Hysteroscopy and Infertility
Authors
INTRODUCTION
Evaluation of the cervix, endocervical canal, uterine cavity, and fallopian tubes should be part of the infertility evaluation. Hysterosalpingography, endometrial biopsy, and, on rare occasions, the Rubin test have been used to evaluate tubal patency and the uterine cavity. Because of the drawbacks associated with these techniques and the need to visually evaluate the endocervical canal and uterine cavity, hysteroscopy has been added to these evaluations. Because the uterine factor accounts for less than 10% of infertility cases and because the procedure adds to the cost of routine evaluations, hysteroscopy has been used selectively.1,2,3 Uterine factors that benefit most from hysteroscopic evaluation are structural abnormalities that distort uterine cavity symmetry or obstruct the tubal passages: submucous leiomyomas, intrauterine adhesions, uterine anomalies, and tubal cornual occlusions. Although these abnormalities cause problems in pregnancy maintenance rather than infertility, they are included in this review because they impair and obstruct normal reproduction.4,5
BASIC METHODS AND INSTRUMENTS FOR HYSTEROSCOPY
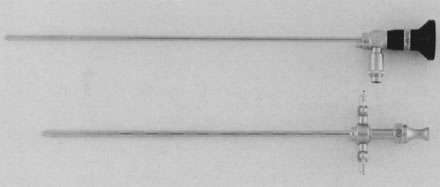
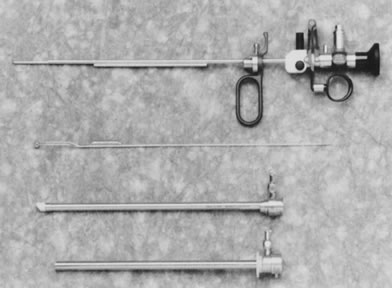
To perform panoramic hysteroscopy, the uterine cavity, a virtual cavity, should be expanded with an appropriate distending medium. Because of the thickness and resistance of the uterine walls, distention requires positive pressure. Three media can be used: carbon dioxide (CO2) gas; low-viscosity fluids with or without electrolytes; and high-viscosity fluids, such as dextran. CO2 gas is the cleanest medium because its refractory index permits the best visualization when no interfering blood or bubbles are present. It is best used with small-caliber (outer diameter [OD] less than 5 mm) diagnostic hysteroscopes, which do not require cervical dilatation. The CO2 gas is delivered at a rate of 40–60 mL/min with an intrauterine pressure of no more than 100 mmHg (Fig. 1). These evaluations are usually performed in an office setting and usually can be accomplished in less than 5 minutes. With CO2 gas, any manipulation of the endometrium, including uterine sounding, should be avoided so as not to traumatize the tissue before exploration begins.
|

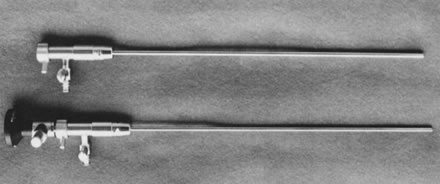
Low-viscosity fluids with or without electrolytes are used with operative hysteroscopes because they allow uterine washings to remove the debris (blood clots or small amounts of blood) usually produced during cervical dilatation and intrauterine surgery. Low-viscosity fluids containing electrolytes, such as normal saline, dextrose 5% in half normal saline, or Ringer's lactate, are most useful and practical when operating with mechanical instrumentation or using fiberoptic lasers because these two modalities lack conductivity. When the resectoscope is used with electrosurgery, only fluids without electrolytes should be employed. These are dextrose 5% in water, glycine 1.5%, sorbitol 3%, and mannitol 5%. They permit use of electrosurgery and avoid conductivity, decreasing the chances of damage to surrounding structures and providing effective and controlled energy to the treated areas (Fig. 2). High-viscosity fluids, such as dextran and, specifically, Hyskon, a 70,000-molecular weight dextran in 10% dextrose, can be used during operative hysteroscopy, particularly when visualization is impaired by bleeding or difficult dissections. This viscous solution does not mix well with blood and, due to its thickness and viscosity, requires only small amounts to be instilled in the uterine cavity during surgery. Hyskon is nonconductive, does not contain electrolytes, and though useful when using mechanical instrumentation or lasers, it is somewhat cumbersome with electrosurgery, specifically the resectoscope. The washing effect of the instrument is lost due to the viscosity of the substance. Furthermore, Hyskon caramelizes around the electrodes, requiring their frequent replacement.
|

Whatever method is chosen for hysteroscopy, the properties, qualities, and drawbacks of each substance should be considered. Complications related to excessive amount of fluid intravasated during operative hysteroscopy can be avoided by careful monitoring of the quantity of fluid infused and recovered. Measuring the amount of nonrecovered fluid, which in all probability has been intravasated, alerts the operator to possible fluid overload.
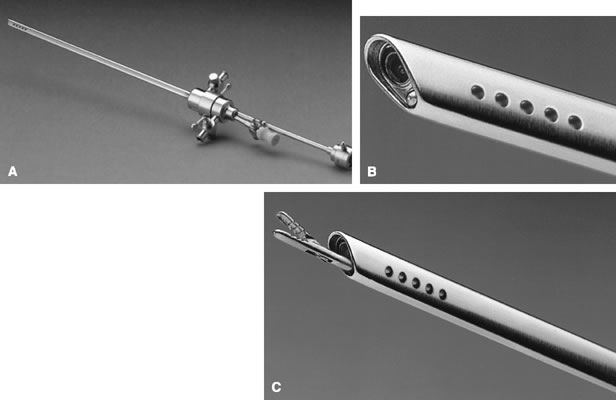
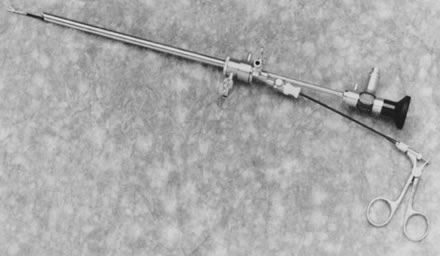
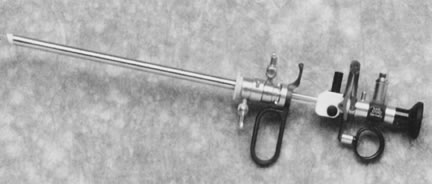
Most diagnostic hysteroscopes of less than 5-mm OD do not provide adjacent channels for operations, and are strictly for diagnostic use. Continuous flow systems have been successfully adapted to small-caliber hysteroscopes, however. Therefore, liquid media can be used with these endoscopes, also permitting the performance of some surgical procedures. The operative hysteroscopes are larger and usually have a 7- to 8-mm OD and a 7-French operating channel to introduce instrumentation, usually of the semi-rigid type when mechanical instruments are used. Alternatively, fiberoptic lasers can be introduced through the operating channel, as well as polyethylene catheters to wash from the cavity the debris, blood clots, or mucus that interfere with visualization (Figs. 3, 4, 5, 6, 7, and 8).
|
|

|
|
|

|
Additionally, because cervical dilatation is avoided, minimal or no anesthesia is required to perform hysteroscopic procedures in the office setting. Therefore, paracervical block anesthesia with 3–4 mL of a local anesthetic, such as chloroprocaine hydrochloride 1% (Nesacaine), will be sufficient to abolish any discomfort for the patient. Furthermore, the need for analgesia is also markedly reduced.
