Open Laparoscopy
Authors
INTRODUCTION
Open laparoscopy is a technique which allows placement of a laparoscopic camera port, in a controlled manner, by sharply opening the layers of the abdominal wall. Different techniques in open laparoscopy, regarding port stability and maintenance of the pneumoperitoneum, have subsequently been developed, as the incision in the fascia of the rectus abdomens is larger than the size of the port itself. Open laparoscopic entry is preferred in patients with a history of previous surgeries and patients in whom intra-abdominal adhesions are anticipated, as well as cases where other entry methods have failed.1 Consequently, some surgeons choose to use open laparoscopy in all instances, thereby allowing surgeons familiarize themselves with every step of this particular technique.
History of Procedure
Open laparoscopy was first developed by Dr. Harrith Hasson of Chicago, IL, who published the description of this technique in the American Journal of Obstetrics and Gynecology in 1971.2 In the past 38 years, this technique of open laparoscopy has become widely accepted and is constantly being modified to improve its practice. A survey published in 1998 revealed that approximately 30% of surgeons use Hasson open entry technique to perform laparoscopy,3 40% perform closed laparoscopy with Veress needle insufflation, and the remaining 30% utilize direct trocar insertion without prior insufflation. Dr. Hasson, in 2000, published 29 years of his personal experiences in the use and development of open laparoscopy.4 During that time he performed 5,284 procedures and found this entry technique to be safe, effective, and reproducible. There were only 27 complications in this group of patients, the majority being wound infections and hematomas. There was only one case of bowel perforation as a consequence of port entry.
TYPES OF OPEN LAPAROSCOPY PORTS
Open laparoscopy ports differ from standard closed ports in a singular but distinct manner. Most obvious is their lack of bladed or sharp trocars. Open laparoscopy port trocars are blunt and consist of a system which permits the tagged, abdominal fascia to be attached to the port, thereby stabilizing the port to the patient. A well-known example of this system is the Hasson open laparoscopy port. Depending on the type of port, a balloon may also be used to stabilize the port as well as maintain pneumoperitoneum.
TECHNICAL ASPECTS
There are different techniques for performing open laparoscopy. The common factor – entry into the peritoneal cavity – is achieved through sharp dissection of the layers of the abdominal wall under direct visualization. The technique presented here is one of the most common and simple means of achieving open laparoscopic entry.
- Using an Allis clamp, the surgeon should grasp the contralateral umbilical fold, and tent the umbilicus anteriorly. Allow your assistant to repeat this process.
- Using a 15-blade scalpel, make a full-thickness vertical skin incision in the center of the umbilicus, extending from superior to inferior umbilical fold.
- Using a Kocher clamp, the surgeon should grasp the fascia on the contralateral side through this umbilical incision. Allow your assistant to repeat this process.
- Elevate previously placed Kocher clamps and, using the same 15-blade scalpel, make a vertical full thickness incision through the fascia. This incision will usually penetrate both the fascia and the peritoneal, thereby entering the intra-peritoneal cavity. If the intra-peritoneal cavity is not entered, identify the peritoneum, grasp with smooth forceps or any blunt grasper, tent anteriorly and enter sharply.
- Use Metzenbaum scissors, or any other thin blunt-tipped instrument, to confirm entrance into the intra-peritoneal cavity.
- In cases where the port must be stabilized to the fascia, this step is the best time to tag the fascia with suture.
- Remove all instruments.
- Place the trocar within the incision and insufflate the intra-peritoneal cavity.
- Confirm intra-peritoneal placement with the laparoscopic cameraPlace any additional ports in your usual manner.
ADVANTAGES, DISADVANTAGES AND SCIENTIFIC EVIDENCE
Safety
Several studies suggest that initial trocar insertion is the most dangerous aspect of trocar use, and possibly the most dangerous step in minimally invasive surgery.5, 6, 7, 8 Champault et al. have shown that 83% of vascular injuries, 75% of bowel injuries, and 50% of local hemorrhage injuries were caused during primary trocar insertion.9 The incidence of these types of injuries may be higher in patients with previous abdominal surgeries and suspected adhesions. Both Brill and Nezhat10, 11 reported series of bowel and omental adhesions in 360 patients who had undergone previous abdominal surgery. Severe adhesions were noted in patients with a history of severe peritonitis, bowel resection, intra-abdominal cancer surgery, radio and chemotherapy and previously diagnosed adhesions. Not surprisingly, midline incisions had a higher incidence of adhesions than Pfannenstiel incisions; and patients with a history of previous gynecologic surgery had a higher risk of adhesions than patients with only an obstetrically related surgical history.
