Female Circumcision
Authors
INTRODUCTION
“He who is eight days old among you shall be circumcised, every male child in your generations, ...must be circumcised, and My covenant shall be in your flesh for an everlasting covenant. And the uncircumcised male child, who is not circumcised in the flesh of his foreskin, that person shall be cut off from his people; he has broken My covenant.”… Abraham was 99 years old when he was circumcised in the flesh of his foreskin – Genesis 17:12–14, 24 (King James Versionof Bible).
DEFINITIONS
Circumcision is derived from the Latin word circumcisio, which means to cut around or to excise in a circumferential manner, or “circular abscission of the prepuce or foreskin.”1 This definition does not translate easily to the female genitals, as the clitoral prepuce is not a circular tissue, nor is it the sole tissue removed during most female circumcision (FC) procedures.
Female circumcision and female genital mutilation are both broad, inexact terms, and they do not describe what tissues have been cut or excised. Table 1 lists the common terms used to describe different FC types in reference to the anatomic defects created.2, 3, 4
Table 1. Circumcision nomenclature
Degree | Anatomic Change | Common Name |
I | Clitoral prepuce excised or cut | Sunna |
II | Clitoral prepuce and end of clitoris excised, possibly anterior edges of labia minora removed | Excision |
III | Clitoral prepuce, clitoral tissue, and all of labia minora excised, followed by infibulation of the raw edges to create a vulvar skin/scar diaphragm covering the urethral meatus | Intermediate Pharaonic – excision and infibulation |
IV | All clitoral and labia minora tissue excised, inner part of labia majora scraped off, followed by infibulation of the raw edges to leave only a pinpoint opening in the perineum through which all urine and menses must pass | Pharaonic |
(Adapted from Ruminjo J: Circumcision in women. East Afr Med J 9:477, 1992; Dirie MA, Lindmark G: The risk of medical complication after female circumcision. East Afr Med J 9:479, 1992; Fourcroy JL: L'eternal couteau: Review of female circumcision. Urology 22:458, 1983; and Toubia N: Female circumcision as a public health issue. N Engl J Med 331:712, 1994)
The type I procedure, colloquially known as Sunna, is considered the mildest form of FC, with only the prepuce of the clitoris being cut or excised. Some use the word Sunna to indicate a burning or a small cut of the prepuce, whereas other references incorrectly term a clitoridectomy a Sunna procedure.3, 5, 6, 7 The type II and type III procedures have considerable overlap in the anatomy affected, but generally these terms indicate cutting and excision of the clitoris and labia minora. Suture is sometimes used to approximate the cut labial edges. Type IV, or Pharaonic circumcision, connotes the most extreme form of FC, whereby the tissues of the clitoris, labia minora, and labia majora are excised and the edges infibulated, buckled, or “clasped together” with thorns, threads, paste, or suture, and then the girl's thighs are bound together to allow union of the raw surfaces.1, 4 This procedure creates a single pinhole opening in the posterior perineum through which urine and menses must pass because the urethral meatus and the vestibule of the vulva have become hidden by a diaphragm of vulvar skin and scar tissue.3
In the past, vaginal introcision was performed by some aboriginal and African tribes, whereby the vaginal wall was cut in addition to the vulvar procedure.8, 9 Currently there are no reported forms of FC that involve cuts into the vagina, and it is safe to assume that most sequelae of FC are related to changes of the vulva and distal to the hymenal tags. Of course, vaginal damage could result from slips of the excising instrument or ascending infection.
Few studies have found a correlation between the procedure that the woman believes she had received and what is actually found on clinical examination. For example, a mother may request a Sunna FC for her daughter, but the provider instead performs an intermediate infibulation (type III), since that is what she knows as a Sunna circumcision. Later this grown-up woman believes she had a Sunna FC as a child.10 Another example is a Nigerian study of women who reported having undergone type I circumcisions as infants; examinations of these women revealed that 58% of those who reported a history of circumcision had no evidence of a genital abnormality or scar.11
Many FC procedures are done under unsanitary conditions by local nonmedical personnel using no or only local anesthesia, and with the girls only partly restrained.4, 12, 13 These conditions combine to create variable results, making the outcomes and complications of a particular type of FC procedure difficult to predict. Consequently, the best advice is to perform a careful anatomic survey of each patient and detailed questioning of ongoing symptoms, rather than assuming the presence of anatomic findings based on the FC term reported by the patient.