Hysteroscopy can be performed using larger operative hysteroscopes (7-mm OD) under local anesthesia; however, with a paracervical block, the need for cervical dilatation requires a larger amount of anesthetic to be infiltrated superficially in the paracervical areas (base of the uterosacral ligaments) with 8 to 10 mL of the solution. In these situations, however, the procedures performed should be expedited and confined to minor surgical procedures. Extensive dissections or procedures using the resectoscope are better performed under regional, spinal, or general anesthesia.
The resectoscope provides inflow and outflow channels by a mechanism of assembling two concentric sheaths of 8- to 9-mm OD. The rectoscope permits the use of electrodes such as the loop to resect, or the rollerball or rollerbar to coagulate; additionally, electrical knives are available to cut thick structures, such as uterine septa or adhesions (Figs. 9 and 10).
|
|
Most hysteroscopes have a 4-mm OD telescope with a foreoblique (30°) angle of vision to permit visualization of the uterotubal areas. The resectoscope has a 12–25° foreoblique view, most useful in obtaining a good visualization of the working electrode as it is moved forward by a spring-loaded mechanism.
High-intensity xenon light is most useful, particularly when using video cameras. Video cameras with high resolution and magnification simplify hysteroscopic evaluation and surgery, providing excellent resolution, comfort to the operator, and the ability to share the procedure with the operating team. The findings and results can be shared with the patient (Figs. 11, 12, and 13).
|

|

|

HYSTEROSCOPY IN THE EVALUATION OF INFERTILITY
The hysterosalpingogram is a practical method to evaluate the uterine cavity and the fallopian tubes. Its accuracy has been challenged, however, particularly for false-positive results, usually due to air bubbles, blood clots, debris, or distortion of the uterine cavity during the examination. This problem can be compounded by the dye chosen for the examination and the performance of hysterosalpingography.6 When patients with abnormal hysterosalpingograms have been evaluated by hysteroscopy, a 30% rectification of the abnormal hysterosalpingogram has been reported.7, 8 For this reason, when the hysterosalpingogram is abnormal, it is important to add endoscopy to confirm or rectify the abnormal hysterographic findings. This evaluation not only provides more accurate diagnosis, but also offers the opportunity for direct treatment under visual control. A submucous myoma may be diagnosed and treated hysteroscopically, a polyp may be located and removed, adhesions confirmed and treated, and a symptomatic uterine septum divided (Tables 1 and 2).
Table 1. Hysteroscopy for infertility (indications)
Abnormal hysterogram
Abnormal uterine bleeding
Suspected intrauterine pathology
Uterine anomalies
Unexplained infertility
Pregnancy wastage
Planned intrauterine surgery
polyps
submucous leiomyomas
uterine septa
intrauterine adhesions
misplaced or embedded foreign bodies
tubal cannulation
Table 2. Hysteroscopic confirmation of hysterographic abnormal findings
Author | No. patients with abnormal hysterograms | Percentage confirmed by hysteroscopy |
Edstrom and Fernstrom | 30 | 53.3 |
Englund et al. | 21 | 50 |
Gribb | 14 | 43 |
Levine and Neuwirth | 11 | 60 |
Norment | 50 | 60 |
Porto and Serment | 76 | 58 |
Sugimoto and Nishimura | 206 | 65 |
Taylor and Cumming | 68* | 55.5 |
Valle | 63 | 68.3 |
Varangot et al.† | 71 | 55 |
*Normal hysterograms; only 30 confirmed.
†Contact hysteroscopy.
(Valle RF, Sciarra JJ: Current status of hysteroscopy in gynecologic practice. Fertil Steril 32:619, 1979)
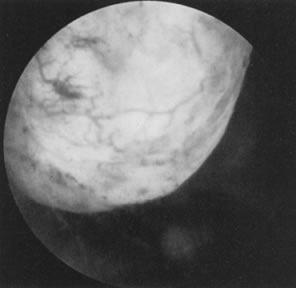
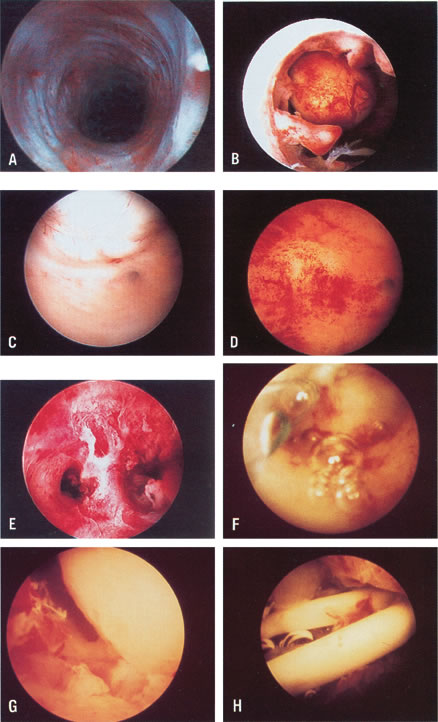
The hysterosalpingogram can provide information about other areas that hysteroscopy cannot, for example, tubal lumen symmetry, suspicion of salpingitis isthmica nodosa, diverticula, normal or abnormal tubal epithelial folds, and tubal patency. Hysteroscopy and hysterosalpingogram are not exclusive of each other but are complementary, and should be used as such. Because hysterosalpingography is easier to perform and interpret than hysteroscopy, less expensive, and provides valuable information about the uterine cavity and fallopian tubes, it should continue to be the first line of investigation in the evaluation of the infertile woman. Hysteroscopy should be used to assess the normal hysterosalpingogram to rectify or confirm previous abnormal hysterographic findings (Table 3).9, 10, 11, 12 The atraumatic introduction of the diagnostic hysteroscope through the endocervical canal provides an excellent method for evaluating this previously inaccessible area. Scars can be ruled out, as can structural abnormalities of the endocervical folds and glands, and adhesions or stenosis of the internal cervical os. The cornual regions of the uterus and the uterotubal junctions have been difficult to evaluate without direct visualization. Adhesions, small polyps acting like valves, sometimes occlude these areas, which can be thoroughly explored by direct visualization. These anatomic lesions can be treated concomitantly (Figs. 14, 15, 16, 17, 18, 19, and 20; Color Plate 1A and B).