To increase the safety of port placement, a trocar was introduced in 1984 with a retractable shield that covers the tip before and after insertion. It is not clear today if this retractable shield decreases the risk of visceral or vascular injury. In a 1996 study by Champault, 103,852 procedures using a total of 386,784 trocars revealed that ten out of the 26 (39%) serious injuries and two out of the seven (29%) deaths involved these shielded trocars.9 That same year, the FDA decided (based upon the data to support the safety claims of those trocars) to refrain from using the term “safety trocar”, so as to not to give surgeons a false sense of security, and permitted use of the term “shielded trocars”.12
The greatest advantage of open laparoscopy is that the technique allows for precise, controlled entry into the intra-abdominal cavity. However, the data on added safety of open laparoscopy, in comparison to traditional closed laparoscopy are still inconclusive (Table 1). In 1997 Bonjer et al. published a retrospective review of literature comparing risks of visceral and vascular injury between open and closed laparoscopic technique.13 Data from 489,335 patients who underwent closed laparoscopy and 12,444 patients who had open procedure were collected. Rates of visceral and vascular injury were respectively 0.083% and 0.075% in the closed laparoscopy group, and 0.048% and 0% in the open laparoscopy group. Mortality rates evaluated, after closed and open laparoscopy, were 0.003% and 0%, respectively. Pearson χ2 analysis demonstrated a statistically significant difference in visceral and vascular injury between closed and open laparoscopy (p = 0.002), but there was no such difference for the mortality rates. A 2005 meta-analysis from Australia also compared risks of visceral and vascular injury in 760,890 patients who underwent closed entry procedure and 22,465 patients who had open laparoscopy.14 Patients in the closed group had 515 visceral injuries (0.07%) and 336 major vascular injuries (0.044%). This accounts for one vascular injury in 2272 patients. In the closed laparoscopy group there were no such vascular injuries (p = 0.003) and there were only 11 visceral injuries (0.05%, p = 0.18). Pasic15 performed a retrospective analysis of 3086 patients, over a 13-year period, who underwent laparoscopic surgery at University of Louisville Hospital in Kentucky. Five different techniques were used to achieve pneumoperitoneum: closed laparoscopy with Veress needle, open laparoscopy, direct entry, subcostal insufflation, and transfundal insufflation. In total, five major injuries were reported: three bowel injuries and two vascular injuries. All injuries occurred when utilizing closed laparoscopic technique; in spite of this, none were caused by Veress needle. Chapron et al.16 compared 8,324 patients in a closed laparoscopy group with 1,562 patients in an open laparoscopy group. They found the risk of converting to laparotomy was significantly higher in the group who underwent open laparoscopy – three cases (0.19%) versus 0 cases in closed laparoscopy (p = 0.04). The risk of major complications was comparable for both groups. In closed laparoscopy group there were four cases (0.05%) and in open laparoscopy there were three cases (0.19%, p = 0.08). The closed laparoscopy group had one vascular injury (aorta) and three bowel injuries; open laparoscopy had two bowel injuries and one postoperative bowel obstruction. Several other studies questioned the level of safety provided by open laparoscopy.11, 17, 18 Corson concluded that open laparoscopy offers little protection from bowel injury but decreases the risk of vascular injury.17 Most recent data, published in the Cochrane Database, reviewed laparoscopic entry techniques and showed no safety advantage of open laparoscopy versus Veress needle closed technique.1 Meta-analysis demonstrated no evidence of an advantage for using either open entry or closed entry with Veress needle in terms of vascular injury and visceral injury with an odds ratio of 0.14 (95% CI 0.00–6.82) and 1.00 (95% CI 0.06–16.14), respectively. Because of mixed results on safety of open laparoscopy, a large group of internationally known gynecologists and surgeons prepared a consensus document stating that currently there is no evidence that this technique is safer or more dangerous than any other alternative methods of laparoscopic entry.19
