Colposcopy
Authors
INTRODUCTION
Colposcopy is an office-based technique designed to diagnose preclinical cervical neoplasia. The technique was introduced into mainstream gynecology in the United States in the late 1960s.
In 1925, it was theorized that the earliest cancers of the cervix might be visualized as ulcers or tumors if adequate magnification and illumination were available. It was soon recognized that the earliest preinvasive conditions were not gross ulcerations or tumors but changes in the vascular pattern of the epithelial capillaries by the dense crowding of epithelial cell nuclei. It is the vascular pattern and epithelial opacity that colposcopists now evaluate for evidence of preinvasive cervical lesions, also known as cervical intraepithelial neoplasia (CIN).
CONTEMPORARY INDICATIONS FOR COLPOSCOPY
Clinical practice guidelines published by the American College of Obstetricians and Gynecologists (ACOG)1 and the American Society of Colposcopy and Cervical Pathology (ASCCP)2 describe contemporary indications for colposcopy. In general, colposcopy is indicated as a response to an abnormal cytologic test and is appropriate for surveillance after treatment of CIN.
Response to abnormal cytology
The major abnormal cytologic categories as defined by the Bethesda System and recommended action plans by ACOG and ASCCP are shown in Tables 1–3. Recommendations differ for women under age 21 years and pregnant women; separate tables are provided for these women. Of note, endocervical curettage and endometrial biopsy are contraindicated in pregnancy.
Table 1. Clinical actions for abnormal cytologic diagnoses: women aged 21 years and older
HPV, human papillomavirus; SIL, squamous intraepithelial lesion.
HSIL+ indicates HSIL, AGC, adenocarcinoma in situ and/or cancer.
ASC-US+ indicates ASC-US, ASC-H, LSIL and/or HSIL+.
Table 2. Clinical actions for abnormal cytologic diagnoses: women under age 21
| Cytology interpretation | Action |
| Epithelial cell abnormalities | |
| Atypical squamous cells of undetermined significance (ASC-US) | Repeat cytology at 12 months (perform colposcopy if ASC-H or HSIL+) and at 24 months (perform colposcopy if ASC-US+). If normal at both 12 and 24 months, resume routine screening |
| Atypical squamous cells, cannot exclude HSIL (ASC-H) | Colposcopy |
Low-grade SIL (LSIL)
| Repeat cytology at 12 months (perform colposcopy if ASC-H or HSIL+) and at 24 months (perform colposcopy if ASC-US+). If normal at both 12 and 24 months, resume routine screening |
| High-grade SIL (HSIL) | Colposcopy |
| Squamous cell carcinoma | Colposcopy |
| Glandular cell abnormalities | |
| Atypical glandular cells (AGC) | |
| Endocervical | Colposcopy with endocervical curettage |
| Endometrial | Colposcopy with endocervical curettage and endometrial biopsy |
| Not otherwise specified | Colposcopy with endocervical curettage; perform endometrial biopsy if abnormal bleeding, chronic anovulation |
| Adenocarcinoma in situ (AIS) | Colposcopy with endocervical curettage and endometrial biopsy |
HPV, human papillomavirus; SIL, squamous intraepithelial lesion.
HSIL+ indicates HSIL, AGC, adenocarcinoma in situ and/or cancer.
ASC-US+ indicates ASC-US, ASC-H, LSIL and/or HSIL+.
Table 3. Clinical actions for abnormal cytologic diagnoses: pregnant women
| Cytology interpretation | Action |
| Epithelial cell abnormalities | |
| Atypical squamous cells of undetermined significance (ASC-US) | Repeat cytology at 6 months; if ASC-US+, perform colposcopy 6 weeks postpartum |
| Atypical squamous cells, cannot exclude HSIL (ASC-H) | Colposcopy† |
| Low-grade SIL (LSIL) | Colposcopy† |
| High-grade SIL (HSIL) | Colposcopy† |
| Squamous cell carcinoma | Colposcopy† |
| Glandular cell abnormalities | |
| Atypical glandular cells (AGC) | |
| Endocervical | Colposcopy† |
| Endometrial | Colposcopy† |
| Not otherwise specified | Colposcopy† |
| Adenocarcinoma in situ (AIS) | Colposcopy† |
HPV, human papillomavirus; SIL, squamous intraepithelial lesion.
HSIL+ indicates HSIL, AGC, adenocarcinoma in situ and/or cancer.
ASC-US+ indicates ASC-US, ASC-H, LSIL and/or HSIL+.
†Endocervical curettage and endometrial biopsy are contraindicated in pregnancy.