Table 3. Comparison of hysteroscopy and hysterosalpingography
Hysteroscopy | Hysterosalpingography |
Direct visualization of uterine cavity | Indirect visualization (contrast medium's shadow) |
Diagnosis and specification of intrauterine lesions | Recognition and presumptive diagnosis |
Possibility of targeted biopsies and surgical therapy | No possibility |
Precise localization of abnormalities (polyps, myomas, malformations , adhesions, carcinoma and precursors) | Localization of abnormalities is less precise |
Direct access to tubal lumen (biochemical or biophysical studies, selective chromopertubation) | No direct access (indirect study, possible spasm) |
No evaluation of fallopian tubes possible | Evaluation of tubal lumen, patency, epithelial folds and abnormalities |
Requires special instrumentation and experience, more expensive | Simple instrumentation, easy to perform, less expensive |
|

|

|
|
|
|

|

|
The evaluation of patients with unexplained infertility requires meticulous attention to details of all the basic methods for evaluating infertility, reassessing the normalcy of reproductive anatomy. These patients frequently require a laparoscopy, which should be accompanied by hysteroscopy. Even a minor abnormality that may not completely explain the infertility should be treated.
Hysteroscopy offers an excellent method of evaluation and therapy, particularly in patients who have undergone intrauterine surgery, such as for intrauterine adhesions, uterine septa, and submucous myomectomy, or when symptoms, such as abnormal bleeding, pain, or dysmenorrhea, persist.13, 14
The diagnostic capabilities of the hysteroscope stop at the uterotubal junction and sometimes only permit visualization of the first 2–3 mm of the tubal lumen. Hysteroscopy offers an excellent platform for launching mini-endoscopes that can be guided directly into the tubal lumen. Eventually, high-resolution fibers can provide good visualization of these small areas. Then salpingoscopy may become a practical method of evaluating and perhaps treating intratubal abnormalities.15, 16
The narrow diameter of this area (less than 0.5 mm) makes this method difficult, as compared to tubaloscopy from the fimbriated end, which benefits from the larger diameter of the tube, as well as the possibility of fluid distention and continuous washing. Nonetheless, this method of tubal evaluation continues to be pursued and remains a promising technique.
THERAPEUTIC HYSTEROSCOPY IN INFERTILITY
The hysteroscope offers not only the opportunity to visualize the intrauterine structures and provide diagnosis, but also therapeutic capabilities for conditions that in the past required a hysterotomy and, obviously, a laparotomy. Instruments can be guided visually and targeted to areas in the uterine cavity in need of treatment for uterine septa, intrauterine adhesions, polyps and submucous myomas, and tubal cornual occlusions.17, 18
Treatment of Uterine Septa
Uterine anomalies, specifically the uterine septum, can interfere with reproduction in about 25% of patients afflicted with this condition.19 Traditionally, the symptomatic uterine septum producing pregnancy wastage has been treated by Jones or Tompkins abdominal metroplasty.19, 20, 21 The ability to manipulate instruments inside the uterine cavity has provided the opportunity to treat the uterine septum transcervically. This method was tried blindly for many years, following Ruge's attempt at transcervical treatment.22 Although abdominal metroplasty gave excellent results in reproduction, it required a laparotomy and a hysterotomy with their inherent morbidity, particularly related to pelvic adhesions. Patients were hospitalized, experienced the usual postoperative convalescence, and waited 3–6 months to attempt conception. These patients were subjected to routine cesarean section when they achieved pregnancy and viability. Such drawbacks were overcome by the ability to transect the septum hysteroscopically on a day-surgery basis without invading the uterine walls and the abdominal cavity (see Fig. 20; see Color Plate 1).23, 24, 25
There are several methods to treat the uterine septum hysteroscopically. In the most widely employed method, mechanical semi-rigid scissors are used to divide the septum systematically until reaching the junction between the fibrotic septum and the myometrium. This is done by following the symmetry of both uterine tubal openings, and observing by hysteroscopy the rich myometrial vascularization of the area, and by laparoscopy the uniform translucency of the hysteroscopic light. Patients are given prophylactic antibiotics, using cephalosporins with 1 g of cefazolin sodium (Kefzol) intravenously during the procedure followed by cephalexin (Keflex) 500 mg by mouth four times daily for 3–4 additional days. Estrogens are given in the form of conjugated estrogens (Premarin) 2.5 mg twice daily for 30 days, and progesterone in the form of medroxyprogesterone acetate (Provera) 10 mg in the last 10 days of this artificial cycle to allow withdrawal bleeding. At the completion of hormonal treatment, a hysterosalpingogram is performed to assess the results of the hysteroscopic treatment; if satisfactory, the patient is allowed to conceive.
