focused on treatment
of patients with regimens that employ etoposide with or without cisplatin. To
date, no study has compared the efficacy and toxicity of
etoposide- or cisplatin-containing regimens with MAC-based chemotherapy. “Triple” MAC chemotherapy consisting of methotrexate, 0.3 mg/kg
IM, dactinomycin, 8 to 10 μ/kg IV, and chlorambucil, 0.2 mg/kg
PO (or cyclophosphamide, 250 mg IV), each given daily for 5 days has
been the combination regimen most often reported in American centers.134 Cycles are repeated every 14 to 21 days and, in most American studies, patients
with brain and liver metastases are given radiation therapy, as
described subsequently. Using variations of this regimen, most investigators
have reported sustained remission rates in 60% to 80% of patients
with high-risk/poor-prognosis metastatic GTT.134,136,139,140,141,143,144,145,171,172,173 MAC chemotherapy frequently results in significant toxicity, particularly
when recycled at intervals of less than 21 days. In the mid 1970s, Bagshawe proposed a complex, alternating eight-drug schedule
incorporating methotrexate, dactinomycin, cyclophosphamide, doxorubicin, melphalan, hydroxyurea, and vincristine (CHAMOMA) in women
with high-risk metastatic GTT.174 Surwit and colleagues reported our initial experience with a modification
of this regimen, commenting on the impression of reduced toxicity
and high initial remission rates in women who had failed to respond to
MAC chemotherapy.175 However, when Weed and associates reviewed a larger series of women treated
with modified CHAMOMA, the primary remission rate dropped to less
than 60% with a much higher incidence of toxicity.176 This undoubtedly reflected the preponderance of previously treated patients
and longer follow-up in their series. Somewhat higher remission
rates have been reported in other single-arm reports. When CHAMOMA was
used as primary therapy for 50 patients with high-risk GTT, Wong and
associates reported an 82% rate of sustained complete remission.177 In summarizing the Charing Cross experience in treating women with high-risk
GTT, Newlands and associates reported a 75% remission rate among
those who received CHAMOMA.178 However, a detailed analysis, including the primary remission rate, of
these patients was not presented. The Gynecologic Oncology Group subsequently reported the results of the
only prospectively randomized trial of chemotherapy conducted for women
with GTT.172 They compared a standard MAC combination regimen recycled at 21-day intervals
to a modified CHAMOMA regimen in women with high-risk metastatic
disease. Primary remissions were achieved in 73% of 22 patients treated
with MAC versus 65% of 20 treated with CHAMOMA (p = not significant); however, the overall survival after salvage therapy
was 96% for those treated initially with MAC versus 70% for those receiving
CHAMOMA. The incidence of life-threatening hematologic and overall
toxicity was higher in patients receiving CHAMOMA (p = 0.004 and 0.014, respectively). This study was terminated early because
of the marked difference in toxicity between the two regimens. On the
basis of the similar primary remission rate and only 9% incidence of
life-threatening hematologic toxicity, it was concluded that the MAC
regimen had a more favorable therapeutic index than the modified CHAMOMA
regimen.172 Oral or intravenous etoposide is highly active in the therapy for GTT as
primary166 or salvage therapy.174 A regimen using alternating cycles of etoposide-methotrexate-dactinomycin
and cyclophosphamide-vincristine (EMA-CO, Table 7) was designed by the group at Charing Cross Hospital in London to incorporate
etoposide into the initial therapy of women with high-risk GTT.178 Newlands and co-workers reported that survival of patients with high-risk
metastatic GTT by WHO prognostic index score criteria was enhanced
using this combination when compared with previous combinations used
by their group.178 Bolis and associates also evaluated this regimen as therapy for 36 women
with high-risk/poor-prognosis metastatic GTT.179 They reported an 86% primary complete remission rate, with 76% of their
patients disease free but 12% alive with persistent hCG level elevations
despite salvage therapy at completion of their study. Only 5.5% of
patients experienced life-threatening hematologic toxicity.179 TABLE 7. EMA/CO Chemotherapy for High-Risk Metastatic Gestational Trophoblastic
Tumors
Course A |
Day 1 | Dactinomycin | 500 μg | IV bolus |
| Etoposide | 100 mg/m2 | IV infusion over 30 minutes |
| Methotrexate* | 100 mg/m2 | IV bolus |
| | 200 mg/m2 | IV infusion over 12 hours |
Day 2 | Dactinomycin | 500 μg | IV bolus |
| Etoposide | 100 mg/m2 | IV infusion over 30 minutes |
| Folinic acid | 15 mg | IM/PO q6th  4 doses 4 doses |
| | | Begin 12 hours after methotrexate infusion completed |
Course B |
Day 8† | Vincristine | 1 mg/m2 | IV bolus |
| Cyclophosphamide | 600 mg/m2 | IV infusion |
Day 15 | Recycle Course A | | |
* In patients with central nervous system metastases increase methotrexate
to 1 g/m2 as 24-hour IV infusion. Increase folinic acid to 15 mg IM/PO q8h × 9 doses
beginning 12 hours after methotrexate infusion completed.