Surveillance after treatment of high-grade CIN
ACOG and ASCCP guidelines are similar concerning the use of colposcopy for surveillance after treatment of CIN 2 or 3. ACOG guidelines state that for women aged 21 years and older who have been treated for CIN 2 or 3, several different strategies may be adopted: (1) cytology at 6 and 12 months; (2) cytology with colposcopy at 6 and 12 months; and (3) HPV DNA testing at 6–12 months. If cytology is normal twice or if HPV DNA testing is normal once, annual screening for at least 20 years is recommended. If any test is abnormaol during the first 12 months after treatment, colposcopy is recommended. For women aged 20 and younger, the ACOG guidelines state that cytology alone is preferred.
ACCURACY OF COLPOSCOPY
Colposcopy has limitations. In 2001, screening outcomes in 1997 previously unscreened women in rural China were reported.1 This study is remarkable in that clinicians performed colposcopy and four-quadrant biopsies in all women, regardless of the findings, thereby avoiding referral bias. Sensitivity of colposcopy was reported as 81% for CIN 2+ and 91% for CIN 3+. Sensitivity for cancer was 100%. Specificity for CIN 2+ was 77% and unreported for the other levels of disease. More recently, colposcopy was reported to have much lower sensitivity in the screening setting than in the diagnostic setting when applied to women in the US and Canada.2 Despite these limitations, cytology-based screening that incorporates colposcopy has accompanied declines in the cervical cancer morbidity and mortality in the United States.
PRINCIPLES OF COLPOSCOPY
The normal transformation zone
The lining of the cervix consists of two cell types. Columnar epithelium lines the endocervical canal and is composed of a single monolayer of mucus-producing cells that form epithelial fronds or “grape-like” structures visible through the colposcope. When columnar epithelium extends onto the ectocervix, it appears as a red zone surrounding the os and is called ectropion or ectopy. Squamous epithelium, on the other hand, is smooth, pale pink in color, and consists of a stratified layer of up to 20–30 cells thick. The squamous epithelium of the vagina and cervix is nonkeratinized. The junction between columnar and squamous cell types is called the squamocolumnar junction (SCJ), which in younger women is usually visible on the ectocervix. The colposcopic appearance of a normal squamous and columnar epithelium and the SCJ is shown in Fig. 1A and B.
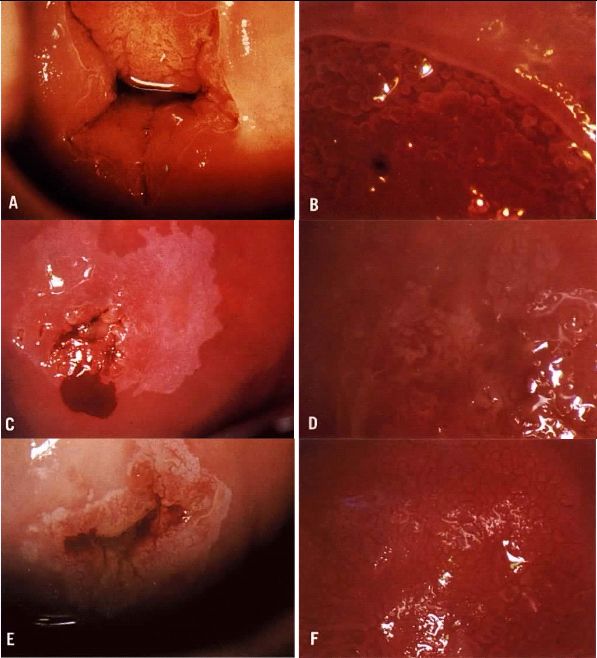
Fig. 1. (A) and (B) Normal cervix, nulliparous patient. The opened speculum has exposed the columnar epithelium surrounding the os and is in the endocervical canal. Higher magnification shows the junction between columnar and squamous epithelia. The faint white line is the transformation zone, which is quite narrow in this patient. (C) Acetowhite epithelium surrounding an area of columnar epithelium. The border, with the surrounding squamous epithelium is irregular. (D) Atypical transformation zone showing an area of punctation in the center of the photograph and a separate island of mosaic in the upper right corner. Note the varying size of the mosaic tiles, but uniform size of the punctate vessels. Biopsy showed CIN 2. (E) Atypical transformation zone showing mosaic tiles. The border is distinct, but irregular. Biopsy showed CIN 1. (F) Large acetowhite lesion showing predominantly mosaic changes. Note the distinct border in the upper right as well as the varying intercapillary distances and punctate vessels within the mosaic tiles (“umbilication”). Biopsy showed CIN 3. Patient refused therapy. Microinvasive carcinoma was diagnosed 4 years later.