The results obtained have surpassed the previous metroplastic operations used in the treatment of the anomaly.26, 27 As an alternative to mechanical methods, fiberoptic lasers (neodymium:yttrium-aluminum-garnet [Nd:YAG], argon, and KTP-532 laser) with sculptured or extruded fibers can be used to divide the uterine septum.24 Care should be taken not to destroy the peripheral endometrium and to avoid uterine perforation by observing carefully the hysteroscopic light through the laparoscope. Bleeding may not be apparent once the myometrium is reached because of the coagulating power of the lasers.28 Alternatively, the resectoscope may be used with a modified loop electrode placed forward to cut the septum, or a narrow knife electrode can divide the septum by pushing forward. Nonetheless, care must be taken to avoid perforation. The coagulating power of the electricity may interfere with the observation of bleeding, which usually occurs at the myometrium. Therefore, the laparoscopic assistant using dimmed laparoscopic light should observe for uniform illumination provided by the hysteroscopic light (Table 4).24, 25, 26, 27
Table 4. Hysteroscopic metroplasty
Pregnancy | ||||||||||
Author | No. patients | Medium | Technique | IUD* | E/P† | Antibiotics | Term | Premature | Abortion | In progress |
Edstrom (1974) | 2 | Dextran 70, 32% | Rigid biopsy foreceps | + | + | — | — | 19 wks | — | — |
Chervenak and Neuwirth (1981) | 2 | Dextran 70, 32% | Scissors adjacent to hysteroscope | + | — | + | 1 | — | — | — |
Rosenberg et al. (1981) | 1 | Dextran 70, 32% | Flexible scissors | NA‡ | NA‡ | NA‡ | NA‡ | — | — | — |
Daly et al. (1983) | 25 | Dextran 70, 32% | Flexible scissors | — | + | — | 7 | — | 1 | — |
Perino et al. (1985) | 11 | CO2 | Flexible semi-rigid scissors | + | — | — | NA‡ | — | — | — |
DeCherney et al. (1986) | 72 | Dextran 70, 32% | Resectoscope | — | — | — | 58 | — | 4 | 4 |
Corson and Batzer(1986) | 18 | Dextran 70, 32%, CO2 | Resectoscope and rigid scissors | — | — | — | 10 | 1 | 2 | 2 |
Fayez (1986) | 19 | Dextran 70, 32% | Rigid scissors | Foley catheter | — | + | 14 | — | — | — |
March and Isreal (1987) | 91 | Dextran 70, 32% | Flexible scissors | + | + | — | 44 | 4 | 7 | 7 |
Valle (1987) | 59 | D5W/Dextran 70, 32% | Flexible, semi-rigid | — | + | + | 44 | 2 | 5 | — |
Choe and Baggish (1992) | 19 | Dextran 70, 32% | Nd:YAG with bare or sculptured fibers | Foley catheter | + | + | 10 | 1 | 1 | 3 |
Fedele et al. (1993) | 102 | Dextran 40, 10% in normal saline | Semi-rigid scissors (80) Argon laser (10) Resectoscope (12) | +(21) | +(39) | + | 45 | 10 | 11 | NA‡ |
Valle (1996) | 124 | D5 in 1/2 normal saline Glycine 1.5% | Semi-rigid scissors (98) Resectoscope (20) | — | + | + | 84 | 7 | 12 | — |
Totals | 545 | 317(78.3%) | 26(6.4%) | 43(10.6%) | 18(4.4%) | |||||
*IUD, Intrauterine device
†E/P, Estrogen/progestrone
‡N/A, Nonapplicable
Modified from Siegler AM, Valle RF: Therapeutic hysterocopy procedures. Fertil Steril 50:685, 1988.
Treatment of Intrauterine Adhesions
Intrauterine adhesions resulting from trauma to the postpartum or postabortal endometrium are known as Asherman's syndrome. This condition usually results in menstrual abnormalities, particularly amenorrhea, hypomenorrhea, or both and may also result in infertility and pregnancy wastage.29
The best screening method to rule out intrauterine adhesions is hysterosalpingography. Hysteroscopy will confirm the presence of adhesions, evaluate the type of adhesions, and serve to divide these adhesions under visual control (see Color Plate 1E). A 7- to 8-mm OD operative hysteroscope is used, with semi-rigid scissors and biopsy forceps to systematically divide the adhesions. Concomitant laparoscopy is used when extensive adhesions are present and when tubal occlusion is demonstrated on the hysterosalpingogram, as a guide to the hysteroscopic surgery.
Perioperative and postoperative antibiotics are usually prescribed in the form of cephalosporins with 1 g IV during the procedure, followed by cephalexin 500 mg orally four times daily for 5–6 days, particularly in women requiring an intrauterine splint after the surgery. Adjunctive hormonal treatment to stimulate re-epithelialization is used with conjugated estrogens, Premarin 2.5 mg orally twice daily for a 30- to 40-day cycle, with additional terminal progesterone as medroxyprogesterone acetate, 10 mg once a day in the last 6 to 10 days of this artificial cycle. At the conclusion of the hormonal therapy, a hysterosalpingogram is performed to evaluate the results of this therapy.
To determine the prognosis of the treatment, a three-stage classification of the adhesions (mild, moderate, and severe) is used based on the extent of adhesions seen on the hysterosalpingogram and the type of adhesions involved as determined by hysteroscopy.
Mild adhesions are usually filmy adhesions composed of basalis endometrium; they partially or totally occlude the uterine cavity. Moderate adhesions are composed of fibromuscular tissue covered by endometrium; they usually partially or totally occlude the uterine cavity, and bleed on division. Severe adhesions are composed of connective tissue. They usually do not have endometrial lining and may partially or totally occlude the uterine cavity.30 The restoration of normal menstruation is achieved in about 90% of the patients treated. The reproductive outcome parallels the extent and type of adhesions. The milder the adhesions, the better the prognosis. Older adhesions that more extensively occlude the uterine cavity have a poorer prognosis. Valle and Sciarra30 reported on 187 patients evaluated and treated by hysteroscopy with restoration of normal menstruation in 88.2%. The reproductive outcome correlated with the type of adhesions and extent of uterine occlusion, and ranged from a term pregnancy rate of 81.3% in patients with mild disease to 31.9% in patients with severe disease.
Although early diagnosis and treatment of intrauterine adhesions seem to improve prognosis, the therapeutic outcome after hysteroscopic division of adhesions has surpassed any blind treatment, adding precision in the re-establishment of normal symmetry to the uterine cavity, and avoiding unnecessary trauma to the rest of the endometrium (Table 5).
