This chapter should be cited as follows:
Koigi MK, Kihara AB, et al., Glob Libr Women's Med
ISSN: 1756-2228; DOI 10.3843/GLOWM.417843
The Continuous Textbook of Women’s Medicine Series – Gynecology Module
Volume 1
Female genital mutilation
Volume Editor:
Professor Anne-Beatrice Kihara, University of Nairobi, Kenya,
President-elect. The International Federation of Gynecology and Obestetrics FIGO
President, African Federation of Obstetricians and Gynecologists (AFOG)
Special Feature
Female Genital Mutilation/Cutting (FGM/C) Screening Tool
First published: July 2022
FGM/C SCREENING TOOL
DATE _____/_____/________
NAME: __________________________________________________________________ AGE: _____
- Do you know what Female Genital Mutilation/Cutting (FGM/C) is? Yes/No
If yes, specify: ____________________________________________________________________________________________________________________
___________________________________________________________________________________________________________________________________
___________________________________________________________________________________________________________________________________
___________________________________________________________________________________________________________________________________ - Have you ever had any injury or cut to the female genital organs for non-medical reasons? Yes/No
If yes, tick the appropriate one: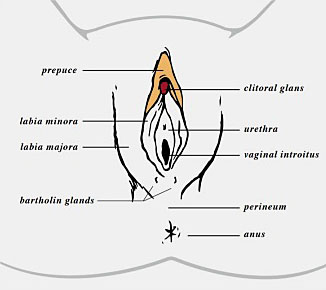
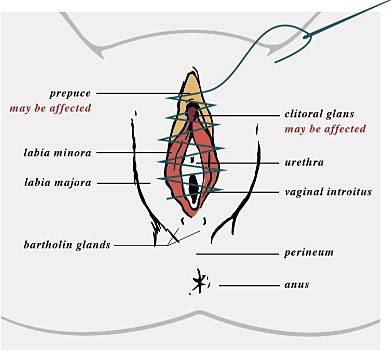
I (a) Removal of the prepuce only
I (b) Removal of the clitoris and prepuce
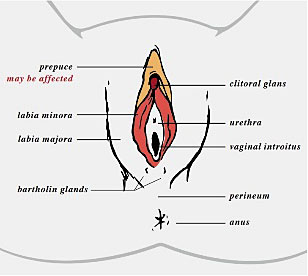
II (a) Removal of the labia minora only
II (b) Partial or total removal of the clitoris, and labia minora
II (c) Partial or total removal of the clitoris, labia minora and labia majora
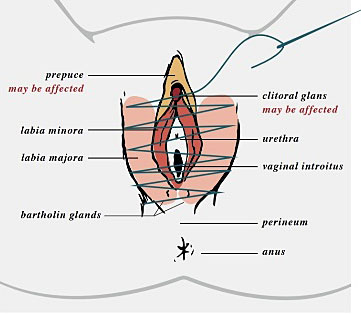
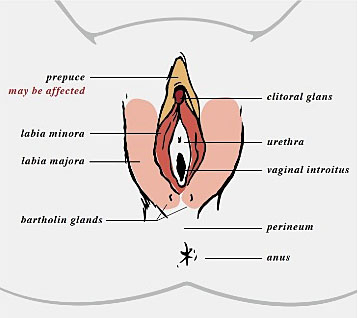
III (a) Removing and closing the labia minora
III (b) Removing and closing the labia majora
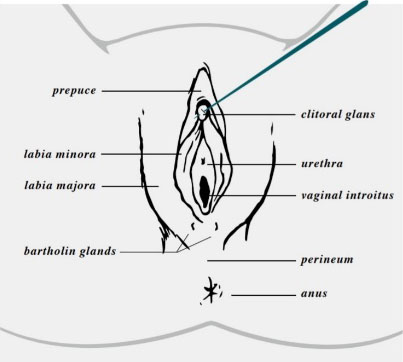
IV Pricking, piercing, incising, scrapping, burning
- How old were you when you went through this experience? _____ years
- Did anyone ever give you a reason to try to make you agree to have the cut? Yes/No
If yes, were any of these reasons part of what was used to make you agree to have the procedure? (Tick all that apply)
- To get rid of bad luck/evil spirits
- To make you more attractive
- To preserve your virginity and chastity
- It is a tradition in the family/community
- To make future child birth safer
- To uphold the honor of the family
- A rite of passage into womanhood
- To make you “marriageable”
- It is a religious obligation
- To cleanse and purify you
- So that you could remain part of the family
- You had no choice, so no reason was given to you
- ( )
- ( )
- ( )
- ( )
- ( )
- ( )
- ( )
- ( )
- ( )
- ( )
- ( )
- ( )
Any other reason (specify): __________________________________________________________________________________________________
________________________________________________________________________________________________________________________________
________________________________________________________________________________________________________________________________ - How many daughters are there in your home? _____
- How many daughters in the home are younger than you? _____
- How many daughters in the home have not yet had a similar experience? _____
- Did you experience any complications after the procedure? Yes/No
If yes, specify: ____________________________________________________________________________________________________________________
___________________________________________________________________________________________________________________________________
___________________________________________________________________________________________________________________________________
___________________________________________________________________________________________________________________________________ - Do you recall who did the procedure? Yes/No
If yes, specify: ____________________________________________________________________________________________________________________
___________________________________________________________________________________________________________________________________
___________________________________________________________________________________________________________________________________
___________________________________________________________________________________________________________________________________ - Has anyone else in your family had an experience like the one that you have had? Yes/No
If yes, specify: ____________________________________________________________________________________________________________________
___________________________________________________________________________________________________________________________________
___________________________________________________________________________________________________________________________________
___________________________________________________________________________________________________________________________________