Induced Abortion: Epidemiologic Aspects
Authors
INTRODUCTION
Induced abortion occurs at least occasionally in all societies and is common in those with low fertility. Even during the 19th century when abortion was illegal, its incidence in the United States and parts of Europe was high enough to be a factor in the declining fertility rates. It is only within the past 60 years, however, that abortion in Western countries and some developing countries has changed from being predominantly illegal and unsafe to being one of the most commonly performed and intensely studied surgical procedures in obstetric and gynecologic practice.
Epidemiological data on legal abortion come from several sources: registration required in many countries and jurisdictions; administrative records of services provided; surveys of abortion providers; and population surveys. Estimates of abortions performed in countries with restrictive laws can be projected from the number of women with abortion complications treated in hospitals or from population surveys but are generally less reliable.
THE LEGAL STATUS OF ABORTION
Among the countries of the world, the legal status of induced abortion ranges from complete prohibition to elective abortion at the request of the pregnant woman.1 The situation in 2013 can be summarized as follows. Approximately 26% of the world's 7 billion people lived in countries where abortion was prohibited without exception or where it was permitted only to save the life of the pregnant woman. These included most of the Muslim countries of Asia, almost two-thirds of the countries of Latin America, a majority of the countries of Africa, and one country in Europe (Ireland).* Approximately 14% lived under statutes authorizing abortion on broader medical grounds, such as to avert a threat to the woman's physical or mental health rather than to her life, and sometimes on eugenic, or fetal, indication (known genetic or other impairment of the fetus or increased risk of such impairment) or juridical indication (e.g. rape, incest) as well. Twenty-two per cent resided in countries where abortion is permitted to protect a woman's health and where social factors, such as inadequate income, substandard housing, and unmarried status, could be taken into consideration in the evaluation of the threat to the woman's health (social–medical indication); or where adverse social conditions alone, without reference to health, could justify termination of pregnancy. Important countries in this group were Great Britain, India, and Japan.
Countries allowing abortion on request without specifying reasons—sometimes limited to the first trimester of pregnancy—accounted for 39% of the world's people. Abortions on medical grounds are usually permitted beyond the gestational limit prescribed for elective abortions, and parental consent may be required if the pregnant woman is a minor. This category includes a heterogeneous list of countries: Austria, Canada, the People's Republic of China, Cuba, Denmark, France, Germany, Italy, The Netherlands, Norway, Singapore, South Africa, Spain, the republics of the former Soviet Union, Sweden, Tunisia, Turkey, the United States, Uruguay, Vietnam, and most of the formerly socialist republics of Eastern and Central Europe.
Several of the categories in the preceding paragraphs cover a range of situations. A statute authorizing abortion to avert a threat to the pregnant woman's mental health may be interpreted strictly or may allow most women to obtain abortions. Social indications are usually defined or interpreted broadly to allow almost any woman to terminate a pregnancy within gestation limits, as in Great Britain, India, and Japan.
The abortion statutes of many countries are not strictly enforced, and occasional abortions on medical grounds are probably tolerated in almost all countries. It is well known that in some countries with restrictive laws, abortions can be obtained openly and without interference from the authorities when performed by private physicians, as in Korea and parts of South America. Abortions may even be performed in public hospitals, as in Cuba before their legalization in 1979 and in Mozambique. Conversely, legal authorization of abortion does not guarantee that the procedure is actually available to all women who may want their pregnancies terminated. Lack of medical personnel and facilities, and conservative attitudes among physicians may effectively curtail access to abortion, especially for economically or socially deprived women, as in parts of Ghana, India, and the United States.
In some countries, restrictions are at least occasionally enforced on women as well as providers. In Chile, women are reported to be serving prison sentences for having an abortion, women accused of abortion are incarcerated in El Salvador,2 and in Nepal many women were incarcerated before the law was liberalized in 2002.3
Where abortion is permitted on request or on broad grounds, other governmental policies may affect its availability. Almost all developed countries cover all or most of the cost of abortion in their national health services or insurance,4 the major exception being the United States, where states vary widely in their abortion policies. The more liberal states cover abortion services under their public insurance for low-income women (Medicaid), and for other women coverage is usually provided by private insurance. In the most conservative states, Medicaid excludes abortion coverage except in cases of rape, incest, and threat to the life of the pregnant woman, and private insurance is prohibited from paying for abortion. In the United States, studies have found that having to pay for abortion services without financial help means that about one-quarter of poor women who would have abortions are unable to do so.5, 6
Many countries have other restrictions that affect women seeking abortions. These include a waiting period between counseling or first provider contact and the procedure, required pre-procedure counseling with specified content, and parental consent or notification for minors. Four countries with relatively unrestrictive laws require spousal authorization for married women.†1 These provisions reflect moral or religious opposition to abortion, concern that women might act impulsively and later regret their decision, and, in a few cases, concern about low birth rates. Abortions for sex selection are outlawed in China and Nepal because of concerns about an unbalanced sex ratio of births.
Other restrictions on abortion affect the facilities and clinicians who provide the services. These include requiring providers to be physicians, requiring them to have certain qualifications such as specified training or hospital privileges, allowing abortions to be performed only in hospitals or in qualified facilities, and limiting the advertising of abortion services. In most cases, these provisions reflect attempts to ensure the safety of abortion, sometimes based on outdated assumptions about the risks of the procedure. In the United States, apparently in an attempt to make services less accessible and more expensive, some states allow abortions to be performed only in ambulatory surgery centers or hospitals, even early abortions performed by medication (mifepristone). A few states allow abortions to be performed only by physicians with admitting privileges in local hospitals. Attempts to require all abortions to be performed in hospitals were found by the Supreme Court to be unconstitutional because they restrict access without contributing to safety. The effects of restricting services are felt mainly by low-income women.