Table 5. Hysteroscopic lysis of intrauterine adhesions
Reproductive outcome | ||||||
Author | No. patients | Medium | Technique | Menses NL No. (%) | Pregnancy No. (%) | Term No. (%) |
Levine and Neuwirth (1973) | 10 | Hyskon | Flexible scissors | 5 (50) | 2 (20) | — |
Edstrom (1974) | 9 | Hyskon | Biopsy forceps | 2 (22) | 1 (11) | 1 (11) |
Siegler and Kontopoulos (1981) | 25 | CO2 | Target abrasion/scissors/ | 13 (52) | 11 (44) | 12 (44.4) |
March and Israel(1985) | 38 | Hyskon | Flexible scissors | 38 (100) | 38 (100) | 34 (79.1) |
Neuwirth et al. (1982) | 27 | Hyskon | Scissors alongside | 20 (74) | 14 (51.8) | 13 (48.1) |
Sanfilippo et al. (1982) | 26 | CO2 | Curettage | 26 (100) | 6 (100) | 3 (50) |
Hamou et al. (1983) | 69 | CO2 | Target abrasion | 59 (85.5) | 20 (51.3) | 15 (38.4) |
Sugimoto et al. (1984) | 258 | Hyskon/normal saline | Target abrasion/ Kelly forceps | 180 (69.7) | 143 (76.4) | 114(79.7) |
Wamsteker (1984) | 36 | Hyskon | Scissors/biopsy | 34 (94.4) | 17 (62.9) | 12 (44.4) |
Friedman et al. (1986) | 30 | Hyskon | Resectoscope/scissors | 27 (90) | 24 (80) | 23 (76.6) |
Zuanchong and Yulian (1986) | 70 | Normal saline | Biopsy forceps/flexible scissors | 64 (84.3) | 30 (85.7) | 17 (48.5) |
Valle and Sciarra (1988) | 187 | D5 W/Hyskon | Flexible/semirigid/rigid scissors | 167 (89.3) | 143 (76.4) | 113 (79.7) |
Lancet and Kessler (1988) | 98 | Hyskon | Flexible scissors/ electrosurgery | 98 (100) | 86 (87.8) | 77 (89.5) |
Pabuccu et al (1999) | 40 | Glycine | Murphy probe scissors | 33 (82.5) | 27 (67.5) | 23 (57.5) |
Feng et al. (1999) | 365 | Dextrose 5% | Biopsy forceps/scissors | 294 (83.7) | 156 (83.8)† | 145 (92.9) |
Totals | 1298 | 1060 (87.5) | 718 (72.3) | 603 (87.2) | ||
*NI, Normal
†Of 186 desiring pregnancy
Modified from Siegler AM, Valle RF, Lindemann HJ et al: Therapeutic Hysteroscopy: Indications and Techniques, Ch 6, p 103. St Louis, CV Mosby, 1990
Polyps and Submucous Leiomyomas
Although benign tumors of the endometrium or the muscle seldom cause infertility, those located in the uterine cavity may interfere with nidation or appropriate growth and development of an established pregnancy. Polyps may be removed accidentally at curettage or exploration with forceps. To establish a definite diagnosis and location of a polyp, hysteroscopy is mandatory. Assurance that the polyp has been removed completely can only be offered by the hysteroscope, however (Fig. 19).
Most submucous leiomyomas are symptomatic, generally causing excessive uterine bleeding. Their removal is best accomplished by hysteroscopy, with transection of the pedicle in those that are pedunculated allowing subsequent removal of the myoma, or systematic shaving of sessile leiomyomas that are partially intramural, using the resectoscope and a cutting loop. When significant distortion of the uterine cavity is caused by these leiomyomas on hysterosalpingography, a postoperative evaluation 2 to 3 months after resection is useful by repeating the hysterosalpingogram and assessing the re-establishment of uterine cavity symmetry (Fig. 20).31, 32, 33, 34 Helpful adjuncts in the preoperative evaluation of patients with submucous leiomyomas are vaginal sonography and the use of gonadotropin-releasing hormone (GnRH) analogues. Vaginal sonography can help detect intramural leiomyomas left behind, and assess the penetration of the submucous leiomyoma in the uterine wall. The use of GnRH analogues is helpful in controlling the excessive bleeding and preparing the uterine cavity by atrophying the endometrium for best visualization during surgery. Additionally, the leiomyoma may become less vascular and may also decrease in size, making the hysteroscopic surgery easier (Table 6).35
Table 6. Hysteroscopic myomectomy for abnormal bleeding
Type of myomas | |||||||||
Author | No. patients | Pedunculated | Sessile | Method | IUD | E/P | Antibiotics | Cure (%) | Recurrent (%) |
Haning et al. (1980) | 1 | — | + | Resectoscope | — | + | + | 1 | — |
DeCherney and Polan (1983) | 8 | + | + | Resectoscope | Foley | + | + | 8 | — |
Neuwirth (1983) | 28 | + | + | Resectoscope | Foley | + | + | 17 (60.7) | 8 (28.5) |
Lin et al. (1986) | 13 | + | — | Resectoscope (9) Rigid scissors (4) | Foley | + | + | 9 (69.2) | 4 (30.7) |
Hallez and Perino (1988) | 300 | + | + | Resectoscope | + | + | + | 299† | — |
Baggish (1989) | 23 | + | + | Nd:YAG laser | Foley (5 patients) | — | + | NR* | NR* |
Valle (1990) | 52 | + | — | Semi-rigid scissors | — | — | — | 52(100.0) | NR* |
Donnez, et al. (1990) | 60 | 48 | 12 | Nd:YAG laser | — | — | — | 48(80.0)§ | 12 (20.0) |
Loffer (1990) | 53 (10 were polyps) | 18 | 25 (2 had 2 procedures) | Resectoscope | NR* | — | — | 40 (93.0) | 3(6.9) |
Corson and Brooks (1991) | 92 | 92 | — | Resectoscope | NR* | — | + | 65 (81.2)‡ | 15 (18.7)‡ |
Derman et al. (1991) | 94 | 94 (2 intraoperative laparotomies) | — | Resectoscope | Rubber balloon | + | + | 69 (75.0) | 23 (24.5) |
Wamsteker et al. (1993) | 51 | 25 | 26 (several patients had 2–3 procedures) | Resectoscope | — | — | + | 48 (94.1) | 3 (5.9) |
Emanuel et al. (1999) | 285 | 73 | 266 | Resectoscope | — | — | + | 225 (78.8)§ | 41 (14.4) |
Totals | 1040 |
|
|
|
|
|
| 881 (81.2) | 109 (10.5) |
*IUD, intrauterine device; E/P, estrogen/progesterone; NR, not reported
†1 patient required laparotomy
‡ From 80 patients
§17 lost to follow-up
Modified from Siegler AM, Valle RF: Therapeutic hysterocopy procedures. Fertil Steril, 50:68, 1988.
