Authors
INTRODUCTION
Since the late 1960s and particularly after the 1970s, laparoscopic tubal sterilization has been established as one of the most frequently used methods of interval sterilization in women. However, for many years the need to simplify tubal sterilization by avoiding general anesthesia, incisions with their associated morbidity and prolonged recovery periods, a transcervical method of sterilization has been sought without success until recently when, because of new and improved technology, the ESSURE system was evaluated and finally approved for clinical use in November 2002.
PRELIMINARY HYSTEROSCOPIC METHODS OF STERILIZATION
In the early 1970s, hysteroscopic tubal sterilization was evaluated using insulated electrodes guided by hysteroscopy in an attempt to coagulate the intramural portion of the fallopian tubes in an ambulatory setting. Although this technique was fairly standard, the coagulation of this tubal area varied among investigators, particularly because of variations in wattage and time of delivery; however, the preliminary results seemed comparable with 75% to 80% bilateral initial tubal closure with one application and approximately 85% to 90% closure with a second application.1,2 However, because of sporadic reports of serious complications, an international registry of 10 collaborators from the United States, Thailand, West Germany, India, and Singapore was formed. 587 cases were analyzed with 333 (57%) found to have bilateral tubal closure at subsequent testing. There were 229 women (39%) who had one or both fallopian tubes open at subsequent testing or who had become pregnant despite tubal closure at patency test. However, the analysis also provided information regarding major complications, which included tubal and cornual ectopic pregnancies, uterine perforation, bowel damage, peritonitis, acute endometritis, excessive uterine bleeding, and one death as a result of bowel perforation and peritonitis. The overall rate of major complications was 4.3%. At the conclusion of this study in 1977, hysteroscopic sterilization by electrocoagulation, which was just beginning to peak and expand to more centers, was stopped altogether and abandoned.3
Other avenues for hysteroscopic sterilization were explored by delivering caustic or sclerotic substances to the tubes with no significant success.4 In 1975, Erb proposed the use of silicone rubber plugs directly formed in place to block the oviducts as a method of tubal occlusion, using a cornual salpingo-guided directly under fluoroscopy. The method was later on adapted to hysteroscopic delivery and clinical trials were initiated. While the method seemed to be an improvement from others, avoiding major complications, still remained cumbersome and time-consuming. Furthermore, when clinical trial results were evaluated, it was obvious that only 85% of patients could be properly sterilized with this method at the first attempt, and close to 90% with several attempts. The method never obtained FDA approval and the interest faded away, despite that in some European countries in selected centers it continued to be used. The original thought was to offer this method as reversible because apparently it was not expected to damage tubal epithelium significantly; nonetheless, histologic evaluations of the fallopian tubes when these plugs remained for some time, proved that the damage was extensive and it could not be expected to be a reversible method of sterilization.5
Soon after, the idea of using rigid plugs to occlude the uterotubal junction of the fallopian tubes was evaluated as well, and of the many methods that were proposed, two were evaluated more extensively than others, the Hossenian plug and the Brundin plug.