CHANGES IN LAWS
During the 19th century, abortion became illegal virtually worldwide. Motivations for restrictive laws included the desire to protect women’s health from what was then a dangerous procedure, efforts to discourage illicit sexual behavior, and the influence of religious authorities. In the first half of the 20th century, abortion remained illegal except briefly in the Soviet Union and in a few other small areas. The legalization movement began in earnest in the Soviet Union in 1955, when the law was changed to permit first-trimester abortion on request. The aims of the new law were “the limitation of harm caused to the health of women by abortions carried out outside of hospitals” and to give “women the possibility of deciding themselves the question of motherhood.”7 Most of the socialist countries of Eastern Europe followed in 1956–57, as did China in 1957.
In Western Europe, the United Kingdom, excluding Northern Ireland, liberalized its law in 1967, followed by Canada in 1969, and the other major European countries except Belgium,‡ Ireland and Portugal in the 1970s and 1980s. India changed its law in 1971 to allow abortion under a variety of conditions, including contraceptive failure. In 1973, abortion became permissible on request in the United States under the Supreme Court decision Roe v. Wade. However, most countries in Africa and Asia retained prohibitions established under colonial laws.
The worldwide trend toward liberalization of abortion laws that was evident in the 1960s through the 1980s has continued in recent years, although at a much slower pace. From 1998 through 2007, laws were liberalized in 14 countries with populations of 1 million or more and also in Mexico City. During this period, new restrictions were imposed in El Salvador and Nicaragua.3
Since 2007, Luxembourg, Spain, Uruguay, and two states in Australia have changed their laws to permit abortion on request, and Kenya, Lesotho, Mauritius, and Hong Kong have liberalized their laws to a lesser extent. No country has made the grounds for first-trimester abortion more restrictive, but Russia limited the social indications for abortions past 12 weeks.** Some states in the United States have made accessing abortion services more difficult, although in theory the procedure remains legal without limits as to reason.
In most countries, the laws were changed by means of legislation but in a few, including the United States and Canada, courts found that restrictive laws violated the constitutional rights of women. On the other hand, liberal laws have occasionally been found to violate constitutional protections for fetuses and embryos. In some jurisdictions, courts and accepted practice gradually expanded the interpretation of restrictive laws to allow abortions under more circumstances. In a few countries, including Greece, The Netherlands and Taiwan, abortion became widely accepted and practiced despite restrictive laws, which were ultimately changed to reflect practice.
Major reasons advanced by advocates of less-restrictive legislation in matters of abortion, and especially of abortion on request, have been considerations of public health (to combat illegal abortion with its associated morbidity and mortality); social justice (to give poor women access to abortion previously available only to the well-to-do); and women's rights (to secure a postulated right of all women to control their own bodies and reproduction). A desire to curb population growth, in the interest of economic and social development, has been an explicit reason for the adoption of nonrestrictive abortion policies in a few countries, such as Singapore, Tunisia, and China, and may have been an underlying reason for policy changes in some other countries, including India and Bangladesh. The majority of countries permitting abortion at the request of the pregnant woman or on broadly interpreted social indications, however, have low birth rates, and some of them actively pursue pronatalist population policies.
Opposition to the liberalization of abortion laws has come traditionally from conservative groups, mainly on moral and religious grounds, with the Roman Catholic Church being the most vigorous and articulate. Antiabortion policies are also favored by fundamentalist Protestants and Muslims and by some Orthodox Jews. The desire for higher birth rates led to restrictive legislation in a few instances, especially in Eastern and Central Europe during the 1960s and 1970s, though legal services were still available to most women who sought them except in Romania. In recent years, Eastern Orthodox churches and concerns about population declines in former Soviet-bloc countries have combined to create pressure for restrictions and were responsible for the new limits on second-trimester abortion in Russia. Abortion has become one of the most emotional and divisive political issues in a number of countries in recent years.
INCIDENCE OF LEGAL ABORTION
The number of pregnancies terminated each year by induced abortion throughout the world cannot be determined exactly. A recent estimate is that approximately 44 million abortions take place each year, about half illegal. The estimated abortion rate for 2008 was 28 abortions per 1000 women in the world aged 15–44, and 21% of pregnancies, including the estimated number of miscarriages, were ended by induced abortion. The worldwide abortion rate has changed little in recent years.8
The abortion rate was about 24 per 1000 women in developed countries and 29 in developing countries (Table 1).
Table 1. Estimated abortions per 1000 women aged 15–44, by region, 2008
| Region | Rate |
| World | 28 |
| Developed countries* | 24 |
| Developing countries | 29 |
| Africa | 29 |
| Asia | 28 |
| Europe | 27 |
| Latin America | 32 |
| Northern America | 19 |
| Oceania | 17 |
*Europe, North America, Australia, Japan and New Zealand
Source: Reference8
The rate may be higher in developing countries (29/1000) than in developed ones because couples’ desires to time and limit the number of children have increased more rapidly than the availability of family planning services and the acceptance of contraception. Abortion rates are higher in areas with higher rates of unmet need for contraception.9
Abortion rates vary little among the regions of the world except in northern America and Oceania, where they are lower. Within Europe, however, rates vary by subregion, being lowest in Western Europe, where the rate is 12 and highest in Eastern Europe, where it is 43. Eastern Europe includes Russia and the former Soviet bloc countries, where historically most contraceptive methods were not widely available and women relied on abortion to limit their family size.
Rates tend to be higher in countries with restrictive laws than where safe abortion services are legally available.8 This is not necessarily because restrictive laws encourage abortion but because almost all countries with restrictive laws are developing areas with lower use of contraception. Legalization of abortion is often accompanied by enhanced family planning programs and efforts to encourage use of contraception. Where abortion is legal, the procedure is often accompanied by contraceptive counseling and supplies, thereby helping to prevent repeat unintended pregnancies.