The transformation zone (TZ) is the area between mature squamous epithelium distally and columnar epithelium proximally, and is the site of active squamous metaplasia. At any one time, the TZ may have columnar epithelium, squamous metaplasia and squamous epithelium present. The TZ moves cephalad as a woman ages. In younger women, the TZ is usually found circumferentially at the external cervical os, whereas in older women it may have receded within the endocervical canal. Thus, in postmenopausal women, the presence of ectropion is uncommon. When a woman becomes pregnant, the cervix markedly increases in size and weight. Concomitant with the size increase, there is usually an eversion of the endocervical (columnar) epithelium.
Over 90% of cervical neoplasia occurs in the cervical TZ. The reasons for the susceptibility of the TZ for neoplastic transformation are not known, but may be related to increased cell proliferation and tissue remodeling secondary to squamous metaplasia in the TZ, propensity of the TZ to be infected with human papillomavirus (HPV), and the high concentration of inflammatory and immune cells in the TZ.3
Given the fact that the TZ is the “hotspot” for neoplastic transformation, the goal of colposcopy is to identify the TZ, assess whether it can be seen in its entirety, identify any abnormal areas, and obtain appropriate samples for histological assessment. The overarching goal is to identify the highest grade of disease present in order to determine the need for and type of treatment.
The atypical transformation zone
In a patient with abnormal cytology, colposcopy is performed to identify abnormal areas in the TZ that correspond to the cytologic findings. Most neoplastic changes are not visible to the naked eye but are visible under binocular magnification after application solution of 3–5% acetic acid. Although the exact mechanism of action of acetic acid is not known, any area with an increased nuclear/cytoplasmic ratio such as CIN will reflect more light back to the colposcope and hence appear white after the application of dilute acetic acid.
When a white area is observed on the cervix prior to the application of acetic acid, it is called leukoplakia. These areas represent hyperkeratosis and can be associated with infection by HPV, chronic trauma or scarring. It is generally recommended that biopsy of at least one representative area of leukoplakia be performed during a colposcopic examination.
Acetowhite epithelium
Areas that appear white after the application of acetic acid are called acetowhite epithelium (Fig. 1C, 1E). These areas can be observed either within or outside the TZ. Because squamous metaplasia has an increased nuclear/cytoplasmic ratio, it will also appear faintly white. However, the acetowhitening of CIN is usually much more distinct than that of squamous metaplasia. If the full SCJ can be seen, the colposcopy is deemed satisfactory. If the acetowhite epithelium extends into the cervical canal, an instrument called an endocervical speculum can be used to identify the extent of the lesion and to visualize the SCJ (Fig. 2E, 2F). If the SCJ cannot be seen, the colposcopy is termed unsatisfactory.
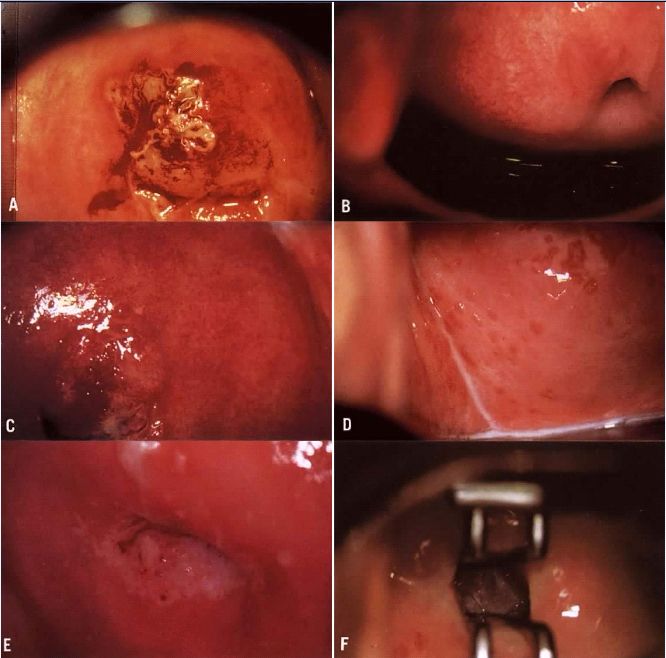
Fig. 2. (A) Atypical vessels. The lesion on the anterior lip of the cervix exhibits large vessels running horizontal to the surface. The border is very distinct and the edge is raised. The lesion color is more yellow than white. Biopsy revealed invasive squamous carcinoma to a depth of 4 mm. Conization was consistent and radical hysterectomy found no evidence of disease spread. Patient is alive and well 17 years later. (B) Normal network of capillaries beneath normal epithelium, which is transparent. (C) Bacterial vaginosis. Note the blurring of the margins of the subepithelial vessels. The squamous epithelium remains transparent. (D) Trichomonas cervicovaginitis. The “strawberry spots” are actually dilated vessels. They do not exhibit abnormal branching. (E) White epithelium on the posterior lip of the cervix. The examination is unsatisfactory because the entire transformation zone cannot be see and the extent of the lesion is not known. (F) An endocervical speculum is used to expose the upper extent of the lesion. Although seen entirely, an excisional procedure rather than ablative is suggested due to the endocervical extension.