The Hossenian Plug
These devices were made of silicone rubber with four anchoring spines made of Elgiloy that served to fix and keep the device in place by penetrating the adjacent myometrium. A special assembly screw of stainless steel attaches the anchoring spines to the plug and provides a grasping base for the device carrier. The device is cone shaped and measures 1 mm or less at the tip increasing to approximately 2 mm at the base and its length varies from 7 to 9 mm. While the original studies in primates were successful (21 baboons) with restoration in fertility of those who were tested for that, when a clinical trial in humans began, 5 of 11 women conceived despite having the devices in place; therefore, no further trials were performed.5
The P-Block Tubal Plug
Another ingenious plug was the hydrogel Brundin tubal plug made of hydrogel, which is a polymeric compound of polyvinylpyrrolidone, a hydrophilic substance, methylcyanoacrylate and hydrophobic material. The body is 4 mm long and 1.2 mm wide, which is fixed on a nylon skeleton in its dry state and has 2-mm-wide nylon wings at the top to prevent expulsions from the tube before hydration. Swelling of the plug with moisture takes approximately 30 minutes, and this swelling maintains the plug in position. However, when tested clinically, 15 of 35 women achieved bilateral occlusion in the first attempt, and in two other women, a second procedure was necessary to achieve successful occlusion of the tubes. The long-term results in these 15 patients show four subsequent pregnancies, perhaps all caused by faulty placement or expulsion of the device. Furthermore, in 15 patients insertion was not possible. Therefore, further clinical trials were discontinued.5
Intratubal Devices
An intratubal device made of nylon thread, 1 mm in diameter and 23 mm in length, was also tested using small-caliber hysteroscopes for its placement to avoid cervical dilatation; however, although the placements were easy and successful, the nylon thread did not occlude the tubal lumen, as demonstrated by hysterosalpingography; therefore, when tested in clinical trials, unwanted pregnancies occurred, (5 pregnancies in 95 women with successful insertions) as expected; therefore, this method also was discontinued.5
THE ESSURE MICRO-INSERT SYSTEM
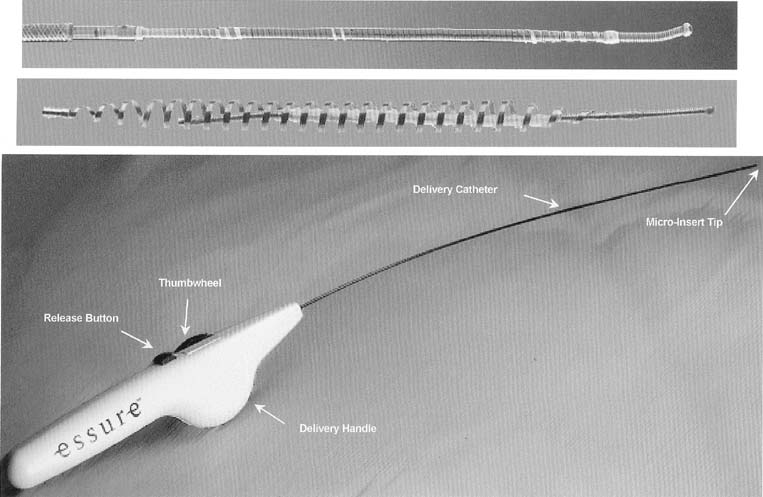
The ESSURE micro-insert is a microcoil that consists of a stainless steel inner coil, an outer coil made from nitinol and polyethylene terephthalate (PET), and Dacron fibers. The inner coil attaches the device to the guidewire used in its placement. The outer coil anchors the device in the fallopian tube on deployment. For the insertion, the device is maintained in a low-profile position through the use of a release catheter. A hydrofilled catheter facilitates the access of the tube and commands the guidewire, release catheter, and the device. The entire system is attached to a handle, aligned for one-hand release of the device. The device is delivered through a 5-French operating channel of a small-caliber hysteroscope (Fig. 1)
|
The PET fibers have had widespread clinical use for more than 40 years and have been demonstrated to produce an immediate local inflammatory response characterized by macrophages, fibroblasts, foreign body giant cells, and plasma cells. A moderate foreign-body inflammatory reaction is solicited by the PET fibers. This inflammatory response peaks between 2 and 3 weeks, after which the inflammatory response slowly resolves during a 10-week period. Extensive fibrosis results, causing occlusion and chronic anchoring of the PET material and any associated medical device.6
Technique of Insertion and Deployment
The patient is placed in the dorsal lithotomy position and the vaginal area and cervix cleansed with an antiseptic solution. A paracervical block is performed with a local anesthetic. Any local anesthetic can be used to perform the paracervical block, nonetheless, because of its low toxicity; an ester-type of anesthetic is preferable such as chloroprocaine, (Nesacaine) 1% solution, injecting 4 to 6 mL of the solution superficially at the base of each uterosacral ligament. A small amount of anesthetic (.5 mL) can also be applied on the anterior lip of the cervix to place the tenaculum without discomfort to the patient.