While it is difficult to estimate the exact level of illegal abortion, it is clear that legally restricting abortion does not necessarily reduce the practice to a low level. A large majority of the residents of Africa and Latin America live where it is virtually impossible to have a legal abortion, yet the abortion rates in those areas are relatively high because women find ways to end their pregnancies through illegal means. An exception is Ireland, where there are few abortions because women can obtain services nearby in Great Britain.
Where abortion is legal and reporting is complete, there is wide variation in the extent to which women rely on pregnancy termination. The highest recorded abortion utilization occurred in Romania in 1965, when the rate reached 252 abortions per 1000 women aged 15–44. This means that one-quarter of reproductive-age women had abortions that year. Among the lowest recorded rates was five per 1000 among residents of The Netherlands in 1985.10 Many of the abortions in The Netherlands were obtained by immigrants; the rate among Dutch-born women was as low as 3.5 per 1000 in some years. The Netherlands had one of the most liberal laws—abortion was permitted on request up to fetal viability—and the service was covered by insurance.
Abortion rates in developed countries with complete data other than in Eastern Europe range from 7 to 21 (Table 2). Rates are higher in some Central and Eastern European countries such as Estonia (30) and Russia (38 based on incomplete reporting). However, these rates have declined sharply since the disappearance of communism as contraceptive methods have become more available. In Estonia, for example, the rate has fallen 46% since 1996.
Table 2. Rate of legal abortions in selected countries with complete reporting, 1996 and 200811
| Country | 2008 | 1996 | % change |
|
|
|
|
|
|
|
| Switzerland | 7 | u | u |
|
| Germany* | 7 | 8 | -13% |
|
| The Netherlands** | 8 | 7 | 14% |
|
| Belgium | 9 | 7 | 29% |
|
| Portugal* | 9 | u | u |
|
| Italy* | 10 | u | u |
|
| Spain | 12 | u | u |
|
| France | 16 | 15 | 7% |
|
| England & Wales*,** | 17 | 16 | 6% |
|
| United States | 20 | 22 | -9% |
|
| Sweden* | 21 | 19 | 11% |
|
| Hungary | 21 | 35 | -40% |
|
| Estonia | 30 | 56 | -46% |
|
*Most recent rate is for 2009, not 2008
**Residents only
Notes: Rate is per 1000 women aged 15-44. u = unavailable
In the United States, the legal abortion rate rose rapidly after the Supreme Court decision in 1973 to a peak of 29 in 1980, changed little through the decade until 1990, then began a long decline to 20 in 2008.12 In that year, 22% of pregnancies (excluding miscarriages) ended in abortion. At 2007 age-specific rates, a cohort of 100 women would have 59 abortions by the time they reach menopause and one-quarter to one-third would have at least one abortion.13 The relatively high US abortion rate is attributable to the elevated rate among racial minorities and Hispanic women.
The large number of abortions in the United States reflects an even larger number of unintended pregnancies. In 2006, an estimated 49% of all pregnancies were unintended; of the unintended pregnancies that ended in birth or abortion, 43% ended in induced abortion.14 The decline in the abortion rate since the early 1990s was concentrated among teenagers and women aged 20–24. Teenagers experienced fewer abortions largely because of improved contraceptive use and secondarily because of delayed initiation of sexual activity15 and a trend toward continuing rather than terminating unintended pregnancies.14
In developing as well as developed countries, abortion rates span a wide range. Currently the highest measured rates are in Azerbaijan and Armenia, with rates of 81 and 54, respectively, measured by population surveys, which usually underestimate rates. Many developing countries lack data or have incomplete reporting, so rates are rarely known. Rates appear to be high in many developing countries because of poorly developed family planning services and traditional cautiousness about contraception. Even China reports 29 abortions per 1000 women of reproductive age despite a well-developed family planning program. Nevertheless it is possible for developing countries to have low rates, an example being Tunisia, where the reported rate is 6 and the actual rate is probably not more than 9.11 Sexual activity before marriage is uncommon in Tunisia and contraceptive services are readily available.
DEMOGRAPHIC PATTERNS
Abortion occurs among women in all population subgroups. Table 3 shows 2008 data for the United States, which is roughly similar to other developed countries and has information on many characteristics of women having abortions. The number of abortions and the abortion rate start at a low level among the youngest women, rise to a peak at 20–24 years (when most women are still unmarried but are sexually active), then decline steadily to a low level among women in their 40s. In countries where premarital sexual activity is uncommon, including many developing countries in Asia and North Africa, the peak abortion age is somewhat older, when women have children but want to delay additional childbearing or want no more children. The pattern of abortion ratios per 100 pregnancies is quite different from that of abortion percentages and rates. In developed countries like the United States, ratios are fairly high among the youngest women, decline progressively to 30–34 years of age, when most women are married and many are building their families, then rise to a higher level among the relatively few pregnancies occurring after age 40. In high-fertility developing countries, abortion ratios usually increase with age.