† Patients with central nervous system metastases or with high-risk WHO
prognostic index scores receive 12.5 mg methotrexate by intrathecal injection.
(Compiled from multiple sources178,179,180,187One significant feature of this regimen is that the EMA portion can be
given during a 2-day hospitalization, whereas the CO portion can be given
on an outpatient basis. The Charing Cross group recommends administering
intrathecal methotrexate with each CO portion of the cycle to prevent
the development of brain metastases.178 This combination is attractive therapy for women with high-risk metastatic
GTT because of the inclusion of etoposide and since it has a primary
complete response rate that appears to be slightly better than that
for MAC triple therapy. However, its efficacy has not been prospectively
evaluated in randomized trials. It should also be noted that the
incidence of life-threatening hematologic toxicity with EMA-CO reported
by Bolis and associates180 was very similar to that reported for MAC by the Gynecologic Oncology
Group study.172 Theodore and co-workers incorporated cisplatin and etoposide together as
first-line therapy for patients with high-risk GTT using cisplatin 100 mg/m2 on day one, with dactinomycin 300 μg/m2 and etoposide 100 mg/m2 delivered on days 1 to 3 and 14 to 16 of each 28-day cycle.181 All eight patients with high-risk GTT who received primary chemotherapy
with this regimen responded. Despite the concerns of using cisplatin
for front-line therapy for patients with GTT, toxicity was acceptable
with no treatment-related deaths. Central Nervous System Metastasis. Patients with metastasis to the CNS have long been recognized to be at
an increased risk for failure of primary therapy compared with patients
who have metastatic disease limited to the lungs or vagina. Bagshawe
assigned CNS involvement the highest level of risk among metastatic
sites.138 Although the vast majority of patients with CNS involvement have lung
and/or liver involvement, a few series have reported CNS metastases in
patients who do not have evidence of active metastatic disease elsewhere.182 Based in part on the work by Brace,183 who reported a significant incidence of CNS control using whole-brain
irradiation, we have incorporated whole-brain radiation therapy into the
primary treatment of patients with brain metastasis. A dose of 3000 cGy
is administered concurrently with MAC chemotherapy, delivered in 10 equal
fractions. Overall survival for patients treated in this fashion
is 50%, with survival of 70% to 89% in patients treated for primary
brain metastases versus only 30% for those who receive salvage treatment
for brain metastases.143,184,185,186 In contrast, the group at Charing Cross Hospital recommends using primary
chemotherapy with EMA-CO and reported a 72% survival among patients
who received primary therapy for brain metastases using this regimen.187 They increase the dose of methotrexate to 1 g/m2 and administer intrathecal methotrexate during the CO portion of each
cycle. They also advocate early surgical intervention for patients who
have a lesion anatomically suitable for resection. Patients with CNS metastases of GTT are at risk for neurologic decompensation
caused by cerebral edema and acute hemorrhage into these highly
vascular and often centrally necrotic lesions. We routinely administer
dexamethasone throughout the course of whole-brain radiation therapy
in an effort to minimize cerebral edema. Neurosurgical consultation is
obtained early in the course of treatment, in the event that surgical
decompression and extirpation is required. Surgical extirpation is generally
reserved for patients who demonstrate neurologic decompensation
or those who require salvage therapy for recurrent CNS metastases of
GTT. Despite the fact that CNS metastasis of GTT constitutes a poor
prognosis factor in this disease entity, it should be noted that the excellent
survival of patients treated for primary brain metastases of
GTT stands in sharp contrast to the grim outlook for patients with brain
metastases from other sites of malignancy. Therefore, the diagnosis
of GTT metastatic to the brain should be entertained in any woman of
the reproductive age-group who presents with brain metastases from an
unknown primary site or unexplained CNS hemorrhage. Hepatic Metastases. Metastases to the liver are identified in 2% to 8% of patients presenting