HISTORY
Circumcision is an ancient custom, as evidenced by carvings of a priest performing male circumcision on the Tomb of Ankmahor at Saggorn from 2400BC.8 Egyptians even had a god of circumcision. FC is documented in two forms: a simple clitoridectomy for the upper classes and infibulation for the slaves.9, 12, 14 Romans placed rings through the vulvar lips of female slaves to infibulate (“clasp together”) the vulva, thus regulating copulation.12, 14 Thus, the practice of circumcision predates the beginning of Islam with the birth of Mohammed in about AD570.15
Throughout history, sacrificial removal or marking of body parts was associated with rites of passage into adulthood. Not all extreme forms of genital circumcision involve females. As late as 1983 in some aboriginal groups, a procedure known as subincision of the penis was used as a puberty rite of inclusion into the tribe's power structure.8 Subincision is a urethrotomy whereby the penile urethra is opened to create a large hypospadias.16 Male circumcision may have been developed in desert areas of Australia to prevent balanitis or inflammation of the foreskin due to dusty conditions and lack of water, and the subincision may have been used to prevent urethral strictures.17 The original reasons for circumcision rites are often difficult to ascertain because often they predate written languages or are part of secret societies, or because the reasons for the ritual change.4, 12, 16
In England and the United States during the 19th century clitoridectomies and even infibulations were performed to treat masturbation, lesbian tendencies, hysteria, and sometimes medical conditions such as dysmenorrhea.10, 12 In Roman athletes, infibulation of the penis, with a ring through the foreskin, made public erection painful and coitus impossible.10, 14 This principle was practiced with wire in the Victorian era and even by Kellogg's followers as a means of “interrupting” the practice of masturbation.18
PREVALENCE
Circumcision is practiced in more than 30 countries worldwide, but predominantly in Africa, which has prevalence rates ranging from 5% to 95% of the population in some countries.2, 6, 12 An estimated 80–100 million women living in Africa are circumcised. In Egypt, circumcision is legal if performed by a physician, and an estimated 3600 girls are circumcised daily.19 Countries where greater than 80% of the female population are subjected to FC operations include Ethiopia, Eritrea, Somalia, Sudan, and Sierra Leone.6, 12, 20 Both Christian and Muslim communities practice FC in these geographic areas. This strengthens the argument that in East Africa, the practice of FC has a Pharaonic rather than Islamic origin that spread from the the Nile Valley to the Horn of Africa through Central Africa, and west to Nigeria.20 FC also occurs sporadically in Malaysia, Indonesia, Australia, Peru, and in the past in areas of Central Mexico.10, 12 North America has no record of an indigenous custom of circumcision.9
FC is performed at ages ranging from 8 days old in Ethiopia, 6 years in Somalia, puberty in Sierra Leone, shortly after marriage in the Masai of Kenya, during pregnancy in Nigeria, and after childbearing in Guinea.4, 12 The Gikuyu, who use circumcision as part of a rite of passage from childhood to adulthood, consider it the most important custom for preserving their social order.21
REASONS FOR THE PRACTICE OF FEMALE CIRCUMCISION
It was stated that, “behind circumcision lies the belief that, by removing parts of girls' external genital organs, sexual desire is minimized. This permits a female … to protect her virginity, and therefore her honor, with greater ease.”22 Indeed, the exhibition of her intact circumcision scar to her mother as proof of her intact virginity is used by Aman in her story about growing up in Somalia.5 Most studies find that the following are given as reasons for FC: tradition, culture, religion, to be married, pleasure for husband, chastity before marriage, family honor, and cleanliness.13, 23, 24, 25, 26, 27