Table 3. Percentage distribution, rate and ratio of abortions by selected characteristics (United States, 2008)
Characteristic | Percentage distribution | Rate* |
Age of woman (years)13 | ||
<15 | 0.5 | 2.9 |
15–19 | 15.9 | 17.8 |
20–24 | 32.7 | 38.4 |
25–29 | 24.6 | 28.6 |
30–34 | 14.61 | 18.4 |
35–39 | 8.7 | 10.2 |
40 or older | 3.0 | 3.4 |
Marital status16, ‡ | ||
Married | 14.8 | 6.6 |
Cohabiting, not married | 29.2 | 67.1 |
Never-married, not cohabiting | 45.0 | 21.9 |
Previously married, not cohabiting | 11.0 | 25.8 |
Prior births13 | ||
0 | 40.2 | 16.6 |
1 | 27.2 | 31.3 |
2 | 19.1 | 18.2 |
3 | 8.6 | 16.0 |
4 or more | 4.9 | 18.4 |
Race13 | ||
White | 54.7 | 13.8 |
Non-Hispanic white | 33.9 | 10.9 |
Black | 37.8 | 48.2 |
Other | 7.5 | 18.4 |
Hispanic ethnicity13 | ||
Hispanic | 22.0 | 23.8 |
Non-Hispanic | 78.0 | 18.5 |
Family income as % of poverty level16 | ||
<100% | 42.4 | 51.6 |
100–199 | 26.5 | 27.5 |
≥200 | 31.1 | 9.3 |
Religious affiliation16, *** | ||
Protestant Christian | 37.3 | 14.6 |
Roman Catholic | 28.1 | 20.2 |
Other | 7.1 | 23.9 |
None | 27.5 | 30.8 |
Prior induced abortions17 | ||
0 | 55.6 | |
1 | 25.3 | |
2 | 11.1 | |
3 or more | 8.0 | |
Weeks of gestation17, § | ||
<7 | 30.7 | |
7 | 18.1 | |
8 | 14.0 | |
9–13 | 28.6 | |
14–15 | 3.5 | |
16–17 | 2.0 | |
18–20 | 1.9 | |
21 or more | 1.3 | |
Abortion procedure17, ** | ||
Instrumental evacuation ≤13 weeks | 75.9 | |
Instrumental evacuation >13 weeks | 8.5 | |
Medication, ≤8 weeks | 14.6 | |
Medication, >8 weeks | 0.7 | |
Intrauterine instillation | 0.1 | |
Other# | 0.6 | |
*For age <15, denominator is women age 14; for 40+, denominator is women aged 40–44
‡ Separated women are included with married
§ Weeks since onset of last menstrual period
**Some reports indicated more than one method, so total is more than 100%
***Among women aged 18 and older
#Includes hysterotomy, hysterectomy, and procedures reported as 'other'
Whether measured by rates or ratios, in most developed countries and probably in Africa, abortion is more common among unmarried women than among married women, even when age is taken into account. Rates in the United States are highest among unmarried cohabiting women. Cohabiting women are especially at risk of unintended pregnancy because they are sexually active and often want to avoid childbearing or are ambivalent about the possibility of pregnancy. They have the highest abortion rate of any demographic group, which makes them an important target group for family planning services.
Historically, in the United States and in Western European countries, half or more of abortions were obtained by women with no children. In recent years, however, the pattern has changed with the decline in the abortion rate of teenagers and women aged 20–24. Now about 60% of abortion patients have children, and the highest abortion rate is among women with one child. Some of the latter are unmarried, young, exposed to risk of pregnancy, and not well situated to take care of two children. Because many women having abortions are nulliparous and a majority intend to have children in the future, it is of highest priority in providing abortion services to minimize risk to the woman's subsequent reproductive potential.18
Although white women, including Hispanics, made up a majority of women having abortions in 2008, the abortion rate for black women (48 per 1000) was more than three times as high as the rate for white women (14 per 1000), and more than four times the rate of non-Hispanic white women (11 per 1000). This difference reflects a high percentage of unwanted and mistimed pregnancies among economically and socially disadvantaged women rather than a greater propensity to terminate such pregnancies by abortion. Compared with white women, black and Hispanic women have a higher rate of unintended pregnancies; these result in more unplanned births as well as in more abortions.14 The abortion rate of Hispanic women in the United States was between that of white and black women.
In other developed countries as well, abortion rates are often particularly high among immigrants from developing countries. This is the case, for example, in Italy, The Netherlands, and Spain, where the relevant data are available. Most countries have not recorded abortions according to the woman’s country of origin, although such information would help to identify subgroups with high rates of unintended pregnancy.
Abortion rates in the United States are highly associated with income, women living under the poverty level being almost six times as likely to have an abortion in a given year as women above two times the poverty level. This pattern is probably characteristic of other developed countries though possibly less pronounced because income inequality is less severe in most other countries. Special efforts are needed to extend family planning and abortion services to the low-income segments of society.
According to surveys of abortion patients in the United States, women who profess a religious affiliation are less likely to have an abortion than women with no religion. Abortion is more common among Catholic women than among Protestants, despite the strong opposition of the Catholic Church to pregnancy termination. This pattern may reflect in part the concentration of Catholics in urban areas, which generally have higher abortion rates than rural areas and small towns.
The issue of repeat abortion is a matter of concern, especially for those who feel that abortion is unacceptable as a primary method of fertility regulation and should be used only as a backup measure when contraception has failed. Others fear that even minor adverse effects on the outcome of later pregnancies would be cumulated by multiple abortion experiences. In the United States, the percentage of repeat abortions increased for 25 years after legalization, then stabilized. The increase did not reflect a progressive change from contraception to abortion as the primary method of fertility regulation. Rather, it reflected the growing number of women who have had a first legal abortion and, therefore, are at high risk of having a repeat abortion. Most women who have had an abortion are at risk of a repeat unintended pregnancy and abortion because they are sexually active, able to become pregnant, have difficulty using contraceptives effectively, are willing to end an unwanted pregnancy by abortion, and are concentrated in subgroups with high rates of unintended pregnancy. It is therefore important for clinicians to pay special attention to the contraceptive needs of patients with a history of abortion. Today 44% of abortions are repeat procedures and 19% are third or higher order abortions.
The proportion of repeat abortions is lower in most other developed countries and is generally lower where the abortion rate is lower. It tends to be elevated in populations where abortions are concentrated in subgroups, as is the case in the United States, where abortion rates are particularly high among low-income women and minorities.