Acetowhite epithelium should be assessed colposcopically for the presence of vascular patterns, borders with surrounding tissues, color, surface contour, and iodine uptake. Numerous scoring systems have been devised to assist the colposcopist in grading lesions based on these features.4, 5, 6 Attention to each of these qualities will assist the colposcopist to select the most significant abnormalities for biopsy. The appearance of borders and vascular patterns often can be enhanced by use of the green filter.
Vascular patterns
CIN results in changes in the epithelial vasculature. Normal vessels are confined to the stroma below the epithelium and may be visible as a fine reticular pattern (Fig. 2B). The neoplastic tissue produces angiogenic factors such as vascular endothelial growth factor, which promotes the growth of new vessels (neovascularization).7
In CIN lesions, vessels can be found within the epithelium itself rather than confined to the area below the epithelium. Intraepithelial vessels that form loops towards the epithelial surface appear colposcopically as red spots on the surface of acetowhite epithelium. This pattern is called punctation. It can be either fine or coarse, depending of the size of the vessels within the fibrovascular core.
In other cases, the intraepithelial vessels do not form simple loops to the epithelial surface but run along the surface and communicate with each other, appearing colposcopically as a pattern of red lines around an epithelial core. This pattern is called mosaicism (Figs. 1D, 1E, and 1F). As with punctation, mosaicism can be graded as fine or coarse depending on the diameter of the vessels. A coarse vessel pattern may indicate a higher grade lesion than a fine pattern.
When microinvasive or invasive cancer is present, the vascular pattern often includes the present of “atypical vessels” (Fig. 2A).8 This term should not be used to describe punctation or mosaic patterns. Atypical vessels typically have irregular enlarged caliber, form bizarre patterns and shapes such as spirals or commas, and do not follow the typical branching patterns described above. The finding of atypical vessels warrants biopsy to determine whether invasive cancer is present. Atypical vessels can also be more friable than normal vessels, hence areas of frank bleeding are suspicious for cancer.
Borders
Histologically, there is a sharp demarcation between CIN lesions and the adjacent normal epithelium. Therefore acetowhite lesions with a sharp well-demarcated border on all sides (360°) are more likely to be high-grade than are acetowhite lesions with indistinct borders. Areas of squamous metaplasia can demonstrate diffuse, poorly defined borders because the process of maturation is a continuous process, and squamous metaplasia fuses with the normal squamous epithelium at the distal margin. Borders can be smooth and sharp or jagged, feathery and angular. In general, the sharper and smoother the border, the more likely it is that a high grade lesion is present.
Surface contour
A smooth, regular surface contour is normal in mature squamous epithelium. Cervical warts may have a papillary, cauliflower-like surface contour. In areas of invasive carcinoma, the surface contour may be grossly uneven with raised nodular areas or exophytic growth. An area of frank ulceration is also suggestive of invasive cancer and is termed erosion (Fig. 2A).
Color
The quality of the color of acetowhite epithelium may be helpful in assessing lesion severity. Squamous metaplasia is usually a more opaque white than the thicker white of a high grade CIN lesion. Cervical warts are usually a bright pure white color compared to the gray or yellowish tones of invasive cancer.
Lugol’s uptake
Lugol’s is a concentrated solution of iodine that reacts with the glycogen in normal squamous epithelium to make it appear dark brown. High-grade CIN lesions have low amounts of glycogen because the epithelium is poorly differentiated, and hence they do not turn brown with Lugol’s solution. This is termed Lugol’s nonstaining or Lugol’s negative. Historically, this used to be referred to as the Schiller’s test. Lugol’s can be useful for determining whether a colposcopically equivocal area warrants biopsy: Lugol’s staining areas are most likely normal epithelium, whereas Lugol’s nonstaining areas may be CIN, metaplasia, or inflammation.
Inflammation
The presence of infection or inflammation may complicate the colposcopic examination. When bacterial vaginosis, trichomoniasis, or candidiasis is present, there is often considerable discharge, as well as some hyperemia that may make evaluation of the cervix difficult (Fig. 2C). Trichomoniasis may cause dilated capillary loops (strawberry spots) that can be interpreted as coarse mosaicism (Fig. 2D). If possible, cervicovaginitis should be treated before colposcopy is performed.