A Russian sect uses circumcision to ensure a state of perpetual virginity to adhere to the following Biblical quotation: “… there be eunuchs, which have made themselves eunuchs for the kingdom of heaven's sake” (Matthew 19:12, KJV).10 The critical role of religion in maintaining the practice is best illustrated by the Islamic position. The Quran does not mention female circumcision but the Hadith, or Oral Tradition, has several quotations attributed to Mohammed: “Circumcision is an ordinance in men and an embellishment in women,” and “… reduce but do not destroy, this is enjoyable to the woman and preferable to the man.”13, 28 Sunna means “to follow the tradition of the prophet,” hence the Sunna FC is considered a “good tradition” in some Muslim sects.28 Yet in most Islamic countries, FC is not practiced.13
A recent survey of university students in Khartoum found that many educated men were now against excision and infibulation in part because of reduced sexual satisfaction.23 For some women the attainment of the “smooth infibulated vulvar scar” is seen as aesthetic and evidence of their bravery.5, 9, 10, 12 They are able to “avoid the unfeminine sound of urination,” and frequently they shave the pubic hair to enhance this appearance of smoothness.7 The fear of the Hottentot Apron or hypertrophied labia keeps some mothers promoting the removal of labia in their daughters to prevent lengthening of the labia.5, 10, 12, 14, 24 Some cosmetic labioplasties in adolescents are performed in the United States.29, 30
IMMEDIATE COMPLICATIONS
There are no prospective or systematic reports on the outcomes of FC, since it is typically an illegal and undocumented procedure. Most complications are those that are remembered by the woman or her family. Deaths are not always reported for fear of retribution against the practitioner. Most data are derived from interviews of survivors or from hospital admissions. Given these limitations, Table 2 lists the percentage of immediate complications according to the type of procedure reported by the women interviewed.3, 31
Table 2. Percentage of immediate complications of female circumcision*
Complications | Sunna El Dareer31 | Pharaonic El Dareer31 | Pharaonic Dirie3 |
Hemorrhage | 6 | 6 | 18 |
Transfusion |
|
| 0.6 |
Shock |
| 1 | 2 |
Fever |
| 4 |
|
Septicemia |
|
| 1.4 |
Local infection |
| 5 | 15 |
Dysuria |
| 6 |
|
Urinary retention | 2 | 3 | 3 |
Total | 8% | 27% | 38% |
*Adapted from El Dareer's31 early 1980s interviews with 3210 Sudanese women and 1545 Sudanese men. Similar outcomes from Dirie and Lindmark's3 interviews with 290 Somalian women in 1978 are also listed.
(Adapted from El Dareer A: Complications of female circumcision in the Sudan. Trop Doct 13:131, 1983; and Dirie MA, Lindmark G: The risk of medical complication after female circumcision. East Afr Med J 9:477, 1992)
As with any genitourinary surgical operation, the most common problems of FC are pain, bleeding, dysuria, urinary retention, wound infection, and delayed healing. Acute hemorrhage can occur if the vessels are not ligated, resulting in shock, transfusion, or death.3, 6 Infection leading to sepsis, gangrene, or tetanus can be life-threatening.12, 32 Although the frequency of fatal complications is difficult to estimate, in Sudan, where type IV FCs are performed, only 23% remembered having any immediate complications, and no deaths were mentioned.31
LONG-TERM COMPLICATIONS
The degree of long-term complications is related to the type of FC performed (Table 3). The most obvious complication of FC is malformation of external genitalia. The urethral meatus is hidden by this vulvar scar, which acts as a diaphragm over the introitus, which in type IV FCs may not allow entrance of even a finger. In some cases, the routine bimanual pelvic or cervical examination may be conducted only with an index finger, or in some cases only by rectal examination. Speculum examination or visualization of the cervix may not be possible in the Pharaonic virgin.6, 33
Table 3. Percentage of delayed complications of female circumcision*
Complications | Sunna El Dareer31 | Pharaonic El Dareer31 | Pharaonic Dirie3 |
Keloid |
| 0.3 |
|
Scar abscess |
| 4 |
|
Inclusion cyst |
| 0.6 | 12 |
Recurrent UTI | 8 | 8 |
|
Chronic PID | 6 | 8 |
|
Apareunia |
| 9 | 13 |
Dyspareunia |
| 2 |
|
Dysmenorrhea |
| 2 | 14 |
Hematocolpos |
|
| 3 |
Total | 14% | 34% | 42% |
*Adapted from El Dareer's31 early 1980s interviews with 3210 Sudanese women and 1545 Sudanese men. Similar outcomes from Dirie and Lindmark's3 interviews with 290 Somalian women in 1978 are also listed.