Women usually have a number of reasons for seeking abortions, more than four reasons on average according to one study. The reasons most commonly reported were that a baby would interfere with work, school, or family responsibilities (74%); lack of financial resources to support a child (73%); and problems in the relationship with her partner or desire to avoid single parenthood (48%). Health reasons were reported by 12% and fear of a possible fetal defect by 13% (although it is likely that few were advised by a physician of such a risk). One per cent of the respondents said the pregnancy was the result of rape or incest.19 A major concern of many women is the well-being of their present and future children.20 More than half of women having abortions practice contraception during the month they become pregnant, although not necessarily correctly and consistently.21
PERIOD OF GESTATION AND METHOD OF ABORTION
One of the most important factors affecting the risk of morbidity and mortality associated with induced abortion is the period of gestation at which the pregnancy is terminated. Although the traditional division has been between abortions in the first trimester and those in the second trimester, experience indicates that this dichotomy is not sufficient because morbidity and mortality increase with the progress of gestation, even within each trimester.
In the United States, more than half (63%) of the abortions take place at or before 8 weeks from the last menstrual period, and an increasing proportion (31% in 2008) are performed before 7 weeks. Medical methods of early abortion by use of mifepristone in combination with the prostaglandin misoprostol are now commonly available. Methotrexate can also be safely used with misoprostol where mifepristone is unavailable, as in Canada, or too costly. In the United States vacuum aspiration, either manual or electric, is sometimes used as early as pregnancy can be detected. Contributing to these developments is the availability in clinics and physicians' offices of sensitive vaginal ultrasound equipment for assessing pregnancy and ensuring that the uterus is empty after the procedure.
One of the most important factors affecting the risk of morbidity and mortality associated with induced abortion is the period of gestation at which the pregnancy is terminated. Although the traditional division has been between abortions in the first trimester and those in the second trimester, experience indicates that this dichotomy is not sufficient because morbidity and mortality increase with the progress of gestation, even within each trimester.
In 2008, 9% of abortions occurred after 13 weeks, including 1% after 20 weeks. Under extraordinary circumstances, abortions may be performed after 24 weeks, often following the discovery of fetal abnormalities. The percentage of later abortions is lower in countries with restrictions on the circumstances in which they are permitted, but in nonrestrictive countries the proportion of abortions past 12 or 13 weeks is generally comparable to the United States. In some developing countries such as India and South Africa, the proportion of later abortions is much higher. The proportion of second-trimester procedures is often high when abortion is first legalized, then declines gradually over time as women become aware of the availability of safe services and the importance of presenting early in pregnancy.
Abortions past 13 weeks occur most frequently among the youngest women, as shown in Fig. 1. The strong inverse association of period of gestation and a woman's age probably reflects the inexperience of the very young in recognizing the symptoms of pregnancy, their unwillingness to accept the reality of their situation, their ignorance about where to seek advice and help, their hesitation to confide in adults, and barriers of cost and distance. In many states, regulations prohibiting abortions for minors without parental consent or notification or a court order, also contribute to delays.
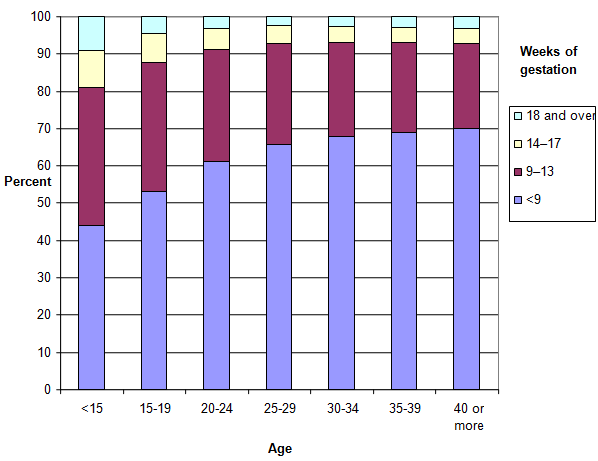 Fig. 1. Legal abortions by woman's age and weeks of gestation, United States, 2008
Fig. 1. Legal abortions by woman's age and weeks of gestation, United States, 2008
In the United States, approximately 85% of abortions in 2008 were performed by instrumental evacuation (vacuum aspiration, dilation and curettage or dilatation and evacuation).18 During the first trimester, vacuum aspiration with or without subsequent check curettage is the most frequently used method, but use of medication (mifepristone or methotrexate followed by misoprostol) is increasing and in 2008 accounted for 23% of abortions before 9 weeks.17 As in other developed countries, utilization of early medication abortion has continued to increase even 8 years after its approval by the FDA. Between 16 and 20 weeks, dilation and evacuation was used in 97% of abortions in 2008, and after 20 weeks in 91%.17 Prostaglandins are often used for cervical preparation with dilation and evacuation. Intrauterine saline instillation and uterine surgery (hysterectomy and hysterotomy) are rarely used.
In many European countries, second trimester abortions are commonly performed by labor induction, often employing mifepristone together with a prostaglandin or by prostaglandin alone. Where the volume of second-trimester abortions is low, it is impractical for physicians to develop the surgical skills needed for dilation and evacuation.
Experience has shown that both first- and second-trimester abortions can be performed safely in clinics and physicians' offices. In the United States, the proportion of abortions performed in hospitals has declined from more than half in 1973 to 4% in 2008.12 Only a small fraction of the hospital abortions were inpatient procedures, the remainder being performed on an outpatient basis or in a nonhospital facility. The number of hospitals where abortions are known to be performed has dropped from a peak of 1687 in 1976 to 610 in 2008, and among hospitals offering abortion services, the number of abortions per hospital has fallen.12 An important factor in the shift of abortion services to nonhospital settings is the greater cost of using hospital facilities to provide the service. Hospital abortions are generally more common in other developed countries, in part because they are not discouraged by the financing mechanisms and because of policies to make services locally available. In France, for example, one public hospital in each local district is required to offer the service.
In the United States, abortion services are increasingly concentrated in high-volume facilities. In 2008, 81% of abortions took place in the 387 clinics and nine hospitals that performed 1000 or more of the procedures during the year, and 70% took place in clinics where half or more of patient visits were for abortion services.12 Such facilities are generally located in large metropolitan areas, with the result that many women in small cities and rural areas must travel long distances for services. The concentration of abortions in high-volume clinics probably increases the experience and competence of the professionals involved and, thereby, the quality of the services. Conversely, follow-up care is fragmented, with possible unfavorable effects on the patient.