COLPOSCOPIC TECHNIQUE
Colposcope
OVERALL DESIGN
The colposcope is a steroscopic microscope with a long focal length (typically 30 cm) in order to be able to focus on the cervix. If the focal length is not long enough, the colposcope will be in the way of biopsy instruments. Colposcopes are available in different sizes to accommodate differences in working space. The colposcope can be mounted on a floor stand (Fig. 3A) or on a swivel arm affixed to a floor stand, to the wall, or to the exam table. The swivel arm may be accessible from above the examiner (Fig. 3B) or from the side (Fig. 3C). The image is brought into focus by either coarse or fine adjustment of the focal length. Coarse focus is achieved by changing the distance between the eyepiece and the patient, either by moving the entire instrument itself or by moving the flexible arm. Fine focus is available on some instruments with a handle or a knob that moves the eyepieces only.
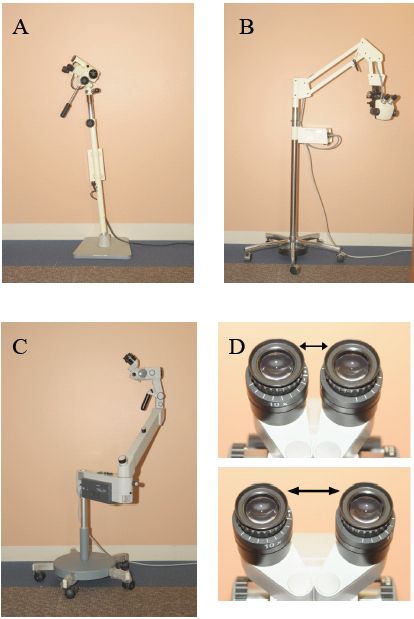
Fig. 3. The colposcope can be mounted on a floor stand (A), an overhead arm (B) or a side arm (C). Eyepieces can be adjusted to accommodate different interpupillary distances (D).
LIGHT SOURCE
A strong light source is essential. All colposcopes should be fitted with a red-free (green) filter that can be swung in front of the light source. The green filter reduces the amount of illumination minimally while enhancing the contrast of acetowhite epithelium and vascular patterns.
MAGNIFICATION
Most colposcopes have a range of magnification settings, usually between 2 and 40x. Ideally the colposcope will have at least three magnification lenses that span from low to high magnification. Some colposcopes have a zoom lens that allows for a continuous range of magnification.
EYEPIECES
The distance between the eyepieces should be adjustable so that the interpupillary distance can be fitted for each observer (Fig. 3D). Adjustment of the interpupillary distance is essential to achieve binocular depth perception. In addition, on most colposcopes one or both eyepieces have diopter settings to adjust focus for each eye individually. Plastic hoods on the eyepieces reduce ambient light.
VIDEOCOLPOSCOPY
It is useful to have the colposcope attached to a small video camera and monitor. This requires a beam-splitter to send the image to both the eyepiece and the camera, a videoscreen, and a computer with appropriate software for image capture and data management. With such a setup, it is possible to record the examination, to use the monitor for teaching, and to demonstrate the findings to the patient. Digital or film cameras can also be attached to some colposcopes to generate still images.
Other equipment
An examination table that is adjustable in height is ideal in order to align the patient, the colposcope, and the examiner. If an adjustable examination table is not available, an adjustable chair is the next best option. Ideally the chair and exam table height are optimally aligned to visualize and illuminate the cervix while allowing comfortable examiner posture.
The colposcopist must have access to a wide range of speculum shapes and sizes. In some cases, vaginal sidewall retractors may be necessary to visualize the cervix. A condom placed over the speculum can also sometimes achieve the goal of retracting the vaginal sidewalls.
Colposcopy also requires an investment in high quality instruments:
- An endocervical speculum is useful for visualizing the transformation zone when it extends into the canal. It has narrow blades that can be inserted into the endocervical canal and retracted in order to widen the diameter of the external os (Figs. 2F and 4A). It can cause extreme cramping if widened excessively and should be used advisedly.
- Biopsy forceps of several types are available (e.g., Tischler, Burke, Eppindorfer, Kevorkian). The instrument should have sharp cutting edges (including straight- or toothed-edge versions) rather than one cutting edge and one smooth edge. Instruments should be handled with care to avoid misalignment and dulling of the cutting surfaces. Instruments need to be sterilized between uses. Heat sterilization techniques can result in dullness. Instruments should be sent for sharpening periodically. Examples of large and small Tischler biopsy forceps are shown in Figure 4B and 4C.