for primary therapy of metastatic GTT.143,188 Involvement of the liver constitutes a poor prognostic factor, as evidenced
by the 40% to 50% survival rates for patients with primary involvement
at this site and dismal survival in patients who develop liver
metastases while being treated for drug-resistant disease.143,144,189 The optimal management of hepatic metastases is unknown. Hepatic metastases
tend to be highly vascular , and death is frequently caused by catastrophic
intra-abdominal hemorrhage. In an effort to minimize this
risk, we have used approximately 2000 cGy whole-liver radiation therapy
in conjunction with combination chemotherapy.189 Toxicity has not prohibited the administration of chemotherapy using this
approach. Barnard and associates reported that only 1 of 13 patients
treated with combined therapy developed postirradiation hepatitis.189 Others have reported the use of selective hepatic embolization in an attempt
to limit hemorrhage from hepatic metastases.190,191 However, the experience is too small to draw strong conclusions regarding
the most efficacious therapy for these high-risk patients. Other High-Risk Metastases. Metastatic GTT has been reported to involve virtually every organ in various
studies from prechemotherapy literature. However, metastases to
the kidneys, gastrointestinal tract, and other organs occur with a lower
frequency than brain, vaginal, or pulmonary metastases in series of
women who present for primary chemotherapy for GTT.143 Bagshawe considered renal and gastrointestinal metastases as intermediate
in risk between pulmonary or vaginal metastases and brain metastases138 but did not give survival data to justify this ranking. Gastrointestinal metastases may present as multiple submucosal metastases
along the intestine, resulting in chronic gastrointestinal bleeding, or
may result from direct invasion by pelvic disease. Unless there is
significant gastrointestinal hemorrhage from a single focus of disease, these
patients do not usually require surgery and can be treated successfully
with chemotherapy alone. In our experience, all 5 patients
with gastrointestinal or intra-abdominal metastases who presented for
primary therapy were cured.143 Renal metastasis occurred in 1.3% of 154 women who presented for primary
therapy and 14% of 42 referred for salvage therapy of metastatic GTT
at our center.192 Only 3 of 8 patients survived, all of whom presented for primary therapy
with unilateral renal metastasis and limited systemic metastases involving
the lungs only. The role of nephrectomy or radiation therapy in
the treatment of patients with renal metastases is unclear. Six of our
patients with renal metastases underwent nephrectomy and 3 survived. Nephrectomy
should be considered in the treatment of patients with unilateral
renal involvement and limited disease involving the lungs but
may not contribute to survival in cases with extensive systemic metastases.192 Irradiation of both kidneys is unlikely to achieve significant disease
control for patients with bilateral metastases given the low radiation
tolerance of the kidneys; however, unilateral renal metastases might
be treated with irradiation. Drug-Resistant Disease. Patients with high-risk metastatic GTT who have failed primary chemotherapy
are extremely challenging to treat and have a very poor prognosis. The
details of previous therapy must be reviewed completely to identify
potentially active agents that have not been used. Surgical extirpation
of drug-resistant foci of disease must be considered in patients
with limited systemic metastases. Before cisplatin and etoposide were available, salvage regimens for patients
failing MAC-type regimens were rarely successful.168,171 The CHAMOMA regimen was used as salvage therapy at our center through 1985, with
an apparent improvement in results compared with previous single-agent
and combination regimens.175,176 Although the vinblastine-cisplatin-bleomycin regimen was reported by Azab
and associates to produce high complete remission rates among their
patients with drug-resistant GTT,193 others have observed few remissions using this regimen without including
surgical resection.194,195,196 Additionally, toxicity from this regimen is often severe among heavily