Although a majority of clinicians performing abortions are obstetrician/gynecologists, specialty training is unnecessary for this simple procedure. In 1997, 32% of clinicians in National Abortion Federation member clinics were family physicians, other physicians who were not obstetrician/gynecologists, or mid-level practitioners.22 Studies in the United States have shown that first-trimester vacuum aspiration abortions can safely be performed by mid-level practitioners such as physician assistants, nurse practitioners, and nurse midwives.23, 24, 25, Midlevel practitioners are providing aspiration and medication abortions in several states where it is permitted. Studies in several developing countries have also found equivalence in complication rates between physicians and mid-level practitioners.26, 27
COMPLICATIONS
Complication rates for abortion are difficult to define and to measure. For example, blood loss that would be considered unproblematic to one investigator might be considered hemorrhage by another. Complications recorded on state-mandated abortion-reporting forms may be underreported in part because infection and other problems may appear after the day the procedure was performed and the reporting form completed. Because fewer than one-third of abortion patients on average return for routine follow-up examination, delayed complications are not always known to the abortion facility.
A large case series of low-risk US abortion patients covered 170,000 consecutive first-trimester abortions performed by vacuum aspiration between 1971 and 1987. Follow-up information was obtained either at the clinic or by return of a physician's note on all but 8%. Only 121 patients had complications requiring hospitalization, a rate of 0.07%. Minor complications were reported for 0.85%; the most common of these were mild infection and need for resuctioning.28
A more recent study in 2013 comparing experienced physicians with newly trained mid-level practitioners found a rate of minor complications of 1.3% among 11,487 first-trimester aspiration patients and a rate of major complications of 0.05%.25
The largest database of abortion complications in the United States is maintained by the National Abortion Federation, an association of abortion providers. In 2005, members reported information on 223,800 abortions at all gestational ages; follow-up information was available for 29%. Complications requiring hospitalization were reported for 139 patients for a rate of 0.06% of all patients and 0.21% of those with follow-up, and transfusion was required for 0.01% (0.05% of those with follow-up). Assuming all complications were known to the providers, the complication rates of first-trimester surgical patients were as follows: retained tissue 0.32%; continuing pregnancy 0.12%; infection 0.06%; hemorrhage 0.01%; and unrecognized ectopic pregnancy and uterine injury, each 0.006%. Complication rates for early medication abortion were: retained tissue 1.0%; continuing pregnancy 0.6%; hemorrhage 0.06%; infection 0.06%; and unrecognized ectopic pregnancy 0.01%. The true rates are likely to be higher because not all complications may have been known to providers and reported.
There have been no other large-scale compilations of abortion complications in recent years in the United States, only smaller studies from individual providers. Complication rates are described further in the chapters on abortion procedures.
MORTALITY
Before abortion was legalized in developed countries, thousands of women died from unsafe illegal abortions, although it is difficult to estimate the numbers. Today this situation continues in countries where abortion is illegal. The World Health Organization estimates that 47,000 women die from unsafe abortion each year, almost all in developing countries where abortion is illegal.29 While this number has declined in recent years, the proportion of maternal mortality attributable to induced abortion, 13%, has remained unchanged. Mortality is estimated at 220 deaths per 100,000 unsafe abortions.30 The mortality rate is high because risky abortion methods are often used in areas where legal abortion services are prohibited, and because of the poor health care generally in many developing countries. The main causes of death are infection, hemorrhage, and organ damage.30
High levels of mortality from legal abortion prevailed in the United States as elsewhere during the period of restrictive legislation, when a significant proportion of the women undergoing abortion experienced pre-existing complications that made them poor risks for any type of surgery. In 1972, the mortality rate was 4 per 100,000 legal terminations. The rate fell to 2 in 1973–1977, when elective abortion became more easily available to most women (Table 4). As abortion services improved with increasing experience and technical advances, mortality fell to 0.8 in 1978–1982 and to 0.7 in 1983–1992. Since 1992, mortality has leveled off at about 0.6 per 100,000. Mortality from illegal abortion fell from 39 recorded deaths in 1972 to 2 in 1976. In recent years there has continued to be a death every few years from illegal abortions (i.e. abortions performed by someone other than a licensed physician or someone acting under the supervision of a licensed physician).