- An endocervical curette should have a sharp straight cutting edge that is applied against the endocervical canal. A depression in the handle indicates the orientation of the cutting edge (Fig. 4D), allowing for effective application of pressure. The curette may contain a “basket” below the cutting edge to collect the specimen (Fig. 4D).
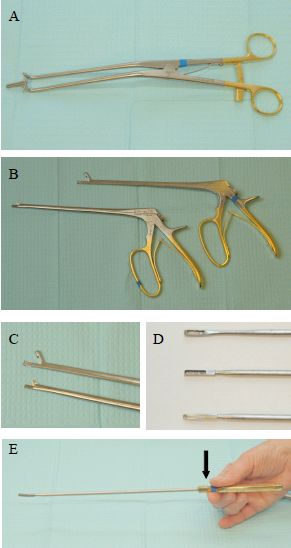
Fig. 4. (A) Endocervical speculum is useful for visualizing the SCJ in cases where the TZ extends into the cervical canal. (B) and (C) Biopsy forceps come in different sizes and should have grasping surfaces on one or both jaws. Shown here are normal and small Tischler biopsy forceps. (D) Endocervical curettes may contain a basket to trap tissue or may be empty. (E) The handle of an endocervical curette may have an indentation in the handle that is aligned with the sharp edge of the curette.
Supplies
The colposcopy room must be supplied with the following disposable items. A typical set-up for colposcopy is shown in Figure 5.
- Single-use jars of 3–5% acetic acid. Kitchen vinegar is 5% acetic acid. It can cause stinging especially when applied to the vulva. Diluted vinegar (3% acetic acid) is less irritating but solutions weaker than 3% are not effective at illuminating abnormal areas.
- Single-use jars of Lugol’s solution. Lugol’s is a strong iodine solution that stains normal epithelium dark brown, useful for delineating normal from abnormal epithelium, for defining the borders of a lesion, and for finding vaginal lesions.
- Silver nitrate sticks. These provide a useful cautery agent that is applied with pressure to bleeding biopsy sites.
- Single-use jars of Monsel’s solution. Monsel’s is a chemical cautery agent made of ferric subsulphate. It should have a consistency of mustard, and is applied to bleeding sites by transferring it on a cotton swab. It is caustic, more effective than silver nitrate, and stings, hence it is important to apply it focally to the bleeding site and to avoid vaginal sidewalls and external genitalia. It is essential to have at hand when performing cervical biopsies in pregnancy.
- Large cotton swabs. Large swabs are useful for applying solutions to the cervix, for manipulating the cervix and vaginal fornices to optimize visualization, and for applying pressure for hemostasis.
- Small cotton swabs. Small swabs are useful for manipulating the cervical os to optimize visualization of the transformation zone, for applying pressure for hemostasis, for applying Monsel’s solution.
- Formalin bottles. Biopsy and curettage samples need to be fixed immediately by placing in formalin. Due to the small size of the samples, small specimen containers are advisable.
- Spatula and endocervical brushes if cervical cytology is to be collected at the time of colposcopy.

Fig. 5. Typical side tray used for colposcopy: (from right to left) spatula and brush if cytology is to be performed, 5% acetic acid, large swabs, Lugol’s solution, small swabs, formalin, silver nitrate sticks and Monsel’s solution.
Method
After introduction of a bivalve speculum, the colposcope is brought into position and focused on the cervix. If there is excess mucus present, it can be removed with a swab dipped in saline. The cervix should then be carefully examined prior to application of acetic acid. After thorough inspection, 3–5% acetic acid is applied to the cervix with a saturated large swab, using pressure rather than rubbing to avoid denuding the surface epithelium. It takes 30–60 seconds for acetowhite changes to occur. Repeated application of acetic acid during the course of the examination is necessary as the acetowhite changes can fade within 1–2 minutes after application.
The colposcope should initially be set at the lowest magnification and used to determine whether the entire TZ can be visualized, i.e., whether the examination is satisfactory. Two elements are necessary for the examination to be satisfactory. First, the entire TZ must be seen. This means that 360° of columnar epithelium and 360° of normal squamous epithelium must be seen, as well as all of the area between them. Second, if a lesion is present, it must be seen in its entirety. Lesions that extend up the canal out of sight have not been seen completely, i.e., the exam is unsatisfactory. The endocervical canal can be visualized with the assistance of the endocervical speculum or small cotton swabs used to retract the edges of the external os.