Tubal Cornual Occlusion
About 30% of infertile women have fallopian tube obstructions causing infertility. Although 10–20% of women demonstrate cornual tubal occlusion in their evaluation by hysterosalpingography, many of these occlusions are due to physiologic tubal spasms and must be evaluated by laparoscopy under general anesthesia.13, 14, 36, 37, 38 In a significant number of patients with cornual tubal occlusion demonstrating occlusion at laparoscopy, no fibrosis is found on microsurgical tubal reconstruction, only obstruction by debris or proteinaceous material plugging the tubal lumen. In fact, Sulak and coworkers39 described an amorphous material present in the tubal lumen at histopathology in 6–18 (33%) patients operated for proximal fallopian tubal occlusion. Three patients (17%) had tubes with normal anatomy and no occlusion. Seven of eighteen patients (39%) had tubal occlusion by fibrosis or salpingitis isthmica nodosa on histopathological evaluation: Over 50% of patients who had surgery and underwent histopathological evaluations demonstrated pseudo-occlusions or obstructions produced by debris or thick mucous tissue. For these reasons, tubal cannulation, begun in the late 1960s and early 1970s, was revived in the early 1980s.40, 41, 42, 43, 44 Better, softer, and thinner catheters were introduced by manufacturers based on experience with angiographic techniques using coaxial catheters, and tubal cannulation was made easier, safer, and more reproducible.39 The important elements in this procedure are a 3-French soft catheter with a soft wire-guide of less than 0.5 mm diameter. A 5-French co-axial catheter can be used to guide these two elements. The procedure should be performed in the early follicular phase when the endometrium is thin and no significant debris is present in the uterine cavity. Concomitant laparoscopy is used to assess tubal patency and to aid in the cannulation procedure. The wire guide is passed into the tubal lumen and the 3-French catheter then is guided over the wire guide, bypassing the intramural portion; the wire guide is removed and indigo carmine is injected directly through the 3-French catheter. An assistant using the laparoscope assesses tubal patency. Patients who fail tubal cannulation are candidates for microsurgical tubal reconstructions on the assumption that the occlusion is fiberoptic. Patency after hysteroscopic tubal cannulation is 72–92% and intrauterine pregnancy approaches 50%.43 Most tubal cannulations can be performed using the rigid hysteroscope. The new flexible operating hysteroscopes, which are steerable and can be directed toward the uterotubal cones, are particularly helpful in small uteri with deeply recessed uterotubal cones (Fig. 21; see Color Plate 1C through G) (Table 7).
|

Table 7. Hysteroscopic cannulation for proximal tubal obstruction
Author | No. patients/failed | No. tubes/failed | Catheter | Complications(perforation) | Pregnancies |
Confino et al. (1986) | 1/0 | 1/0 | Balloon | 1 | — |
Daniell and Miller (1987) | 1/0 | 1/0 | Urological | 1 | 1 |
Sulak et al. (1987) | 2/0 | 4/0 | Epidural | 0 | 1 |
Huang Yu-Lian et al. (1988) | 78*/0 | — | Epidural | 0 | 46 |
Confino et al. (1988) | 12/5 | 23/14 | Balloon | 3 | 2 |
Novy et al. (1989) | 10/1 | 12†/1 | Cornual coaxial set | 1 | 2 |
Deaton et al. (1990) | 11/4 | 18/5 | Urological | 2 | 6 (3 ectopics) |
Lin et al. (1990) | 10/0 | 18/2 | Urological | — | 5 (1 ectopic) |
Flood and Grow (1993) | 27/3 | 46/10 | Cornual coaxial set | 4 | 15 |
Valle (1994) | 63/11 | 120/19 | Cornual coaxial set | 2 | 27 (1 ectopic) |
Total | 215/24 (11/1%) | 244/61 (25.0%) |
| 14 (6.5%) | 105 (49.7%) |
*15 patients refused additional procedures.
†Some performed under fluoroscopy
Vaucallie T, Schmidt EH: The uterotubal junction. A proposal for classifying its morphology as assessed with hysteroscopy. J Reprod Med 33:624, 1988
Impacted and Misplaced Intrauterine Foreign Bodies
An intrauterine foreign body such as a forgotten intrauterine device (IUD) will interfere with fertility. This type of foreign body usually is detected by sonography, but fragments of a broken IUD may remain unnoticed. Additionally, bony fragments from previous late first-trimester or second-trimester abortions can remain in the uterine cavity or form osseous metaplasia acting as osteoblastic grafts. These formations can impair fertility by acting as a foreign body. Because blind removal of this type of foreign body is difficult, hysteroscopy is used to aid in proper complete removal. Patients will assume fertility following these procedures. It is important, nonetheless, to add sonography in the evaluation of these patients, should fragmented IUDs or bony fragments have penetrated the myometrium (see Color Plate 1J and K).45, 46
Hysteroscopy and New Reproductive Technologies
Hysteroscopy can be used as a platform to invade the fallopian tubes; it can be used for intratubal insemination and for delivery of gametes and zygotes, procedures that with refinements in technology may become simpler, less invasive alternatives to laparoscopy.47 The endometrial changes occurring throughout the menstrual cycle can be explored visually, with added magnification, and may eventually help to determine appropriate endometrial maturation and receptivity for embryo transfers.48 Similarly, the cumulative pregnancy rates in patients who had normal hysteroscopic examinations before embryo transfers seem to be significantly better than those in women in whom some abnormalities are detected. This suggests the need for better assessment of the uterine cavity before embryo transfers are performed.47, 48
Hysteroscopy and Ectopic Gestations
Evaluation of the patient with a possible ectopic pregnancy has been greatly facilitated by the use of quantitative human chorionic gonadotropin (hCG) titration and abdominal and vaginal ultrasound. Interest has arisen in using less invasive methods to treat ectopic pregnancies, particularly with methotrexate. This method requires systematic administration of the drug, and produces frequent side effects. Alternative methods of delivering the methotrexate locally used laparoscopic guidance, sonography, and blind tubal cannulations. The hysteroscope remains another alternative, particularly for pregnancies located at the proximal tubal openings and for confirming the pregnancy location determined by ultrasound. This approach may be expanded to include selected patients with early ectopic pregnancies, and women desirous of further fertility who have β-hCG levels of less than 1400 mLU/mL.49