A small-caliber, 3.9 to 5.9 mm OD hysteroscope with continuous flow system is used. The tenaculum is optional, placed on the anterior lip of the cervix and hysteroscopy performed without previous cervical dilatation. Low viscosity fluids such as normal saline are preferable when using the hysteroscopic method with a continuous flow system. The normal saline is warmed to room temperature to avoid discomfort to the patient by cooling.
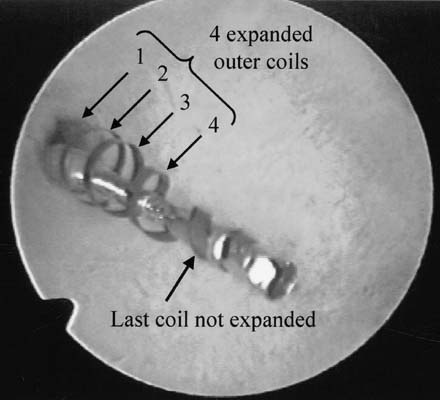
These procedures are best performed with a video camera to share with the patient the steps in performing the sterilization. The uterine cavity is evaluated and both tubal openings are observed. The ESSURE micro-insert is fed through the 5-French operating channel of the hysteroscope and gently guided into the tubal opening until the dark circle of the outer catheter comes into view, signifying time for deployment. The wheel in the handle is activated until a stop occurs, showing the micro-insert in the tubal lumen still not deployed in the catheter. A metal notch marker comes into view, signifying good placement, and by pressing the small button in the handle, the micro-insert is deployed. Further turning of the wheel in the handle will demonstrate the anchoring of the micro-insert by expansion of the spring outer metal. Several counterclockwise turns finally detaches the delivery system and the micro-insert proximal end is evaluated by hysteroscopy to assure that 5 to 10 mm (5 to 10 coils) of trailing micro-insert are in the uterine cavity. The same procedure is performed in the opposite fallopian tube (Figs. 2,3)
|
|

Evaluation of the ESSURE Micro-Inserts in a Prehysterectomy Study
To evaluate the feasibility of insertion, anchoring and complete tubal occlusion produced by the ESSURE micro-inserts, studies were designed to insert these devices in women who required hysterectomy and were willing to have this device tested. The initial study evaluated acute anchoring and feasibility of insertion and the woman underwent immediate hysterectomy. The second group of patients required to wait at least 3 months after the tubal devices were inserted to have a hysterectomy, to evaluate histology and tubal closure. At hysterectomy, the portion of the fallopian tubes containing the device was removed for histologic evaluation. Forty-three patients underwent device placement with the ESSURE micro-inserts. Forty-one patients had device placement in both fallopian tubes and two patients each had device placement in one tube, with a total of 84 tubes treated with device placements. The success of the device placements occurring in at least one tube in 43 patients or 50 patients per 84 (68%) attempts. Because of the uterine pathology present in this patient population, the device placement rate was significantly less than experienced in the intended sterilization population. Failure to place the device was considered to be device-related in only one tube (1%). In this case, the catheter failed to retract from the device. The cause of this failure was identified and resolved with design change. In those patients with uterine myomas or thickened endometrium who permitted visualization of the tubal ostium, placement of the device was achieved. The average procedure time was 15 minutes. No intraoperative adverse effects were noted during placement.6
The patients in this study were followed-up until their hysterectomy, which was performed between 24 hours and 14 weeks after device placement. Most were performed at the completion of almost 3 months. Tubal occlusion was evaluated by hysterosalpingography before the hysterectomy and all tubes (50/50; 100%) were found to be occluded. The histologic evaluation in 27 patients accounting for 47 tubes was also performed with an 80% occlusion rate in those patients with devices that had been in place for more than 4 weeks and consistent with 100% functional occlusion noted by the hysterosalpingogram performed before hysterectomy.
