Basal Body Temperature In 1904, van de Velde observed that body temperature obtained at basal
level during the menstrual cycle shows a biphasic pattern. Monitoring
of basal body temperature (BBT) has been found to be one of the simplest
and most practical means of ovulation detection. In practice, women
are instructed to take their oral, vaginal, or rectal temperatures with
a basal thermometer every morning on awakening, before getting out
of bed or doing any physical activity. A period of 6 to 8 hours of uninterrupted
rest is deemed necessary before the temperature is obtained. The
temperature record shows a typical biphasic pattern during ovulatory
cycles; in anovulatory cycles it remains monophasic. A preovulatory
dip (possibly coinciding with estrogen peak) is usually, but not invariably, observed.21 The WHO definition of changes in BBT indicates that a shift in BBT to the
hyperthermia phase of the cycle should occur within a period of 48 hours
or less. Three consecutive daily BBTs should be at least 0.36°F (0.2°C) higher than the previous six daily temperatures.21 In a study of 10 normal women, cyclic fluctuations of gonadotropins and
ovarian steroids were simultaneously measured and correlated with the
BBT. The mean BBT was 97.48°F ± 0.25° (36.37°C ± 0.12°) during the follicular phase and 98.09°F ± 0.22° (36.72°C ± 0.12°) in
the luteal phase. The BBT began to rise simultaneously with the LH surge. A
significant rise did not occur until 2 days after the LH peak. This
coincided with the rise of serum progesterone to a mean level above 4 ng/mL
and urinary pregnanediol to greater than 1.8 mg per 24 hours (see Fig. 1 and Fig. 3). After the rise, the BBT remained 98°F until serum progesterone
declined below 4 ng/mL and urinary pregnanediol to less than 1.8 mg
per 24 hours. The BBT rose significantly during midcycle above the follicular
phase level and increased further to a highly significant degree
during the luteal phase.2 These observations confirm that the rise of BBT precedes or coincides
with ovulation and is associated with the increased production of progesterone
by the ovary. The BBT record does not predict the day of ovulation
but rather provides evidence of ovulation 2 or 3 days after it has
occurred.2,21,22 Biphasic BBT is usually indicative of an ovulatory cycle, although a monophasic
BBT may be observed in some ovulatory cycles.23,24 The reason for the absence of thermogenic response to ovulatory levels
of progesterone in these cases is unknown. The rise in temperature is
secondary to progesterone, and the primary reason for the rise is the
increase in the production and secretion of norepinephrine, which is
a thermogenic neural hormone. 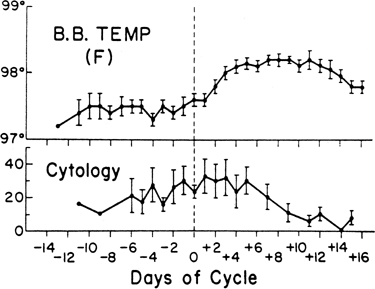 Fig. 3. Basal body temperature and karyopyknotic index of vaginal cytology throughout
the menstrual cycle in 10 ovulatory women. Day 0 = day of
luteinizing hormone surge (dotted line). Vertical bars represent one standard error of the mean.(Moghissi KS, Syner FN, Evans TN: A composite picture of the menstrual
cycle. Am J Obstet Gynecol 114:405, 1972.) Fig. 3. Basal body temperature and karyopyknotic index of vaginal cytology throughout
the menstrual cycle in 10 ovulatory women. Day 0 = day of
luteinizing hormone surge (dotted line). Vertical bars represent one standard error of the mean.(Moghissi KS, Syner FN, Evans TN: A composite picture of the menstrual
cycle. Am J Obstet Gynecol 114:405, 1972.)