Hysteroscopy can be useful in patients who have flattened or not decreasing levels of β-hCG; in patients in whom ultrasound does not provide information of the location of the pregnancy to rule out early threatening or incomplete abortions; and in determining the possibility of an ectopic gestation when the uterine cavity is completely normal.50
TIMING OF HYSTEROSCOPY
The best time to perform hysteroscopy is in the early follicular phase to avoid the increased endometrial thickness debris and mucus that can impair visualization. Office hysteroscopy should always be performed at the early follicular phase to obtain optimal visualization. Diagnostic hysteroscopy may be combined with laparoscopy and therefore performed in the luteal phase of the menstrual cycle, but care must be taken to avoid abrading the endometrium during the procedure, causing unnecessary trauma. Although laparoscopy and hysteroscopy are performed concomitantly, we prefer to introduce the laparoscope without cervical or uterine manipulation first. Once the laparoscope is in place, then the cervix is grasped with a tenaculum and the endocervical canal and uterine cavity systematically evaluated with the hysteroscope. Unexpected pathology of the uterus and fallopian tubes may be detected by laparoscopy. At the completion of the hysteroscopic observation, chromopertubation is performed through the operating channel of the hysteroscope. When unilateral tubal occlusion is diagnosed, selective chromopertubation is performed using a small polyethylene catheter placed at the uterotubal junction 4 to 5 mm inside the lumen and indigo carmine is directly injected through this catheter to evaluate tubal patency.5 The concomitant use of laparoscopy and hysteroscopy in selected patients offers the most complete examination of the genital tract to rule out and treat cervical, uterine, and tubal peritoneal factors that may affect fertility. Therapeutic hysteroscopy should be undertaken only in the early follicular phase to facilitate surgery (see Color Plate 1H, J, K).5,16,51
CORRELATION OF HYSTEROSCOPY, HYSTEROSALPINGOGRAPHY, AND ULTRASONOGRAPHY
Hysteroscopy and hysterosalpingography are essentially luminal studies, or techniques designed to evaluate the different channels and spaces of the uterus. Hysterosalpingography permits evaluation of the endocervical canal, uterine cavity, and fallopian tubes; however, the evaluation is an indirect one using radiopaque substances that fill these natural passages and permit visualization on x-rays, either by fluoroscopy or permanent-ray pictures. Hysteroscopy provides direct visualization of the endocervical canal and uterine cavity and can also offer evaluation of the uterotubal junctions, but does not provide direct evaluation of the fallopian tubes. Hysteroscopy (by providing direct visualization) is more precise than hysterosalpingography, but it cannot replace the hysterographic examination. These procedures complement each other in the evaluation of the infertile patient. Because hysteroscopy offers appraisal only of topographic details, it cannot provide information on the uterine walls and evaluation of the uterus as an organ, and this also applies to hysterosalpingography. A technique that provides such information is ultrasonography by the abdominal or vaginal route. The new high-frequency transducers provide evaluation of the uterine walls that is particularly useful in the evaluation of lesions that infiltrate the myometrium, such as purely intramural leiomyomas. This procedure therefore adds three-dimensional evaluation of the uterus and, in combination with hysteroscopy and hysterosalpingography, permits a complete evaluation of this organ.11,12,52
Vaginal sonography is useful to screen patients for endometrial abnormalities, but it cannot provide accurate diagnosis; therefore, patients require a hysteroscopy and hysteroscopy-directed biopsies. In the evaluation of uterine leiomyomas, sonography can offer information about intramural leiomyomas not visible by endoscopy or diagnosed by the hysterosalpingogram. The size, location, and number of leiomyomas can be assessed, as well as the relationship of leiomyomas to the endometrial stripe, and the thickness of myometrial involvement in sessile leiomyomas can be measured. This information becomes most valuable when planning transcervical hysteroscopic resection of submucous leiomyomas.52
Ultrasonography is also valuable in evaluating the response of leiomyomas to medical treatment, specifically GnRH analogues, because these medications decrease the size of the leiomyoma, particularly after 3 months of administration.35 Combining the three methods of evaluation complements the overall evaluation of the uterus, and is especially valuable in the presurgical evaluation of uterine leiomyomas.
SUMMARY
Uterine factors account for less than 10% of all infertility. The hysterosalpingogram has been the most useful method of evaluation as the initial screening test. Because of the high false-positive yield of the hysterosalpingogram, hysteroscopy becomes a valuable adjunct in the evaluation of patients with abnormal hysterograms, permitting an accurate diagnosis and sometimes direct treatment. Hysteroscopy is used as a therapeutic method in many conditions that may affect fertility, such as symptomatic uterine septum, intrauterine adhesions, endometrial polyps and submucous leiomyomas, and cornual fallopian tube occlusion. The addition of ultrasonography complements the overall evaluation of the uterus and in selected patients becomes a useful adjunct to infertility evaluation.
The main indication for hysteroscopy in infertile patients is the abnormal or ambiguous hysterogram. In conjunction with hysterosalpingography, it adds accuracy and precision in the evaluation of uterine cavity and endocervical canal, ruling out factors that may affect fertility.
REFERENCES
Wallach EE: Evaluation and management of uterine causes of infertility. Clin Obstet Gynecol 22: 43, 1979 |
|
Valle RF: Clinical management of uterine factors in infertile patients. Semin Reprod Endocrinol 3: 149, 1985 |
|
Mohr J, Lindemann HJ: Hysteroscopy in the infertile patient. J Reprod Med 19: 161, 1977 |
|
Valle RF: Hysteroscopy in the evaluation of female infertility. Am J Obstet Gynecol 137: 425, 1980 |