pretreated patients.196 Regimens containing etoposide, both with and without cisplatin, have definite
activity in patients with drug-resistant GTT. The EMA/CO regimen178,180 and EMA portion alternating with etoposide-cisplatin178 have been successfully used as salvage therapy. Wong and colleagues used
an etoposide-methotrexate-bleomycin combination to produce remissions
in eight of nine women who experienced failure on the CHAMOMA regimen.197 Others have successfully employed etoposide-cisplatin combinations for
these extremely high-risk patients.187,198 We generally employ EMA-CO for patients who have not been exposed to etoposide, and
we have salvaged a few patients with etoposide-cisplatin
regimens who have failed EMA-CO. Another regimen that should be considered
is the etoposide-ifosfamide-mesna-cisplatin salvage regimen used
in the treatment of patients with refractory testicular germ cell malignancies.199 We have noted anecdotal responses to this regimen in heavily pretreated
patients. Therapy is often limited by accrued toxicity, and patients
must be aggressively re-treated, even in the presence of life-threatening
hematologic toxicity, in an effort to optimize the chance for survival. Surgery. Although the majority of women with high-risk metastatic GTT are not suitable
candidates for surgical extirpation based on extensive metastases
of their disease, surgery is incorporated in approximately 30% of
women with poor-prognosis metastatic GTT.168 In addition to surgical procedures aimed at extirpating sites of disease, additional
procedures are often needed to treat complications of malignancy
such as hemorrhage or infection, thus stabilizing the patient
to allow continuation of therapy. In particular, we frequently use tunnelled
central venous catheters in these patients since they often require
antibiotic therapy, support with blood products, and nutritional
support200 during the course of treatment. Hysterectomy incorporated into the primary therapy for women with poor-prognosis
metastatic GTT does not appear to be as efficacious as for those
with nonmetastatic or good-prognosis metastatic GTT.168 However, occasional patients with persistent disease confined to the uterus
can be salvaged with a delayed hysterectomy. Before hysterectomy
is performed, the patient must be carefully rescreened to rule out occult
metastatic involvement and must be able to withstand a major surgical
procedure. As in all extirpative procedures performed on patients
with GTT, we perform surgery under the umbrella of systemicchemotherapy. Usually, we
will administer single-agent therapy in an attempt to
limit toxicity. Thoracotomy with pulmonary wedge resection is the surgical procedure used
most frequently for removal of distant drug-resistant metastases from
GTT. Even though pulmonary resection can be performed safely under
the coverage of chemotherapy, it is not necessary to resect pulmonary
nodules in the majority of patients. Although those with persistent pulmonary
nodules on chest roentgenography may be at an increased risk for
recurrent GTT, radiographic evidence of tumor regression may lag far
behind the hCG level response.201 Therefore, there is little justification for resection of pulmonary metastases
that persist on chest roentgenography during chemotherapy with
a satisfactory hCG level response or after the induction of hCG level
remission.202 Many investigators have reported success with the resection of pulmonary
nodules in highly selected women with drug-resistant disease.203,204,205,206,207 Before performing thoracotomy it is important to exclude the possibility
of disease elsewhere. We perform computed tomographic evaluations of
the brain, thorax, and abdomen, as well as simultaneous CSF and serum β-hCG
levels to screen for occult extrapulmonary metastases. If
hysterectomy has not been performed, active pelvic disease should be
excluded radiographically before thoracotomy. Prognostic factors for planned resection of pulmonary metastases of GTT
have been reviewed by Tomoda and associates.206 These researchers found that the following criteria predicted a successful
resection: (1) good surgical candidate; (2) primary malignancy controlled (uterus
excised or no evidence of pelvic disease on angiography); (3) no
evidence of other systemic metastases; (4) solitary pulmonary