|
The reliability of BBT to detect ovulation has been studied repeatedly. In
a retrospective assessment of 210 biphasic BBT records, the thermal
nadir occurred within 1 day of the urinary LH surge in 75% of
the cases and in 90% within 2 days.25 In the prospective study reported by Guermandi and colleagues11BBT records were compared to LH, E2, and progesterone in the serum and follicular collapse demonstrated by
daily ultrasound. BBT reading showed 0.77 sensitivity, 0.33 specificity, and 0.74 accuracy
for ovulation documentation. In infertility evaluation, the patient should be instructed to record her
BBT during the entire course of the menstrual cycle for several months. This
is done in an effort to document the occurrence as well as normalcy
of the ovulatory process. A prolonged follicular phase and short
luteal phase (less than 12 days’ duration) may be contributing
factors to infertility. Several computerized or digitalized BBT recording devices have been developed
to identify the fertile period more accurately. The Thermodigital
thermometer is a solid-state electronic oral thermometer that uses
microcomputer-assisted, repeated calculations to give a digital LCD in 60 seconds. The
Rabbit Computer Corporation (Los Angeles, CA) has developed
a fertility indicator for home use called The Rabbit. This device
uses BBT measurement and a built-in computer program to predict the
preovulatory period by documenting prior cycle lengths. The device also
has a built-in alarm to awaken the user and can visually graph out
up to 12 prior cycles of BBT measurement. Two other sophisticated, but rather expensive, devices available are the
Rite Time (Rite Time Ltd., United Kingdom) and Fertil-A-Chron (Fertil-A-Chron
Inc., Hauppauge, NY). The latter product incorporates an electronic
digital oral probe and an alarm system to remind the user to take
her BBT. A device called Bioself Fertility Indicator (Bioself Distribution SA, Geneva, Switzerland) has
been marketed for the purpose of integrating findings
of BBT and menstrual cycle records.26 It consists of an electronic thermometer that registers the daily morning
temperature, as well as the first day of each menstrual cycle. A unique
algorithm programmed into the microprocessor chip calculates when
the temperature shifts from the lower to the higher level after ovulation. The
method is based on a calculation involving the observation
of about six menstrual cycles and the deduction of 18 days from the shortest
cycle and 9 days from the longest. The interval between these two
points represents the fertile period of the following cycles. The use
of this device as a contraceptive in field trials has been reported
to result in a pregnancy rate of 9 per 100 women year and the 1-year
discontinuation of 32.5%.27 Another device, the Ovudate fertility test kit (Franklin Diagnostics Inc., Morristown, NJ), measures core temperature using a first morning
urine sample. Royston,28 in collaboration with a WHO task force, has shown that a modified form
of cumulative sum test (CUSUM), a method commonly used in industrial
quality control to detect drift away from a preset target value, may be
used as a sensitive and reasonably reliable method for picking up a
signal represented by a change in the mean level of serial hormone or
BBT readings. By a simple extension, one can also find peak values that
correspond approximately to ovulation. Distinctive and valuable features
of the CUSUM analysis are that it may be used prospectively in the
current cycle to monitor changes as they occur, and it may be applied
to detect ovulation electronically. Tests Based on Cervical Mucus Secretion of cervical mucus is regulated by ovarian hormones. Estrogen
stimulates the production of large amounts of thin, watery, alkaline, acellular
cervical mucus with intense ferning, spinnbarkeit, and sperm
receptivity. Progesterone inhibits the secretory activity of cervical
epithelia and produces scanty, viscous, cellular mucus with low spinnbarkeit
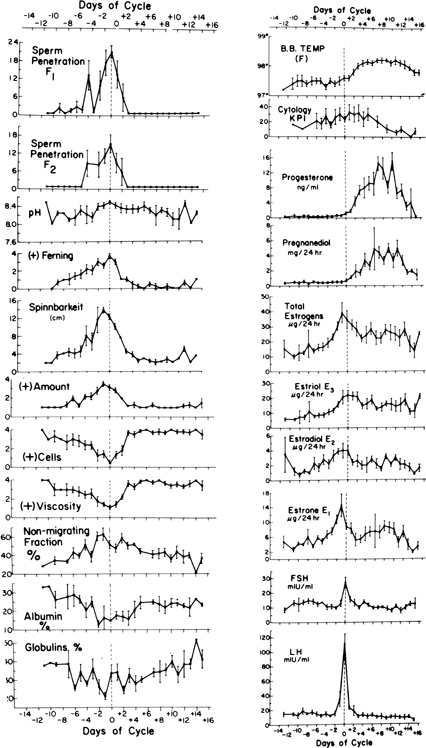
and absence of ferning, which is impenetrable by spermatozoa. Changes of various properties of cervical mucus related to gonadotropins
and sex steroids during a normal menstrual cycle in 10 women are shown
in Figure 1. The preovulatory peak of urinary estrogen coincides with cervical mucorrhea
exhibiting high spinnbarkeit and ferning, low cell count, and viscosity. The
lowest value for albumin and globulin, the highest percentage
of mucin (electrophoretically nonmigrating fraction), and the greatest