Table 4. Number of legal abortions, number of associated deaths, and mortality per 100,000 abortions (United States)
| Years or characteristics | Number of abortions
| Number of deaths
| Deaths per 100,000 abortions |
| Year |
| ||
| 1972 | 587,000 | 24 | 4.1 |
| 1973–1977 | 5,173,000 | 108 | 2.1 |
| 1978–1982 | 7,612,000 | 59 | 0.8 |
| 1983–1992 | 15,726,000 | 106 | 0.7 |
| 1993–2003 | 14,729,000 | 87 | 0.6 |
| 2004–2008 | 6,093,000 | 39 | 0.6 |
| Gestation, 1988–1997 (weeks)* |
| ||
| ≤8 | 7,700,000 | 11.1 | 0.1 |
| 9–10 | 3,671,000 | 6.9 | 0.2 |
| 11–12 | 1,775,000 | 8.3 | 0.5 |
| 13–15 | 953,000 | 20.7 | 2.2 |
| 16–20 | 591,000 | 26.3 | 4.4 |
| ≥21 | 159,000 | 20.7 | 13.0 |
| Age, 1988–1997 |
| ||
| <20 | 3,188,000 | 20 | 0.6 |
| 20–29 | 8,230,000 | 47 | 0.6 |
| 30 and older | 3,407,000 | 26 | 0.8 |
| Race, 1988–1997 |
| ||
| White | 9,150,000 | 38 | 0.4 |
| Black and other | 5,674,000 | 56 | 1.0 |
*Twenty-six deaths with unknown gestation were distributed proportionately
Note: Number of abortions as estimated by the Guttmacher Institute
Information on abortion mortality is provided by the CDC, which investigates all reports of abortion-related deaths, whether or not abortion is recorded as a cause of death on the death certificate.31 The CDC reports include all deaths associated with abortion, including those with another primary cause, usually a pre-existing medical condition. The main causes of death associated with legal abortion are infection, hemorrhage, embolism, and complications of anesthesia. Since the early 1970s, the number of deaths has dropped sharply from all causes.32 One of the main risk factors for abortion mortality is the period of gestation when pregnancies are terminated. In the United States between 1988 and 1997, mortality ranged from 0.1 per 100,000 abortions at 8 weeks or less to 13.0 per 100,000 for abortions at 21 weeks or more. Mortality increased by approximately 30–40% with each week of gestation past 8 weeks.33
Age has little relation to abortion mortality, but mortality is distinctly higher among women of minority races than among white women. Mortality was higher during 1974–1977 for first-trimester abortions performed in hospitals than for abortions in nonhospital facilities. The difference disappeared when women with pre-existing complications or concurrent sterilization were excluded from the hospital data.34 Similar results were found for abortions performed at 13–15 weeks by dilation and evacuation between 1972 and 1978.35 These analyses have not been repeated for more recent years.
Abortion-related mortality may be compared appropriately with the risk to life associated with carrying a pregnancy to term. In the United States, maternal mortality attributed to complications of pregnancy and childbirth, excluding induced abortion, was 8.7 deaths per 100,000 live births in 1993–2003, based on data recorded on death certificates. Excluding deaths from spontaneous abortion and ectopic pregnancy, some of which may have resulted from pregnancies that would have ended in induced abortion if they had been normal, mortality was 7.9 per 100,000 live births. These statistics exclude deaths associated with but not attributed to pregnancy and childbirth. Thus, mortality from induced abortion before around 20 weeks of gestation is lower than maternal mortality attributed to childbirth, and mortality from abortion is not statistically significantly higher at any gestation. Overall, the mortality risk associated with continuing a pregnancy (at least 7.9) is more than 10 times the risk associated with induced abortion (0.6).
The safety of abortion in the United States is comparable to that in other developed countries, even though most other countries have a smaller proportion of second-trimester abortions and count only the deaths attributed to abortion. As listed in Table 5, abortion mortality ranges from 0.1–1.0 death per 100,000 procedures. Because of the small numbers of deaths on which the rates are based, the differences among the countries are not statistically significant.
Table 5. Number of legal abortions, associated deaths, and mortality rate per 100,000 legal abortions by country
| Country | Abortions (1000s) | Deaths* | Mortality Rate† |
| Belarus (1991–1996) | 1127.5 | 9 | 0.8 (0.3–1.3) |
| Bulgaria (1984–1996) | 1451.0 | 2 | 0.1 (0.0–0.5) |
| Canada (1976–1994) | 1407.7 | 2 | 0.1 (0.0–0.5) |
| Czech Republic (1984–1996) | 1091.1 | 4 | 0.4 (0.0–0.7) |
| Denmark (1976–1995) | 425.1 | 2 | 0.5 (0.1–1.7) |
| England & Wales (1991–1993) | 520.3 | 5 | 1.0 (0.3–2.2) |
| Finland (1976–1995) | 271.0 | 2 | 0.7 (0.1–2.7) |
| Hungary (1984–1996) | 1080.7 | 2 | 0.2 (0.0–0.7) |
| The Netherlands (1976–1997) | 958.7 | 1 | 0.1 (0.0–0.6) |
| Sweden (1977–1995) | 640.6 | 2 | 0.3 (0.0–1.1) |
| United States (1988–1992 | 7851.7 | 54 | 0.7 (0.5–0.9) |
| United States (1993–2003) | 14,729.4 | 87 | 0.6 (0.5–0.7) |
*Deaths were attributed to legal abortion on death certificates, except for England and Wales, where deaths are recorded on the abortion notification form, and the United States, where deaths include all those associated with abortion after investigation by the Centers for Disease Control and Prevention
†95% confidence intervals in parentheses
In all countries for which we have data, there were sharp declines in the abortion mortality rates between the 1970s and the 1980s. Factors that appear to account for the declines include increasing skill of abortion practitioners as a result of having more years of experience; the nearly universal adoption of vacuum aspiration; improved treatment of complications; advances in abortion technology; and, in some countries, a reduction in the proportion of procedures performed during the second trimester. There may also have been improvements in the underlying health condition of patients.
ACKNOWLEDGMENTS
Portions of this chapter were reproduced from Tietze C: Induced Abortion: Epidemiological Aspects. In Sciarra JJ (ed): Gynecology and Obstetrics. Philadelphia, Harper & Row, 1982.