HISTOLOGIC EVALUATION
There were 47 patients enrolled and who underwent implantation with devices in the prehysterectomy trial. Table 1 provides the length of the device-wearing for each of the devices interaction in this study. There were no reports of pain during device-wearing. No pain was reported during pelvic examinations conducted just before hysterectomy in any of the patients. There was no evidence of inflammation, ulceration, or hemorrhage on gross examination of the uterus, except one patient with adenomyosis who was noted to have ulceration and hemorrhage in the uterine cavity; both fallopian tubes in this patient were unremarkable.
Table 1. Length of Device Wearing by Device Iteration
| Length of Device Wearing | No. Patients |
| <2 wk | 02 |
| 2–5 wk | 05 |
| 5–7 wk | 01 |
| 7–9 wk | 00 |
| 9–11 wk | 02 |
| 11–13 wk | 06 |
| 13–15 wk | 16 |
| >15 wk | 01 |
| Pending hysterectomy | 00 |
| Total | 33 |
Tubal occlusion was evaluated just before the hysterectomy by HSG. In tubes in which device movement or perforation did not occur occlusion was noted in 50 of 50 (100%) tubes evaluated.6
Methodology for Histologic Evaluation
Fallopian tubes of all patients enrolled in the study underwent both gross and microscopic examination. Care was taken at the time of hysterectomy to remove the uterus and tubes in block, without cutting into the device or using electrosurgery on the tubes. Once the tubes were removed, the uterus and tubes were x-rayed to determine the position of the devices in the tubes. Markers were placed at the uterotubal junction (UTJ) as a landmark. The uteri were then bivalved and the uterine end of the device was evaluated for position as well as to examine the local response to the device in the uterus. The uterine cornua and tubes were then excised and placed in formalin. An independent histopathologist then conducted gross examination of the tubes. Subsequent to the gross examination, the tubes were sent for processing at the Core Laboratory and then returned to the independent histopathologist for microscopic evaluation.6 The tubes were processed at the Core Laboratory as follows: the tubes were x-rayed to determine placement of the device within the tube. The specimens were then dehydrated in alcohol and xylene and embedded in methacrylate (MMA) until polymerized.
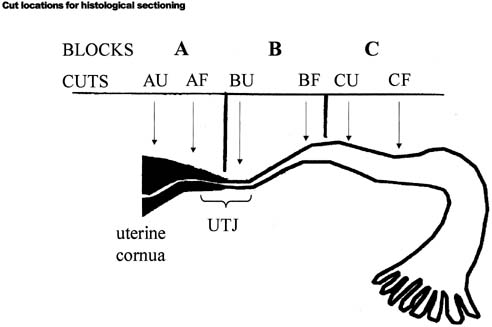
The resulting block was then compared with the x-ray and the imbedded fallopian tube was divided into three blocks according to the device position, using a diamond blade saw. (Figs. 4,5)
|
|
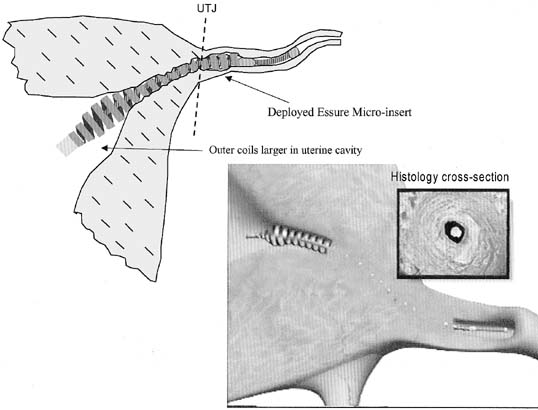
Block A included the uterine cornua up to the (UTJ). Block B included the UTJ to the proximal isthmic portion of the tubes, and block C included the proximal isthmic portion to a point within 5 mm distal to the end of the device. Two cross-sectional sections were then taken from the uterine end of blocks A, B, and C, and the fimbrial end of block C, using a diamond saw.