volume of mucus and spinnbarkeit precede the rise of LH and occur
simultaneously with the estrogen peak. The lowest cell count, maximal
ferning, and sperm penetration coincide with the midcycle surge of
LH the day after the preovulatory estrogen peak. Other investigators have
repeatedly confirmed these observations. Changes in the appearance of the cervix and physical properties and chemical
constituents of cervical mucus form the basis for many tests commonly
used to determine the time of ovulation. These include the appearance
of the cervix, midcycle mucorrhea, crystallization (ferning), spinnbarkeit, viscosity
or consistency, and cyclic changes of various constituents
of cervical mucus. The appearance of the cervix varies during the menstrual cycle. In midcycle, the
cervix softens progressively, the os dilates, and clear, profuse
mucus exudes from the os. Within a few days after ovulation, the
cervix becomes firm and the os is closed and covered by scanty, turbid, tenacious
mucus. Women can be taught to palpate the cervical os, inspect it through a speculum
daily, and examine the cervical mucus and detect by this means
the ovulatory period.29 Billings and coworkers30 reported that women who were adequately instructed were able to predict
and identify the approximate time of ovulation by recognizing increased
midcycle mucous discharge, which occurred at about the time of ovulation. In 22 subjects, the authors measured plasma LH and urinary total
estrogens and pregnanediol daily in midcycle to provide a hormonal
estimate of the day of ovulation. A characteristic lubricative mucus identified
by all the women occurred from 2 days before to the day of ovulation. The
onset of perceptible mucorrhea occurred 6.2 days (mean) before
ovulation. The authors concluded that the time of ovulation could
be identified clinically by recognizing increased midcycle mucous discharge. Hilgers
and associates31 confirmed that ovulation was estimated to occur from 3 days before to 3 days
after the peak mucous symptoms, with a mean of 0.31 days before
the peak symptoms. Midcycle mucorrhea, ferning, spinnbarkeit, and lowered cell content and
viscosity of cervical mucus are used commonly in ovulation detection
and as an index of estrogenic response of the cervical epithelium. However, these
changes extend over several days (see Fig. 1). Only rarely do favorable changes in cervical mucus occur abruptly and
persist for only 1 to 2 days in the cycle.32 Hence, to determine the time of ovulation by this means, serial observations
would have to be made during midcycle. Intense ferning, high spinnbarkeit, and
low consistency do not necessarily indicate ovulation
and are merely an index of an optimal amount of circulating estrogen that
may be also observed in anovulatory cycles. Changes in cervical mucus
in the opposite direction indicate a postovulatory progesterone effect. In
the presence of endocervicitis, assessment of cervical mucus
may be difficult or impossible. SPINNBARKEIT OR FIBROSITY. This refers to the capacity of cervical mucus to be drawn into threads. The
simplest technique for performing this test consists of stretching
an adequate amount of cervical mucus between a glass slide and a coverslip. The
length of the mucous thread is measured in centimeters just
before it breaks. Alternatively, the mucous sample may be aspirated
into a capillary tube; the tube is broken and the ends drawn slowly apart
against a scale marked in centimeters until the mucous thread parts (Fig. 4).  Fig. 4. Technique of evaluating spinnbarkeit of cervical mucus. Fig. 4. Technique of evaluating spinnbarkeit of cervical mucus.
|
FERNING OR CRYSTALLIZATION. Papanicolaou discovered the fact that cervical mucus, when spread on a
glass slide and allowed to dry, exhibited an intriguing pattern of arborization
with crystallization. He also observed the relation between
crystallization and estrogen activity. Ferning results where true crystals
of sodium and potassium chloride form around a small and optimal
amount (1% to 15%) of organic matter. Ferning appears between
days 8 and 10 of a typical cycle and peaks at ovulation. Immediately
after ovulation, it decreases or disappears (Fig. 5). 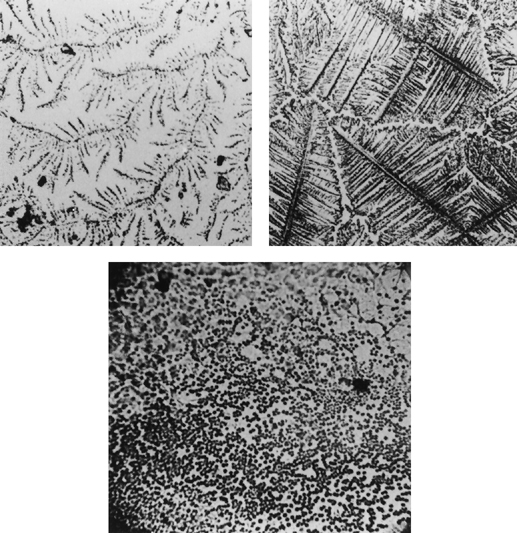 Fig. 5. Ferning (crystallization) of cervical mucus. Preovulatory ferning (top right), atypical ferning (top left), and absent ferning (bottom). Fig. 5. Ferning (crystallization) of cervical mucus. Preovulatory ferning (top right), atypical ferning (top left), and absent ferning (bottom).
|
|