PID, pelvic inflammatory disease; UTI, urinary tract infection.
(Adapted from El Dareer A: Complications of female circumcision in the Sudan. Trop Doct 13:131, 1983; and Dirie MA, Lindmark G: The risk of medical complication after female circumcision. East Afr Med J 9:477, 1993)
Recurrent urinary tract infections are possibly related to type IV FC, but validation is difficult because clean-catch specimens are impossible to obtain in most infibulated women. These women void into the vagina behind the diaphragm. Thus, voided urine specimens contain vaginal material, and cystitis is difficult to distinguish from contamination. Most studies do not report cultures from catheterized specimens for comparison.3, 4, 31
Premenarchal children are more likely to present with urologic rather than gynecologic complaints. Complaints of pain, straining, dribbling incontinence, and poor flow prior to deinfibulation procedures are documented.32 Only two cases of urethral stricture were reported in this series of 55 children; presumably, routine intravenous pyelogram and cystoscopy were normal. Aziz7 reported two urethral strictures in his larger series of 7505 Sudanese women.
Epidermal inclusion cysts are commonly found in the infibulation scar.3, 7, 31 These cysts result from the invagination of epithelial tissues; thus keratin is shed into a closed space. Occasionally, the cysts become infected.7, 33
The problems of circumcision at menarche are considerable, as 2–4% of women will require deinfibulation to drain a vulvovaginal hematocolpos.3, 7, 31 Most studies report deinfibulation operations occurring in the operating room under spinal or general anesthesia;7, 32, 33 however, our clinic performs approximately four deinfibulations per month with the following technique. A blunt probe is inserted into the pinhole opening under local anesthesia, and a longitudinal scalpel incision is made along the probe following the linear infibulation scar. The urethral meatus at the apex of the vestibule must be avoided as the incision is extended over the clitoral bed.32, 33, 34 Interrupted sutures can be used for hemostasis but are often not necessary. The patient is instructed in hygiene, sitz baths, and mechanical separation of the edges to prevent reagglutination.
Although apareunia is often the cause of infertility, pregnancy is possible in women with pinhole openings.7, 34, 35 Full penetration occurred in women with Sunna FC in 3–7 days; with Pharaonic FC, consummation took as much as 2–12 weeks.26 Of 119 married infibulated women, 27 required instrument deinfibulation.3 Deinfibulation is viewed as shameful because it indicates that the husband was incapable of penetration, and some couples will continue to attempt intercourse, resulting in penile injuries, anal intercourse, or surgery at home.3, 6, 10, 12
Dysmenorrhea is a common complaint that often resolves with the use of nonsteroidal anti-inflammatory drugs. After consummation of marriage and childbearing, both urinary and menstrual complaints typically diminish.7, 10
Sexual dysfunction must occur as a result of FC procedures, but questions on orgasm and pleasure are rare. However, detailed interviews explicitly describing the woman's sensation and experiences with orgasm report what appears to be sustained sexual satisfaction (i.e., orgasm) for some women, despite infibulation.10
Chronic pelvic infection is often listed as a complication of FC, but there is no objective substantiation, and since most complaints are self-reported during an interview, vulvovaginitis may be confused with pelvic infection.
The frequency of FC complications requiring surgery in 119 cases included excision of an inclusion cyst in 55%, drainage of a scar abscess in 9%, and vaginal stenosis or deinfibulation procedures for complications including vulvovaginal hematocolpos in 36%.34
OBSTETRIC IMPLICATIONS
Death due to a pregnancy-related cause during reproductive life occurs in 1 in 21 women in Africa (compared to the 1 in 15,000 lifetime maternal mortality in the United States).20 Little is known regarding the precise role of infibulation in maternal mortality, but infibulation does contribute to obstetric difficulties.
A British clinic performed antepartum deinfibulation to allow pelvic examinations and delivery without anterior episiotomy.33 This is not common practice, and even when offered, most patients refuse and want to wait until delivery for the deinfibulation. This makes pelvic examination difficult, and obstetric dating often must be augmented with ultrasound studies. Deinfibulation is recommended in the first trimester so that digital examinations can be used to monitor cervical dilation during labor, eliminating the need for rectal examinations to monitor cervical dilation.