The colposcopist then needs to determine whether the transformation zone is normal or atypical. This requires assessment under higher magnification. Any areas of acetowhite epithelium should be examined using the criteria described above and the most abnormal areas should be sampled with a biopsy. Injection of anesthetic is unnecessary for cervical biopsy due to low density of nerve endings sensing pain. Sharp instruments reduce the pain associated with biopsies; hence it is important to maintain the equipment in good condition and to send for sharpening when necessary. The biopsy instrument should be placed directly over the abnormal area. For a large lesion, the biopsy should be taken closest to the squamocolumnar junction, since the highest grade of disease is usually the most proximal. Depending on the extent and appearance of the lesion(s), several biopsies may be necessary. Biopsy samples are typically 3–5 mm3. The biopsy sample should be placed immediately in formalin and labeled with the patient identifiers and location. It is always necessary to take a sample of the epithelium and underlying stroma to be able to accurately grade the dysplasia and to rule out invasive cancer. Pressure with a large swab or cautery with silver nitrate or Monsel’s solution can be used to control bleeding after biopsy.
In cases in which the colposcopy is unsatisfactory, an endocervical curettage (ECC) is usually performed. This technique uses a small curette to obtain a circumferential scraping of the endocervical epithelium. Tissue captured on the curette should be collected by rinsing the instrument directly into formalin (avoid the use of telfa as loss of tissue due to sticking to the telfa may lead to an insufficient sample). Additional tissue should be recovered from the canal with an endocervical brush passed into the canal and rotated at least twice, then scraped off the brush into the formalin bottle. In cases in which a stenotic os does not admit the curette, a suitable sample may be obtained with aggressive use of a series of endocervical brushes. ECC commonly causes pain and/or cramping.
After colposcopy, patients should be advised that they may experience spotting but that heavy bleeding is unusual.
PATIENT MANAGEMENT AFTER INITIAL COLPOSCOPY
ACOG1 and ASCCP2 guidelines address the most common clinical scenarios. Table 4 outlines management strategies after initial colposcopy generally based on current ACOG and ASCCP guidelines. Readers may wish to consult actual guidelines for a broader discussion. Of course, patients can be managed individually based on clinical judgment.
Table 4. Management strategies after initial colposcopy
| Referral cytology (cytology prior to initial colposcopy) | Findings at initial colposcopy | ||
No CIN
| Biopsy-proven CIN I | Biopsy-proven CIN 2 or 3 | |
| ASC-US once | Repeat cytology in 12 months | Treat as per ACOG and ASCCP guidelines
| |
| ASC-US twice (unknown HPV status) ASC-US, positive high-risk HPV Atypical squamous cells, cannot exclude HSIL (ASC-H) Low- grade SIL (LSIL) | Repeat cytology at 6 and 12 months: After 2 normal cytology tests, resume routine screening
| ||
High-grade SIL (HSIL)
| Satisfactory colposcopy. ECC and vagina are normal: review referral cytology. If HSIL interpretation upheld, may perform either DEP (nonpregnant women only) or colposcopy and cytology at 6 and 12 months
| Unsatisfactory colposcopy. Perform DEP (nonpregnant women only)
| |
Atypical glandular cells (AGC)
| Repeat cytology at 6, 12, 18, and 24 months. Repeat colposcopy if ASC-US+. After 4 normal cytology tests, resume routine screening. If AGC recurs, perform cone biopsy. (ASCCP guidelines support HPV-based management; see guidelines for full discussion) | ||
| Adenocarcinoma in situ, cancer | Cone biopsy | ||
ASC, atypical squamous cells; CIN, cervical intraepithelial neoplasia; SIL, squamous intraepithelial lesion.
HSIL+ indicates HSIL, AGC, adenocarcinoma in situ and/or cancer.
ASC-US+ indicates ASC-US, ASC-H, LSIL and/or HSIL+.
DEP indicates diagnostic excisional procedure (e.g., cone biopsy, loop excision).
SPECIAL CONSIDERATIONS: PREGNANCY
The goal of colposcopy in pregnancy is to rule out invasive cancer. Biopsies of suspicious lesions may be obtained, but bleeding may be more brisk than in the nonpregnant state. The examiner is advised to hold a cotton-tipped swab next to the end of the biopsy instrument and place the swab immediately into the biopsy crater. Another swab containing Monsel's solution can then be exchanged in the biopsy location. Using this technique, blood loss is minimized. The colposcopist must have the ability to suture the biopsy site if necessary.