lesion; and (5) persistent hCG level of less than 1000 mIU/ml despite
chronic chemotherapy. In their series, 14 of 15 (93%) patients who
satisfied these criteria survived after pulmonary resection compared
with none of the 4 patients who had one or more unfavorable factors.206 Other investigators have reported that a prompt hCG level remission after
pulmonary resection predicts a favorable outcome.203,204,205,206,207 Several investigators have reported successful imaging of occult foci of
choriocarcinoma using radioimmunoscintigraphy with iodine-131-labeled
polyclonal208,209,210 or monoclonal211 anti-hCG antibodies or monoclonal antibodies directed against a human
testicular germ cell cancer.212 Because many patients with persistent or recurrent disease may have sites
of pulmonary scarring resulting from previous surgery or previous
active metastases, these techniques are promising adjuncts to conventional
imaging studies. Further investigations are needed to clarify the
sensitivity and specificity of the various radioimmunoscintigraphy techniques
in patients with GTT. Coordination of Therapy. It should be stressed that the results cited for therapy for patients
with high-risk/poor-prognosis metastatic GTT are from centers that specialize
in the treatment of women with this disease. We believe strongly
that all women with high-risk/poor-prognosis disease should be treated
in consultation with a physician at a trophoblastic disease center
or by a physician who is experienced in the management of patients with
GTT who can coordinate all aspects of therapy. A general outline of
our approach is given in Table 6. Monitoring of Patients During Therapy. Patients being treated with chemotherapy for GTT should be monitored at
least weekly using sensitive assays for serum β-hCG. Rotmensch
and co-workers have reported that women treated for nonmetastatic GTT
have a log-linear clearance of serum hCG levels after initiation of treatment.153 In our experience, patients with low-risk metastatic GTT exhibit a similar
pattern of hCG regression among patients who respond to methotrexate
regimens. A 1-log reduction in hCG is observed between the first and
second weeks of chemotherapy.213 In general, we will consider a change in regimens if there is less than 25% reduction
in the hCG level or a rise following a single course of
therapy. Chemotherapy should be continued beyond the first normal hCG
level in an attempt to prevent the development of recurrent GTT. Remission
is defined by three normal hCG levels over 14 days. After completion
of chemotherapy, patients are monitored with serial hCG values at 2-week
intervals for the first 3 months after completion of chemotherapy
and at least monthly for the first year of surveillance. Although
it is rare for a patient to develop recurrent disease more than 1 year
after remission,214 we recommend following hCG values at 6-month intervals indefinitely.153 Late recurrences have been reported several years after completion of
treatment. Recurrent Disease. Recurrent episodes of GTT are defined as reelevation of hCG levels or
appearance of new metastases after induction of remission, without an
intervening pregnancy. Recurrence is diagnosed in less than 5% of patients
with nonmetastatic or low risk metastatic GTT but in approximately 20% of
patients with high-risk disease.214 Approximately 80% of all recurrences are identified less than 12 months
after completion of chemotherapy; therefore the risk of recurrence after
the first year of normal hCG levels is less than 1% for an individual
patient.179 Patients who have been treated for one episode of recurrent GTT are at
an increased risk for a subsequent recurrence after induction of a secondary
remission and must be monitored closely after completion of chemotherapy.213 It has long been recognized that normal hCG values can be present with
a significant tumor burden. Bagshawe first recommended administering chemotherapy
after normalization of hCG values in an attempt to reduce
the risk of recurrence of GTT.138 We routinely administer one cycle of chemotherapy beyond the first normal
hCG value in patients being treated for nonmetastatic GTT, one or
two cycles for those being treated for good-prognosis/low-risk metastatic
GTT, and three or more cycles for patients being treated for high-risk/poor-prognosis
GTT. Patients who are being treated for recurrent