In a comparison of the obstetric outcomes of infibulated women to noncircumcised women in a Saudi Arabia hospital, infibulation did not appear to affect the first stage of labor because it did not interfere with uterine activity or cervical dilation.36 The second stage of labor was significantly prolonged in infibulated women because the infant's head was not easily visible as a result of the obstructing scar at the introitus, which created delays in the cutting of the necessary anterior episiotomy. Infibulation had no effect on the rate of instrumented delivery.33, 36
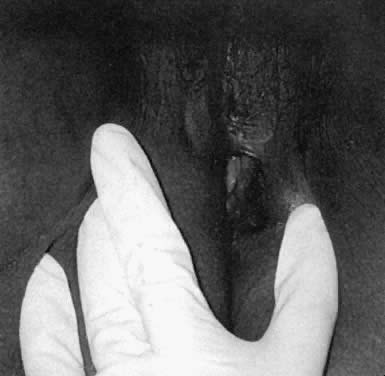
Infibulated women had a significantly higher rate of hemorrhage secondary to both an anterior episiotomy and the use of the mediolateral episiotomy to prevent fourth-degree extensions.36, 37 The unyielding scar tends to cause a greater degree of perineal tearing. A timely anterior episiotomy by trained personnel appears to avoid obstructed labors, and hence tissue necrosis, vesicovaginal and rectovaginal fistulas, uterine rupture, and infant trauma.36, 38 In a recent report on female genital mutilation, 46% of multiparas delivered with intact perinea, and more than 90% of primiparas delivered vaginally (Fig. 1).33
|
A word of caution is necessary regarding cesarean section for recent African immigrants. The surgeon may need to hold extensive discussions with the patient and her family about the need for the surgery. For example, the woman may wrongly think that she is being advised to have a cesarean section because the physician is hesitant to perform an episiotomy on the circumcision scar, rather than the multitude of reasons for which cesarean sections are performed in developed countries. The concept of surgical intervention for the infant's well-being is unfamiliar to many of these women. Informed consent may also be a foreign concept. It is often wise for the obstetrician to discuss the many reasons for a cesarean section before labor ensues, as well as the implications of not performing a cesarean section, so that he or she may develop an understanding of the particular wishes of the patient and her family before an emergent need arises for operative consent.
Before cesarean section or forceps delivery, placement of a urinary catheter is required to reduce complications. Catheter insertion can be performed similar to intrauterine pressure catheter introduction, using palpation and blind guidance of the catheter into the urethra. If necessary, early anterior episiotomy can be performed.
To perform an anterior episiotomy, a finger is introduced into the introitus and the vulvar skin diaphragm is elevated and cut with scissors or a scalpel using the finger to protect the underlying tissue, particularly the urethral meatus.38, 39 This widens the introitus and exposes the urethral opening. The cut should be performed only when the head is crowning on the perineum to stretch the tissues. However, the cut should be made before tears begin because the scar has little elasticity, and extensions are common if the head is not well controlled. For additional room, a routine posterior episiotomy can be made. A mediolateral episiotomy also should be considered, since this is often the practice in Africa to avoid rectal tears. Despite counseling about the risks of excess bleeding, pain, and extensions, African women in our clinic tend to insist on a mediolateral cut rather than a posterior midline episiotomy.
After delivery, if the woman chooses to leave the scar tissue open, the two edges of the anterior episiotomy incision can be oversewn with a loose running or interrupted absorbable suture, if needed for hemostasis. The woman is instructed on twice-daily sitz baths and on keeping the scar edges open with mechanical separation with an open gauze during washing. Topical application of estrogen can be applied in lactating women. If the woman chooses to have the edges of her circumcision scar reapproximated, then any bleeding edges can be sutured together with a single subcuticular layer of running absorbable suture. A continuous suture minimizes the development of a fistula in the linear vulvar scar due to the pressure of urination. Even with reapproximation, the introital opening is always larger than it was before delivery because the anterior episiotomy is not cut until after pushing and stretching of the perineum.