REFERENCES
Center for Reproductive Rights: The World’s Abortion Laws Map, 2013 Update (Fact Sheet). http://reproductiverights.org/sites/crr.civicactions.net/files/documents/AbortionMap_Factsheet_2013.pdf |
|
Center for Reproductive Rights: letter to the United Nations Committee against Torture, March 7, 2012 (http://reproductiverights.org/sites/crr.civicactions.net/files/documents/crr_ElSalvador_Shadow_Letter_CAT_8.15.12v1.pdf). |
|
Boland R, Katzive L: Developments in laws on induced abortion: 1998-2007. Int Fam Plann Perspect 34:110, 2008 |
|
International Planned Parenthood Federation, European Network: Abortion Legislation in Europe (updated May 2012). http://archive-org.com/page/1066391/2012-12-25/http://www.ippfen.org/NR/rdonlyres/ED17CA78-43A8-4A49-ABE7-64A836C0413E/0/Abortionlegislation_May2012corr.pdf |
|
Cook PJ, Parnell AM, Moore M, Pagnini D: The effects of short-term variation in abortion funding on pregnancy outcomes. Journal of Health Economics, 1999, 18(2):241–257. |
|
Henshaw SK, Joyce TJ, Dennis A, Finer LB, and Blanchard K: Restrictions on Medicaid Funding for Abortions: A Literature Review. New York: Guttmacher Institute, 2009. |
|
Field MG: The re-legalization of abortion in Soviet Russia. New England Journal of Medicine 255:421, 1956 |
|
Sedgh G, Singh S, Shah IH, Ahman E et al.: Induced abortion: incidence and trends worldwide from 1995 to 2008. The Lancet 379:625, 2012. |
|
Westoff CF: A new approach to estimating abortion rates. DHS Analytical Studies No. 13. Calverton, Maryland: Macro International Health, 2008. |
|
Henshaw SK, Morrow E: Induced abortion, a world review , 1990 supplement. New York: The Alan Guttmacher Institute, 1990. |
|
Sedgh G, Singh S, Henshaw SK, Bankole A: Legal abortion worldwide in 2008: levels and recent trends. International Perspectives on Sexual and Reproductive Health 37:84, 2011. |
|
Jones RK, Kooistra K: Abortion incidence and access to services in the United States, 2008. Perspectives in Sexual and Reproductive Health 43:41, 2011. |
|
ProQuest Statistical Abstract of the United States 2013: National Data Book. Bernan Press: Blue Ridge Summit, Pennsulvania, 2013. |
|
Finer LB, Zolna MR: Unintended pregnancy in the United States: incidence and disparities, 2006. Contraception 84:478, 2011. |
|
Santelli JS, Lindberg LD, Finer LB, Singh S: Explaining recent declines in adolescent pregnancy in the United States: The contribution of abstinence and improved contraceptive use. Am J Pub Health 97:150, 2007 |
|
Jones RK, Finer LB, Singh S: Characteristics of U.S. abortion patients, 2008. New York: Guttmacher Institute, May 2010. |
|
Pazol K, Zane SB, Parker WY, Hall LR, et al.: Abortion Surveillance—Untied States, 2008. MMWR Surveillance Summaries, Vol. 60, No. 15, Nov. 25, 2011. |
|
Jones RD, Darroch JE, Henshaw SK: Patterns in the socioeconomic characteristics of women obtaining abortions in 2000-2001. Perspectives on Sexual and Reproductive Health 34:226, 2002. |
|
Finer LB, Frohwirth LF, Dauphinee LA, Singh S: Reasons U.S. women have abortions: Quantitative and qualitative perspectives. Perspectives on Sexual and Reproductive Health 37:110, 2005. |
|
Jones RK, Frohwirth LF, Moore AM: "I would want to give my child, like, everything in the world": How issues of motherhood influence women who have abortions. Journal of Family Issues 29:79, 2008 |
|
Jones RK, Darroch JE, Henshaw SK: Contraceptive use among U.S. women having abortions in 2000-2001. Perspectives on Sexual and Reproductive Health 34:294, 2002 |
|
Lichtenberg SE, Paul M, Jones H: First trimester surgical abortion practices: a survey of National Abortion Federation members. Contraception 64:345, 2001 |
|
Goldman MB, Occhiuto JS, Peterson LE, Zapka JG, Palmer RH: Physician assistants as providers of surgically induced abortion services. American Journal of Public Health 94:1352, 2004 |
|
Freedman MA, Jillson DA, Coffin RR, Novick LF: Comparison of complication rates in first trimester abortions performed by physician assistants and physicians. American Journal of Public Health 76:550, 1986 |
|
Weitz tA, Taylor K, Desai S, Upadhyay UD et al.: Safety of aspiration abortion performed by nurse practitioners, certified nurse midwives, and physician assistants under a California legal waiver. American Journal of Public Health 103:454, 2013 |
|
Warriner IK, Meirik O, Hoffman M et al.: Rates of complications in first-trimester manual vacuum aspiration abortion done by doctors and mid-level providers in South Africa and Vietnam: a randomised controlled equivalence trial. Lancet 368 (9551):1965, |
|
Jeejeebhoy SJ, Kalyanwala S, Zavier AJ et al.:Can nurses perform manual vacuum aspiration (MVA) as safely and effectively as physicians? Evidence from India. Contraception 84:615, 2011 |
|
Hakim-Elahi E, Tovell HMM, Burnhill MS: Complications of first-trimester abortion: A report of 170,000 cases. Obstet Gynecol 76: 129, 1990 |
|
World Health Organization: Unsafe Abortion: Global and Regional Estimates of the Incidence of Unsafe Abortion and Associated Mortality in 2008. Geneva, Switzerland: WHO, 2011. |
|
Singh S: Hospital admissions resulting from unsafe abortion: estimates from 13 developing countries. Lancet 369(9550):1887, 2006 |
|
Pazol K, Creango AA, Zane SB, Burley KD, et al.: Abortion Surveillance—Untied States, 2009. MMWR Surveillance Summaries, Vol. 61, No. 8, Nov. 23, 2012 |
|
Lawson HW, Frye A, Atrash HK et al: Abortion mortality, United States, 1972 through 1987. Am J Obstet Gynecol 171: 1365, 1994 |
|
Bartlett LA, Berg CJ , Shulman HB et al: Risk factors for legal induced abortion-relation mortality in the United States. Obstetrics & Gynecology 103:729, 2004 |
|
Grimes DA, Cates W, Selik RM: Abortion facilities and the risk of death. Fam Plann Perspect 13: 30, 1981 |
|
Cates W, Grimes DA: Deaths from second trimester abortion by dilatation and evacuation: Causes, prevention, facilities. Obstet Gynecol 58: 401, 1981 |