|
Valle RF: How endoscopy aids the infertility work-up. Contemp Ob/Gyn 3: 191, 1984 |
|
Siegler AM: Hysterosalpingography. Fertil Steril 40: 139, 1983 |
|
Vaile RF, Sciarra JJ: Current status of hysteroscopy in gynecologic practice. Fertil Steril 32: 619, 1979 |
|
Siegler AM: Hysterography and hysteroscopy in infertile patients. J Reprod Med 18: 148, 1977 |
|
Kessler I, Lancet M: Hysterography and hysteroscopy: A comparison. Fertil Steril 46: 709, 1986 |
|
Fayez JA, Mutie G, Schneider PJ: The diagnostic value of hysterosalpingography and hysteroscopy in infertility investigation. Am J Obstet Gynecol 156: 558, 1987 |
|
Taylor PJ: Correlations in infertility: Symptomatology hysterosalpingography, laparoscopy, and hysteroscopy. J Reprod Med 18: 339, 1977 |
|
Snowden EU, Jarrett JC, Dawood MY: Comparison of diagnostic accuracy of laparoscopy, hysteroscopy, and hysterosalpingography in evaluation of female infertility. Fertil Steril 41: 709, 1984 |
|
Valle RF: Hysteroscopy in the evaluation of infertility. In Winfield AC, Wentz AC (eds): Diagnostic Imaging in Infertility, pp. 117–150, 2nd ed. Baltimore, Williams & Wilkins, 1992 |
|
March CM: Hysteroscopy for infertility. In Baggish MS, Barbot J, Valle RF (eds): Diagnostic and Operative Hysteroscopy: A Text and Atlas, pp. 333–352, 2nd ed. St Louis, Mosby, 1999 |
|
Grow DR, Coddington CC, Flood JF: Proximal tubal occlusion by hysterosalpingogram: A role for falloposcopy. Fertil Steril 60: 170, 1993 |
|
Shalev J, Meizner I, Bar-Hava I et al: Predictive value of transvaginal sonography performed before routine diagnostic hysteroscopy for evaluation of infertility. Fertil Steril 73: 412, 2000 |
|
Valle RF: Hysteroscopy: Diagnostic and therapeutic applications. J Reprod Med 20: 115, 1978 |
|
Valle RF: Therapeutic hysteroscopy in infertility. Int J Fertil 29: 143, 1984 |
|
Rock JA, Zacur MA: The clinical management of repeated early pregnancy wastage. Fertil Steril 39: 23, 1983 |
|
Jones HW, Jones GES: Double uterus or an etiologic factor in repeated abortions: Indications for surgical repair. Am J Obstet Gynecol 65: 325, 1953 |
|
Tompkins P: Comments on the bicornuate uterus and twinning. Surg Clin North Am 42: 1049, 1962 |
|
Ruge P: Einen Fall yon Schwangerschaft bei uterus septus. Geburtshilfe Gynakol 10: 141, 1884 |
|
Daly DC, Waiters CA, Soto-Albors CE et al: Hysteroscopic metroplasty: Surgical technique and obstetric outcome. Fertil Steril 39: 623, 1983 |
|
Valle RF, Sciarra JJ: Hysteroscopic treatment of the septate uterus. Obstet Gynecol 676: 253, 1986 |
|
DeCherney AH, Russell JB, Graebe RA et al: Resectoscopic management of mullerian fusion defects. Fertil Steril 45: 726, 1986 |
|
Siegler AM, Valle RF: Therapeutic hysteroscopic procedures. Fertil Steril 50: 685, 1988 |
|
Hassiakos DK, Zourlas PA: Transcervical division of the uterine sepia. Obstet Gynecol Surv 45: 165, 1990 |
|
Choe JK, Baggish MS: Hysteroscopic treatment of septate uterus with Neodymium-YAG laser. Fertil Steril 57: 81, 1992 |
|
Klein SM, Garcia CR: Asherman's syndrome: A critical and current review. Fertil Steril 24: 722, 1973 |
|
Valle RF, Sciarra JJ: Intrauterine adhesions: Hysteroscopic diagnosis, classification, treatment, and reproductive outcome. Am J Obstet Gynecol 158: 1459, 1988 |
|
Valle RF: Hysteroscopic removal of submucous leiomyomas. J Gynecol Surg 6: 89, 1990 |
|
Loffer FD: Removal of large symptomatic intrauterine growths by the hysteroscopic resectoscope. Obstet Gynecol 76: 836, 1990 |
|
Corson SL, Brooks PG: Resectoscopic myomectomy. Fertil Steril 55: 1041, 1991 |
|
Derman SG, Rehnstrom J, Neuwirth RS: The long-term effectiveness of hysteroscopic treatment of menorrhagia and leiomyomas. Obstet Gynecol 77: 591, 1991 |
|
Perino A, Chianchiano N, Petronio M: Role of leuprolide acetate depot in hysteroscopic surgery: A controlled study. Fertil Steril 59: 507, 1993 |
|
Vancallie T, Schmidt EH: The uterotubal junction. A proposal for classifying its morphology as assessed with hysteroscopy. J Reprod Med 33: 624, 1988 |
|
Menken FC: Endoscopic observations of endocrine processes and hormone changes. In Albrecht FR, Sanchez JR, Willowitzer H (eds): Simposio Esteroids Sexuals, pp 276–281, Museo Nacional, Bogota, Colombia, June 26, 1968. Berlin, Saladruck, 1969 |
|
Quinones-Guerrero R, Alvarado-Duran, Aznar-Ramos R: Tubal catheterization: Applications of a new technique. Am J Obstet Gynecol 114: 674, 1972 |
|
Sulak PJ, Letterie GS, Coddington CC et al: Histology of proximal tubal occlusion. Fertil Steril 48: 437, 1987 |
|
Thurmond AS, Novy M, Uchida BT, Rosch J: Fallopian tube obstruction: Selective salpingography and recanalization. Radiology 163: 511, 1987 |
|
Confino E, Friberg J, Gleicher N: Preliminary examine with transcervical balloon tuboplasty. Am J Obstet Gynecol 159: 370, 1988 |
|
Novy MJ, Thurmond AS, Patton P et al: Diagnosis of cornual obstruction by transcervical fallopian tube cannulation. Fertil Steril 50: 434, 1988 |
|
Thurmond AS, Novy MJ: Transcervical fallopian tube catheterization for management of proximal tubal obstruction. In Winfield AC, Wentz AC (eds): Diagnostic Imaging in Infertility, pp 192–207. Baltimore, Williams & Wilkins, 1992 |
|
Valle RF: Future growth and development of hysteroscopy. Obstet Gynecol Clin North Am 15: 111, 1988 |
|
Taylor PJ, Hamou J, Mencaglia L: Hysteroscopic detection of heterotopic intrauterine bone formation. J Reprod Med 33: 337, 1988 |
|
Valle RF: Intrauterine bone formation causing infertility. OBG Management 6: 11, 1999 |
|
Bordt J, Belkien L, Vancaillie T et al: Ergebnisse diagnosfischer Hysteroskopien in einem IVF/ET Programm. Geburtshilfe und Frauenheilkd 44: 813, 1984 |
|
Shamma FN, Lee G, Gutmann JN et al: The role of office hysteroscopy in in vitro fertilization. Fertil Steril 58: 1237, 1992 |
|
Goldenberg M, Bider D, Oelsner G et al: Treatment of interstitial pregnancy with methotrexate via hysteroscopy. Fertil Steril 58: 1234, 1992 |
|
Loffer FD: Hysteroscopy in differentiating ectopic pregnancy from other nonviable pregnancies when serum hCG titers remain below the threshold of ultrasound diagnosis. J Gynecol Surg 8: 165, 1992 |
|
Taylor PJ, Leader A: Laparoscopy combined with hysteroscopy in the management of the ovulatory infertile female. Int J Fertil 28: 59, 1983 |
|
Cohen LS, Valle RF: Role of vaginal sonography and hysterosonography in the endoscopic treatment of uterine myomas. Fertil Steril 73: 197, 2000 |