Repair of an anterior episiotomy at the time of delivery is illegal in the United Kingdom because it is considered a reinfibulation. Toubia6 described circular stitches over the edges of the cut labia majora scar, but did not discuss or illustrate in the diagrams the point that the scar edges are flaps, rather than flat surfaces. Because no tissue is excised or removed at delivery, oversewing the edges leaves two flaps of scar tissue that are not labia. The rate of spontaneous reformation of the midline scar is high when the woman does not take precautions to avoid reagglutination. The practice of nonobstetric reinfibulation between deliveries or to hide the loss of virginity is not advised, as it will create additional scar tissue and potential complications.10, 20, 25
Since many women with infibulation FC are Muslim, it is helpful to be familiar with Islamic requirements such as Ramadan. This is a time of daily fasting from sunrise to sunset for the entire ninth month of the Islamic calendar.15, 28 Vaginal examinations are forbidden when fasting. Pregnant women are excluded from required fasts, but they will often fast to attain the state of purity. A common request is for all care givers, including physicians, to be female, but it is important to know that this is not an Islamic law; women can be treated by a “trustworthy” male physician when there is no female physician available and the case cannot be delayed.28
ERADICATION
There are current laws forbidding FC in some European countries.6 In the United States, Senator Harry Reid passed a senate amendment to title 18, of the United States Code titled the “Federal Prohibition of Female Genital Mutilation Act of 1996.” Section 116 (a) states: “Whoever knowingly circumcises, excises, or infibulates the whole or any part of the labia majora or labia minora or clitoris of another person who has not attained the age of 18 years shall be fined under this title or imprisoned” (Congressional press release). Both the 1992 International Federation of Gynaecology and Obstetrics and the 1993 World Health Organization have published statements condemning FC.6, 40 The American Medical Association and the American College of Obstetricians and Gynecologists also released position statements against FC in 1995,40, 41 although circumcision of male infants is routinely practiced in the United States.42
Historically, laws forbidding circumcision have not reduced its practice. In 1945, when British law forbade Pharaonic FC, midwives developed FC types II and III, calling them Sunna FC procedures.10, 13 Many believe the solutions and laws need to come from the communities themselves.12, 14 The imposition of laws may serve only to harden sentiment for the practice of FC and perpetuate FC as part of the cultural identity.43, 44
Islamic teaching may be reformed to advocate Sunna rather than Pharaonic FC procedures, but unfortunately there is no consensus on the precise definition of Sunna.44 Until providers of FC operations and family are taught to accept the true Sunna or type I FC, it is not clear what reform will accomplish. The belief in the need to perform FC is deep rooted, as illustrated by a Sudanese woman who described FC as “a bad practice,” but then stated that “she does not dare to leave her daughter entirely uncut. She must have some sort of circumcision … or people will look down on her.”10 This sentiment is also reflected by the following statement made by a Somali woman: “You cannot live in Somali and not be circumcised.”43
REFERENCES
Dorland's Medical Dictionary, 27th ed. Philadelphia, WB Saunders, 1988 |
|
Ruminjo J: Circumcision in women. East Afr Med J 9: 477, 1992 |
|
Dirie MA, Lindmark G: The risk of medical complication after female circumcision. East Afr Med J 9: 479, 1992 |
|
Fourcroy JL: L'eternal couteau: Review of female circumcision. Urology 22: 458, 1983 |
|
Barnes VL: Aman, The Story of a Somali Girl [biography as told to Virginia Lee Barnes and Janice Boddy]. New York, Random House, 1994 |
|
Toubia N: Female circumcision as a public health issue. N Engl J Med 331: 712, 1994 |
|
Aziz FA: Gynecologic and Obstetric complications of female circumcision. Int J Gynaecol Obstet 17: 560, 1980 |