GTT receive additional chemotherapy in proportion to the amount of treatment
required to achieve hCG level remission. Several investigators
have reported that similar strategies of maintenance chemotherapy appear
to decrease the incidence of recurrent GTT when compared with historical
experience.135,214,215 Placental Site Trophoblastic Tumor. Placental site trophoblastic tumors are composed of intermediate trophoblastic
cells and deserve special consideration because they do not secrete
hCG to the same extent as other forms of GTT.35,36,37,38,39,40 These lesions run the gamut in clinical course from benign trophoblastic
proliferations of the placental site that can be cured with uterine
curettage to locally invasive neoplasms that will metastasize outside
the uterus in less than 20% of patients.35,36,37,38,39,40 Unlike other forms of GTT, placental site trophoblastic tumors are not
sensitive to single-agent methotrexate or dactinomycin chemotherapy. Histologic
identification of placental site trophoblastic tumor or radiographic
identification of bulky disease in conjunction with a low hCG
level should suggest the possibility of this lesion.35 Hysterectomy should be employed as primary therapy for cases of nonmetastatic
placental site trophoblastic tumors, while combination chemotherapy
should be employed for the treatment of metastatic disease. The
optimal regimen has not been identified, but two apparent complete remissions
have been reported in patients with metastatic placental site
trophoblastic tumors who received EMA-CO chemotherapy.178 Pregnancy After Treatment of Gestational Trophoblastic Tumors. Gestational trophoblastic tumors characteristically develop in women in
the prime reproductive age-group. The majority of these women can be
cured using chemotherapy alone, thus preserving the potential for child-bearing
capacity. During the first year after completion of therapy, pregnancy
is deferred so that hCG surveillance is not disrupted by an
intercurrent pregnancy. Several series of women treated with simple
chemotherapy for nonmetastatic and low-risk metastatic GTT have reported
an apparently normal reproductive capacity in women who desired child-bearing.168,216,217,218 Although there is an apparent higher incidence of spontaneous abortions, this
apparently higher abortion rate may be related to intense hCG
surveillance in these patients and might not be different from that experienced
by the general population.218 The congenital malformation rate appears to be comparable to that observed
in the general population. Although placenta accreta may be increased
in women with pregnancies after treatment of GTT,217 other obstetric complications do not appear to be increased.168,218 The only other specific increased risk after treatment for GTT is the
inherent increased risk of a repeat molar gestation. Additional information is available from China, indicating that pregnancies
after successful treatment of GTT with 5-fluorouracil or an antibiotic
chemotherapeutic agent similar to dactinomycin (KSM) resulted in
no increase in the incidence of pregnancy wastage, congenital anomalies, perinatal
mortality, or multiple gestations.219 An increased incidence of placenta accreta and postpartum hemorrhage was
noted, similar to studies in patients treated with methotrexate and
dactinomycin. Cytogenetic studies performed on 94 children revealed no
increase in chromosomal anomalies.219 Therefore, it appears that patients who have been successfully treated
for GTT and desire preservation of fertility can be encouraged in this
regard. The majority of pregnancies after treatment for GTT are uncomplicated, and
there does not appear to be an increased risk of congenital
malformations. These women should be counseled as to the increased
risk for a repeat molar gestation and should undergo an ultrasound scan
at 6 to 8 weeks of gestation to exclude the possibility of a second
mole and to confirm fetal viability. A chest roentgenogram should be
obtained with appropriate uterine shielding to exclude the possibility
of occult metastatic disease. Products of conception or placenta should
be examined histologically at the time of delivery to exclude choriocarcinoma. Six
to 8 weeks after delivery, we recommend that an hCG value
be obtained to exclude the possibility of recurrent GTT. |