If high-grade CIN is diagnosed, it should not be treated during pregnancy; patients should be counseled that the risk of developing cancer is low. ASCCP guidelines state that repeat colposcopic and cytologic examination to rule out progression to invasive cancer is acceptable but should not be performed more frequently than every 12 weeks. Repeat biopsy should be performed if invasive cancer is suspected. Alternatively, colposcopy may be deferred to 6 weeks postpartum after initial colposcopy. High-grade CIN is not an indication for a cesarean section.
VAGINA: VAGINAL INTRAEPITHELIAL NEOPLASIA
As with CIN, vaginal intraepithelial neoplasia (VAIN) is also the result of HPV infection. VAIN can be diagnosed by means of colposcopically directed biopsy, but the colposcopic appearance of VAIN is slightly different from that of CIN. Lesions in the vagina rarely show mosaic changes. Rather, acetowhite epithelium or punctation are more commonly seen. Abnormal cytology in women who have undergone hysterectomy rarely indicates the presence of significant intraepithelial neoplasia; invasive cancer of the vagina is the single rarest genital cancer in women, even rarer than primary fallopian tube carcinoma. More often, in premenopausal women they indicate only HPV infection and in postmenopausal women epithelial atrophy. However, if cytology suggests the presence of a high-grade lesion, colposcopy is indicated. Acetic acid can be used in the vagina in the same manner as on the cervix. Lugol's solution can be useful when attempting to identify a vaginal lesion. Only glycogenated epithelium will stain with iodine.
VULVA: VULVAR INTRAEPITHELIAL NEOPLASIA
The colposcope can be of use in the diagnosis and treatment of vulvar intraepithelial neoplasia (VIN). Because the vulvar skin is keratinized, acetic acid only slowly produces acetowhite changes. Three to five per cent acetic acid can be used on the vulva. It is necessary to allow at least one minute between application and observation. Soaking a gauze sponge in acetic acid and holding it against the vulva for a minute is an effective method for applying acetic acid. Acetowhite changes may be associated with VIN, HPV, and hyperkeratotic areas due to trauma, scratching, or pressure. Mosaicism and punctation are rarely seen on the vulva. However, if abnormal vascular patterns are present, biopsy is always indicated.
Vulvar biopsy may be safely accomplished in the office. A local anesthetic, such as lidocaine, should be injected into the epithelium with a 30-gauge needle and a specimen including both epithelium and stroma obtained. Disposable 3 mm Keys biopsy instruments are useful on the exterior hair-bearing surfaces. On the labia minora and vestibular area, a cervical biopsy punch can be used to obtain a biopsy. Usually the application of silver nitrate to the base of vulvar biopsy sites is all that is necessary to stop bleeding. Sutures are rarely necessary.
VIN lesions may have other appearances besides acetowhitening. Many VIN 3 lesions are darkly pigmented. A biopsy should be performed on any lesion that shows change in pigmentation particularly areas with irregular edges and contours. For more information, the reader is referred to the chapter on chapter on Vulvar intraepithelial neoplasia.
ACKNOWLEDGMENTS
We acknowledge the contributions of Drs Kenneth L. Noller and Arnold L. Wagner Jr to earlier versions of this chapter.
REFERENCES
Belinson J, Qiao YL, Pretorius R et al. Shanxi Province Cervical Cancer Screening Study: a cross-sectional comparative trial of multiple techniques to detect cervical neoplasia. Gynecol Oncol 2001;83:439-44. |
|
Cantor SB, Cardenas-Turanzas M, Cox DD et al. Accuracy of colposcopy in the diagnostic setting compared with the screening setting. Obstet Gynecol 2008;111:7-14. |
|
Pudney J, Quayle AJ, Anderson DJ. Immunological microenvironments in the human vagina and cervix: mediators of cellular immunity are concentrated in the cervical transformation zone. Biol Reprod 2005;73:1253-63. |
|
Stafl A. Colposcopy. Clin Obstet Gynecol 1975;18:195-213. |
|
Coppleson M. Colposcopic features of papillomaviral infection and premalignancy in the female lower genital tract. Obstet Gynecol Clin North Am 1987;14:471-94. |
|
Reid R, Scalzi P. Genital warts and cervical cancer. VII. An improved colposcopic index for differentiating benign papillomaviral infections from high-grade cervical intraepithelial neoplasia. Am J Obstet Gynecol 1985;153:611-8. |
|
Guidi AJ, Abu-Jawdeh G, Berse B et al. Vascular permeability factor (vascular endothelial growth factor) expression and angiogenesis in cervical neoplasia. J Natl Cancer Inst 1995;87:1237-45. |
|
Sillman F, Boyce J, Fruchter R. The significance of atypical vessels and neovascularization in cervical neoplasia. Am J Obstet Gynecol 1981;139:154-9. |