|
Montagu MFA: Ritual mutilation among primitive peoples. Ciba Symp 8: 421, 1946 |
|
Worsley A: Infibulation and female circumcision: A study of a little known custom. J Obstet Gynaecol Br Emp 45: 686, 1938 |
|
Lightfoot -Klein H: Prisoners of Ritual: An odyssey into Female Genital Circumcision in Africa. New York, Harrington Park Press, 1989 |
|
Odujinrin OMT, Akitoye CO, Oyediran MA: A study on female circumcision in Nigeria. West Afr J Med 8: 183, 1989 |
|
Koso -Thomas O: The Circumcision of Women: A Strategy for Eradication. London, Zed Press, 1987 |
|
El Dareer A: Woman, Why Do You Weep? London, Zed Press, 1982 |
|
Cutner LP: Female genital mutilation. Obstet Gynecol Surv 40: 437, 1985 |
|
Anderson N: The World's Religions, 4th ed. Grand Rapids, MI, William B. Erdmans, 1997 |
|
Pounder DJ: Ritual mutilation subincision of the penis among Australian aborigines. Am J Forensic Med Pathol 4: 227, 1983 |
|
Morrison J: The origins of the practices of circumcision and subincision among the Australian aborigines. Med J Aust January, p 125, 1967 |
|
Money J: Honk if you masturbate: Safe sex in the era of AIDS. Trends Health Care Law Ethics 10: 27, 1995 |
|
Khaled K, Vause S: Genital mutilation: A continued abuse. Br J Obstet Gynaecol 103: 86, 1996 |
|
Paul BK: Maternal mortality in Africa: 1980-87. Soc Sci Med 37: 745, 1993 |
|
Kenyatta J: Facing Mt. Kenya. New York, Random House, 1965 |
|
El Saadawi N: The Hidden Face of Eve: Women in the Arab World. London, Zed Books, 1980 |
|
Lowenstein LF: Attitudes and attitude differences to female genital mutilation in the Sudan: Is there a change on the horizon? Soc Sci Med 12: 417, 1978 |
|
Walker A: Possessing the Secret of Joy. New York, NY, Harcourt Brace Jovanovich, 1992 |
|
El Dareer A: Epidemiology of female circumcision in the Sudan. Trop Doct 13: 41, 1983 |
|
El Dareer A: Attitudes of Sudanese people to the practice of female circumcision. Int J Epidemiol 12: 138, 1983 |
|
Dirie MA, Lindmark G: Female circumcision in Somalia and women's motives. Acta Obstet Scand 70: 581, 1991 |
|
Rispler-Chaim V: Islamic medical ethics in the 20th century. J Med Ethics 15: 203, 1989 |
|
Hodgkinson DJ, Hait G: Aesthetic vaginal labioplasty. Plast Reconstr Surg 74: 414, 1984 |
|
Laufer MR, Galvin WJ: Labial hypertrophy: A new surgical approach. Adolesc Pediatr Gynecol 8: 39, 1995 |
|
El Dareer A: Complications of female circumcision in the Sudan. Trop Doct 13: 131, 1983 |
|
Agugua NEN, Egwuatu VE: Female circumcision: Management of urinary complications. J Trop Pediatr 28: 249, 1982 |
|
McCaffrey M, Jankowska A, Gordon H: Management of female genital mutilation: The Northwick Park hospital experience. Br J Obstet Gynaecol 102: 787, 1995 |
|
Dirie MA, Lindmark G: A hospital study of the complications of female circumcision. Trop Doct 21: 146, 1991 |
|
Ozumba BC: Acquired gynetresia in eastern Nigeria. Int J Gynecol Obstet 37: 105, 1992 |
|
De Silva S: Obstetric sequelae of female circumcision. Eur J Obstet Gynecol Reprod Biol 32: 233, 1989 |
|
McSwiney MM, Saunders PR: Female circumcision: A risk factor in postpartum haemorrhage. J Postgrad Med 38: 136, 1992 |
|
Baker CA, Gilson GJ, Vill MD, Curet LB: Female circumcision: Obstetric issues. Am J Obstet Gynecol 169: 1616, 1993 |
|
Gabbar IA: Medical protocol for delivery of infibulated women in Sudan. Am J Nurs 85: 687, 1985 |
|
Council on Scientific Affairs, American Medical Association: Council report: Female genital mutilation. JAMA 274:1714, 1995 |
|
American College Obstetricians and Gynecologists Committee Opinion Number 151, January 1995, on Female Genital Mutilation issued by the Committee on Gynecologic Practice and the Committee on International Affairs |
|
Grimes DA: Routine circumcision of the newborn infant: A reappraisal. Am J Obstet Gynecol 130: 125, 1978 |
|
Ntiri DW: Circumcision and health among rural women of southern Somali as part of a family life survey. Health Care Women Int 14: 215, 1993 |
|
Gruenbaum E: The Islamic movement, development, and health education: Recent changes in the health of rural women in central Sudan. Soc Sci Med 33: 637, 1991 |