Table 1 Relative risk of visceral and vascular injury with open and closed laparoscopy
| Closed visceral (%) | Open visceral (%) | P+ | Closed vascular (%) | Open vascular (%) | χ2 | |
| Bonjer, 1997 | 0.083 | 0.048 | 0.002 | 0.075 | 0 | 0.002 |
| Chapron, 2003 | 0.036 | 0.13 | 0.08 | 0.01 | 0 | |
| Laborina, 2005 | 0.07 | 0.05 | 0.18 | 0.044 | 0 | 0.003 |
Speed
The second potential benefit of open laparoscopy is time to the achievement of pneumoperitoneum. There are several studies which have shown a small decrease in this amount of time, when compared to closed laparoscopy techniques. Conversely, there are several other studies which show there is no benefit in time.20, 21 Perone in 585 found that the average time to achieve pneumoperitoneum was 2.5 minutes and to close open laparoscopy incision 4 minutes.22 Gordon demonstrated in 237 patients that average time to achieve pneumoperitoneum was 3.5 minutes.23
Convenience
One of the big advantages of open laparoscopy is that it allows for easy retrieval of specimens from the abdominal cavity. Hasson port may be removed at any time during the procedure. Using a camera through an assistant port, specimens may be removed through the incision in the umbilicus. If necessary, fascial incision in the umbilicus can be extended. Prior to reinsertion of Hasson port, fascia has to be sutured to the size of an occluder on the port and surgery can continue. In closed laparoscopy, once the port is removed and incision in the fascia extended, port may not be reinserted because of the gas leak.
Gas leak
Two of the drawbacks of open laparoscopy are potential for leakage of CO2 gas and difficulty in achieving pneumoperitoneum. Various modifications of Hasson trocars have been designed to provide an ideal seal for escaping gas. Nevertheless the rate of gas leakage in literature ranges from 4.2 to 14.2%.21, 23 In case of leakage of carbon dioxide around the Hasson trocar most practitioners use towel clamps around the incision and Vaseline gauze or simply a suture to achieve pneumoperitoneum.
TIPS AND TRICKS FROM A TEACHING ATTENDING
- If the patient has a deep umbilicus grasp the bottom with hemostat and pull it out. Then make a vertical incision through the skin of the umbilicus and place Allis clamps on the cut edges. Proceed in the usual way with Kocher clamps and incision of the fascia.
- When closing skin of the deep umbilicus place two separate sutures in the center of the incision. Use one of them to suture cephalad and other to suture caudad
- If you cannot find the fascia after the initial skin incision, make it slightly bigger and use S-retractors, Army-Navy retractors or small Richardson retractors to identify the fascia.
- If you cannot place stay sutures in the fascia after abdomen is entered, place them in the skin. Do not place sutures in the fat between the skin and fascia, because sutures will pull out.
- If after entering the abdomen there is evidence of bowel injury, make the incision slightly bigger. Small bowel can be pulled out through that incision, repaired and placed back in the abdomen. After fascial incision is sutured smaller to the size of the occluder, Hasson port can be reintroduced and surgery can continue.
- If, after placing the Hasson port you notice omental adhesions close by, you can remove the port, place one finger through the incision and sweep the adhesions off. Be very careful if there is any bowel in those adhesions, because bowel wall can be easily torn with blunt dissection.
- When using the robot make sure that at least 4 cm of the shaft of laparoscopic protrudes above the skin. This is necessary to dock the camera arm of DaVinci robot. If patient is overweight you may have to use a longer port.