These sections were ground down to a thickness of approximately 50 to 100 microns for microscopic evaluation. Slides were then prepared from each section: One was stained in H and E and the other one with Goldner's trichrome. The MMA embedding process and the diamond saw cutting were undertaken to observe the integrity of the relationship with the device and the tissue.
Results of Histologic Evaluation
Patients wore the device ranging from 8 days to 14 weeks. The distribution of wearing time is noted in Table 1. Table 2 provides some quantitative information derived from the histology slides. The information is presented by wearing time to more clearly view the increasing tissue response seen over time.
Table 2. Histology Results by Tube
| Wearing Time (wks) | ||||||
| 1–4 n = 9 | 4–8 n = 5 | 8–12 n = 3 | 12–16 n = 8 | <16 n = 1 | Total N = 23 | |
| Tissue Reaction | Tubes | Tubes | Tubes | Tubes | Tubes | Tubes |
| Moderate/extensive acute inflammation | 7/9 | 2/5 | 0/3 | 17/29 | 0/1 | 26/47 |
| Moderate extensive chronic inflammation | 8/9 | 4/5 | 3/3 | 26/29 | 1/1 | 42/47 |
| Moderate/extensive loose fibrosis | 7/9 | 3/5 | 3/3 | 26/29 | 1/1 | 40/47 |
| Moderate/extensive dense fibrosis | 7/9 | 2/5 | 3/3 | 25/29 | 1/1 | 38/47 |
| Moderate/extensive disruption of epithelium | 7/9 | 4/5 | 3/3 | 29/29 | 1/1 | 44/47 |
| Moderate/extensive disruption of lamina propria | 7/9 | 4/5 | 3/3 | 28/29 | 1/1 | 43/47 |
| 80–100% obliteration of tubal lumen | 4/9 | 5/5 | 3/3 | 26/29 | 1/1 | 39/47 |
| Overall reaction to device = extensive | 3/9 | 1/5 | 3/3 | 26/29 | 1/1 | 34/47 |
| Overall reaction to device = moderate | 2/9 | 3/5 | 0/3 | 01.29 | 0/1 | 06/47 |
| Overall/reaction to device = mild | 4/9 | 1/5 | 0/3 | 02/29 | 0/1 | 07/47 |
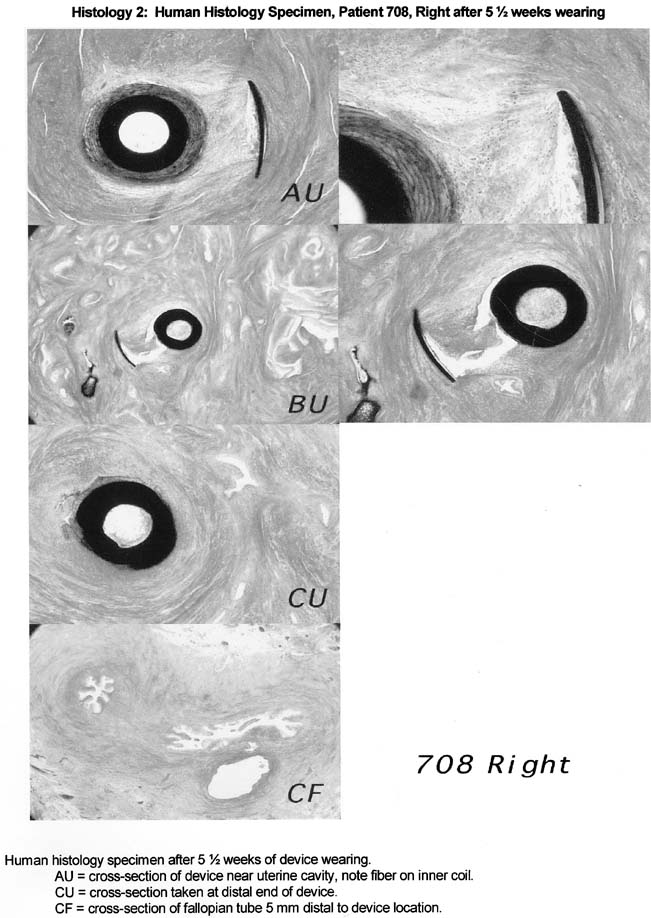
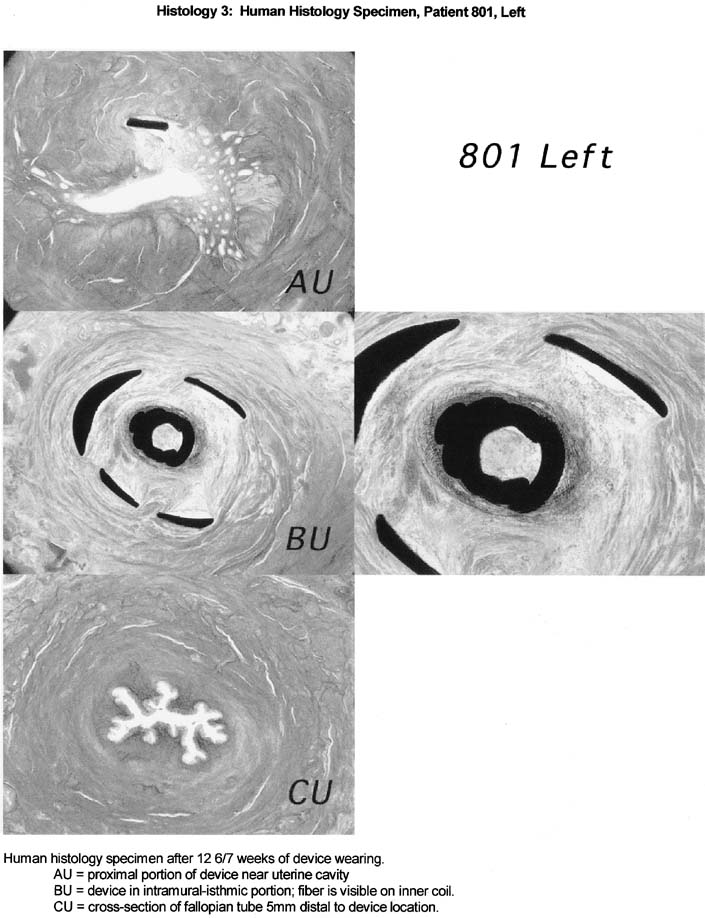
