Cervical cancer is the third most common gynecologic cancer in the United States with an annual incidence of 12,800 cases and 4600 deaths per year. The overall mortality from cervical cancer has decreased as a result of early detection of preinvasive disease with Pap smears; however, the mortality from invasive disease has not changed in 30 years. Carcinoma of the cervix is most commonly staged using the FIGO (International Federation of Gynecology and Obstetrics) classification that stages the tumors based on their size, local extension, and spread to adjacent or distant organs. These are evaluated by a combination of clinical and radiologic examinations that include biopsy, colposcopy, endocervical curretage, hysteroscopy, proctoscopy, intravenous pyelogram, chest x-ray and skeletal x-rays. Another important prognostic factor in cervical cancer, which is not included in FIGO classification, is the lymph node status. The preoperative evaluation of lymph node status has been done with lymphangiography, computed tomography (CT), or magnetic resonance imaging (MRI). The sensitivity of CT and MRI for detection of lymph node metastasis is not satisfactory (44% to 50%). Lymphangiography is not widely available and does not appear to be more accurate than CT or MRI. Therefore, surgical or laparascopic total pelvic lymphadenectomy and selective paraaortic lymphadenectomy are commonly performed in conjunction with hysterectomy to evaluate for lymph node involvement in surgical candidates. Patients with positive pelvic lymph nodes are treated with postoperative whole-pelvis external beam irradiation and intracavitary brachytherapy.
Several studies have reported promising results for PET imaging with FDG in diagnosis of lymph node metastases from cervical cancer. Sugawara and colleagues1 studied 21 patients with cervical cancer, 7 of whom were shown to have lymph node metastases based on surgical data and clinical or imaging follow-up. Abnormal accumulation of FDG on PET images and presence of lymph nodes greater than 1 cm in paraaortic or pelvic chain on CT scans were considered as positive for malignant. The FDG-PET scan showed a sensitivity of 86% compared to 57% for CT. The SUVs of metastatic lymph nodes ranged from 2.14 to 6.81. Identification of para-aortic nodal metastasis is of special importance because in these patients the field of radiotherapy is extended to include the abdomen up to the level of T-12 vertebra. Rose amd colleages,2 in their study of 32 patients with predominantly FIGO stage IIIB disease with no evidence of para-aortic nodal disease on CT found a sensitivity of 75% (6/8) and a specificity of 92% (22/24) for identification of para-aortic nodal metastases with FDG-PET. PET correctly identified pelvic nodal metastases in all 11 patients with pelvic nodal involvement and was superior to CT, which identified pelvic nodal enlargement only in 5 patients. Reinhardt and coworkers3 compared FDG-PET and MRI in 35 patients with FIGO stage IB and II disease. All patients had pelvic lymphadenectomy and 12 patients also had dissection of para-aortic lymph nodes. Eleven patients had lymph node metastases. The criterion for malignancy was lymph node diameter of 1 cm or greater for MRI and focal uptake of FDG in pelvic and para-aortic nodes for PET imaging. The sensitivity/specificity values of PET and MRI in diagnoisis of nodal disease were 0.81/0.99 and 0.67/0.99, respectively.3
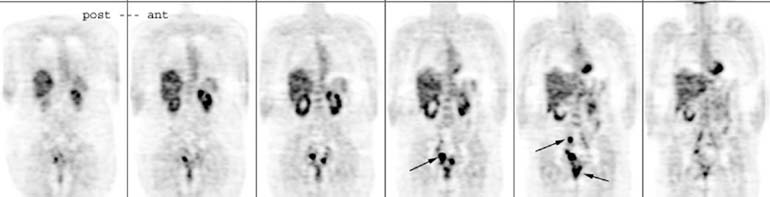
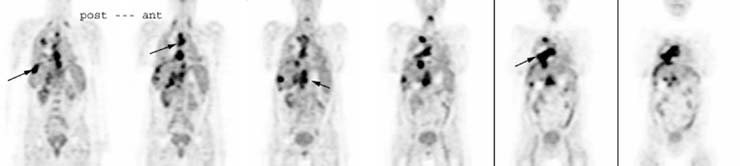
The prognostic significance of FDG uptake was addressed by Grigsby and colleagues4 in a retrospective study that included 101 patients with cervical cancer who were followed for a median period of 15.4 months after definitive irradiation and chemotherapy. Patients with negative para-aortic lymph nodes by CT had a 64% 2-year progression-free survival rate when PET was negative, but only 18% if PET showed abnormal FDG uptake. The FDG PET scan of a patient with recurrent cervical cancer is shown in Figure 1.
|
|