The histological response to the ESSURE micro-insert is characteristic of the histological response observed with the use of PET fibers in other anatomical sites. Specifically, the PET fibers appear to elicit strong fibrous and inflammatory tissue response that extends into the space viewed in the inner and outer coils of the ESSURE micro-inserts. The tissue response consists predominantly of macrophages and mononuclear cells, with some foreign body-type giant cells and acute inflammatory cells response. The fibrous response consists of both loose and dense fibrosis. In the studied cases with 3 months of wearing time, smooth muscle cells are also observed migrating from fallopian tube wall into the space viewed with the inner and outer coil. This response clearly demonstrated with comparable cross-sections of tubal segments of patients with and without the devices.
In addition, the fibrosis and tissue reaction were noted to be localized to the inner portions of the fallopian tube wall. There was no evidence that the fibrosis induced by the device will extend beyond the wall of the fallopian tube or cause peritubal adhesions or serositis (Figs. 6, 7, 8).
|
|
|
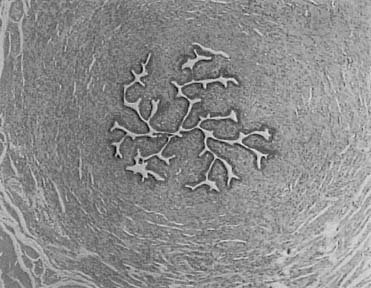
Normal tubal architecture was present within 5 mm distal to the end of the device. The histological analysis revealed normal tubal segment that were absent of inflammatory cells. This can be observed in specimens collected that were distal to the device (Fig. 9)
|

An independent histopathologist for the study concluded that the initial response to the ESSURE micro-insert is occlusive in nature and should provide for long-term anchoring of the device and pregnancy prevention. The study demonstrated that the tissue reaction is predictable, occurred in all specimens that contained fiber, and is localized to the device.
CLINICAL RESULTS
Eight hundred seventy-one women with documented fertility who selected investigational hysteroscopic permanent contraception with ESSURE micro-inserts were recruited. Two hundred and sixty-nine women in phase 2 and 602 women in a pivotal study were involved. Two hundred and twenty-seven (84%) of women in phase 2 were attempted and 518 (86%) in the pivotal study. One hundred eighty-seven out of 193 women (96.4%) in the phase 2 study had bilateral occlusion at 3 months. Four hundred sixteen out of 433 women (96.1%) in the pivotal study. Bilateral occlusion at 6 months was demonstrated in all 194 patients (100%) in the phase 2 study and 420 out of 433 (97.7%) in the pivotal study. One hundred forty-three women in phase 2 study were relying on the ESSURE device for more than 1 year. No pregnancies have occurred in either study. The procedure was well-tolerated by the majority of patients (more than 90%), it averaged 13 to18 minutes, and resulted in little or no postoperative discomfort. Local anesthesia (43.8%), intravenous sedation, and/or analgesia (52.4%) were the anesthesia used for these procedures in 93.0% of patients in the phase 2 study and 92.8% in the pivotal study. As time passes, the number of patients who had placement of these micro-inserts have increased as well as their follow-up with more than 500 women relying on the devices for contraception for more than 1 year and more than 300 for more than 2 years. As of this writing, no pregnancies have occurred in patients with properly fitted devices7,8,9,10 (Tables 3, 4, 5).
Table 3. Clinical Study Demographics
| Phase II | Pivotal | |
| Patients enrolled | 269 | 602 |
| Patients attempted | 227 (84%) | 518 (86%) |
| Average age | 35 | 32 |
| Age range | 23–45 | 21–40 |
| Height | 64.17 in. | 64.45 in. |
| Weight | 154.0 lb | 159.49 lb |
| Gravidity | 2.6 | 3.0 |
| Parity | 2.2 | 2.3 |
Table 4. Clinical Effectiveness
| Phase II | Pivotal | |
| Bilateral occlusion at 3 mon | 96.4% | 96.1%* |
| (n = 187/194) | (n = 416/433) | |
| Bilateral occlusion at 6 mon | 100% | 97.7% # |
| (n = 194/194) | (n = 420/433) | |
| Woman-months of wearing | 3974 | 3462 |
| Woman-months of effectiveness | 3057 | 1360 |
| Number of women relying on | 143 | N/A |
| Essure pbc > 1 tear | ||
| Number of pregnancies | 0 | 0 |
* Of the 17 patients not occluded at 3 months, only 4 had undergone repeat HSGs at the time of this data freeze
# 5/13 patients have undergone repeat HSGs at 6 months, 8 patients are awaiting evaluation
Table 5. Adverse Events
| Phase II | Pivotal | |
| Percent experiencing AE | 5.7% (13/227) | 4.2% (22/518)* |
| Type of AE | ||
| Expulsion | 0.4% (n = 1) | 2.7% (n = 14) |
| Perforation | 1.8% (n = 4) | 0.8% (n = 4) |
| Proximal band detachment | 1.3% (n = 3) | 0.4% (n = 2) |
| Undesirable device location | 1.3% (n = 3) | 0.2% (n = 1) |
| Others | 0.9% (n = 2) | 0.6% (n = 3) |
*Of 14 patients experiencing expulsion, 8 had reattempts resulting in successful replacement of the device. Three were also found to have a patency but underwent sterilization before reattempts were considered. One patient was found to be occluded despite the expulsion.
PRESENT STATUS
While many physicians have been trained specifically for the use of this method of sterilization, the long-term results from procedures performed by these practitioners still remains to be evaluated. The logistics of introducing a new medical procedure is being explored as far as coding, standardized training by experienced hysteroscopics familiar with this method of sterilization, and future follow-up of these patients that will derive in meaningful statistics regarding long-term results. Nonetheless, from preliminary evaluation of patients all over the world who have undergone this method of sterilization, it seems that the results continue to provide uniform consensus on the satisfactory effectiveness of the ESSURE system.
SUMMARY AND CONCLUSIONS
While an ambulatory transcervical method of sterilization has been elusive, the new ESSURE micro-insert system has opened a new avenue as an alternative to tubal sterilization by fulfilling the vacuum of having a transcervical method of sterilization truly ambulatory, not requiring general anesthesia or incisions in the body, but using the natural body passages. Because of its manufacturing and thin deployment catheter, it can be deployed transcervically in the fallopian tube using a small-caliber hysteroscope with a 5-French operating channel, therefore avoiding cervical dilatation that permits its use in an office setting under local anesthesia. In vitro and in vivo studies have demonstrated the feasibility of insertion of these devices and the occurrence of complete tubal occlusion by fibrosis of the lumen. The preliminary clinical trials have shown promising results as far as pregnancy prevention with no significant associated morbidity, therefore making the method an excellent alternative for women seeking permanent contraception. Because its performance is a truly ambulatory office procedure, it decreases morbidity, cost, and inconvenience to the patient. The clinical trials performed thus far, have demonstrated a promising long-term safety and effectiveness of the ESSURE system as a contraceptive method.
REFERENCES
Sciarra JJ: Hysteroscopic approaches for tubal closure. In Zatuchni GI, Labbock MH, Sciarra JJ (eds): Research Frontiers in Fertility Regulation. pp 270-286, Hagerstown, MD, Harper and Row, 1980 |
|
Zatuchni GI, Shelton JD, Goldsmith A et al: Female Transcervical Sterilization. Philadelphia, Harper and Row, 1983 |
|
Darabi K, Richart R: Collaborative study on hysteroscopic sterilization procedures: Preliminary Report. Obstet Gynecol 49:48-54 |
|
Valle RF: Tubal catheterization for sterilization purposes. In Gleicher N, et al (eds): Tubal Catheterization Procedures. pp 139-160, New York, Wiley, 1992 |
|
Valle RF, Read T: Hysteroscopic sterilization. In Baggish MS, Barbot J, Valle RF (eds): Diagnostic and Operative Hysteroscopy: A Text and Atlas. pp 353-366, 2nd ed.. Boston, MA, Mosby, 1999 |
|
Valle RF, Carignan CS, Wright TC: and the STOP Prehysterectomy Investigation Group: Tissue response to the STOP microcoil transcervical permanent contraceptive device: Results from a Prehysterectomy study. Fertil Steril 76:974-980 |
|
Kerin JF, Carignan CS, Cher D: The safety and effectiveness of a new hysteroscopic method for permanent birth control: Results of the first ESSURE PBC Clinical Study. Aust NZ J Obstet Gynaecol 41:364-370 |
|
Valle RF, Cooper JJ, Kerin JF: Hysteroscopic tubal sterilization with the ESSURE non-incisional permanent contraception system. Obstet Gynecol 99:11S, 2002 |
|
Kerin JF, Cooper JM, Price T et al: Hysteroscopic sterilization using the ESSURE micro insert: Results of a multicenter phase II study. Hum Reprod (In press) |
|
Cooper JM, Carignan CS, Cher D et al: Microinsert nonincisional hysteroscopic sterilization. Obstet Gynecol 02:59-67, 2003 |