ILLUSTRATIONS
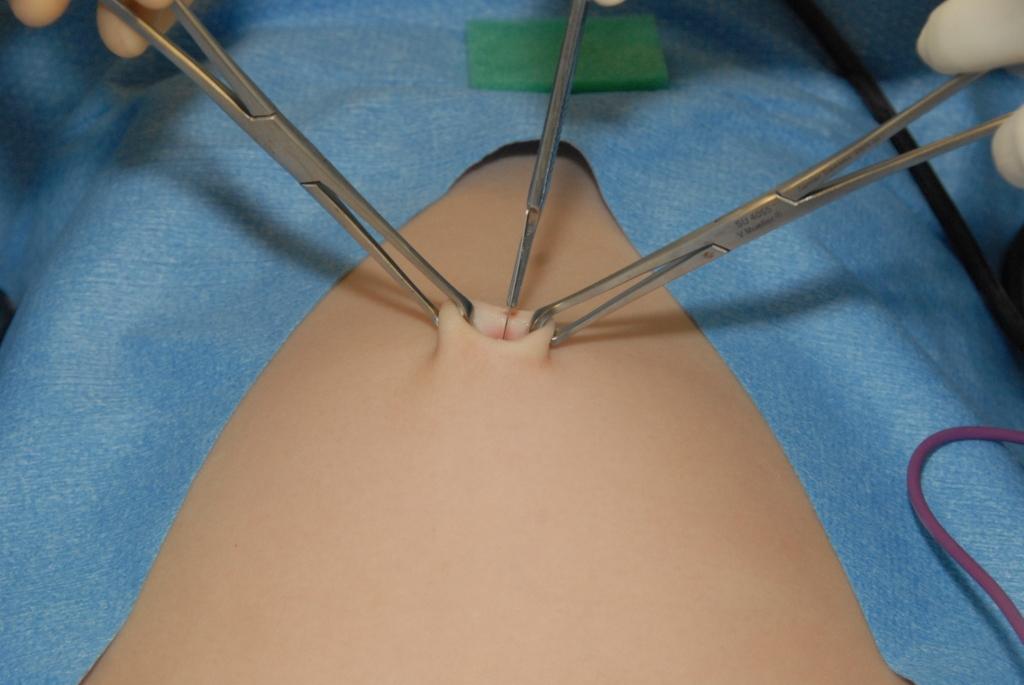 Fig. 1. Incision through the skin of the umbilicus. Allis clamps applied on both sides of the umbilicus
Fig. 1. Incision through the skin of the umbilicus. Allis clamps applied on both sides of the umbilicus
 Fig. 2. Incision through the fascia and peritoneum. Kocher clamps applied on the fascia
Fig. 2. Incision through the fascia and peritoneum. Kocher clamps applied on the fascia
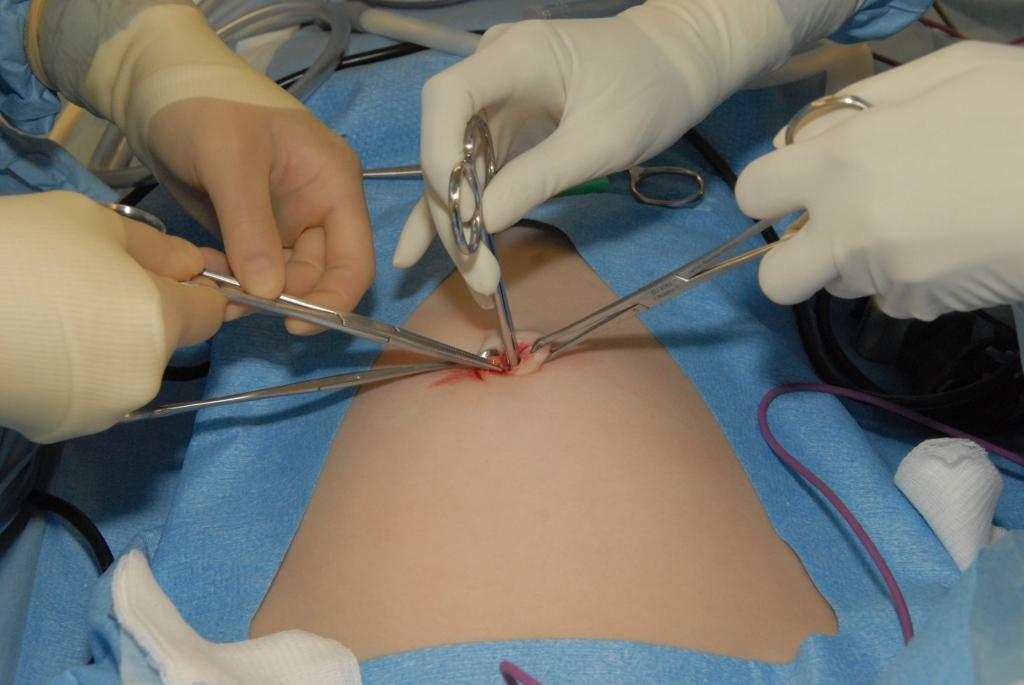 Fig. 3. Metzembaum scissors in the abdominal cavity to confirm successful entry
Fig. 3. Metzembaum scissors in the abdominal cavity to confirm successful entry
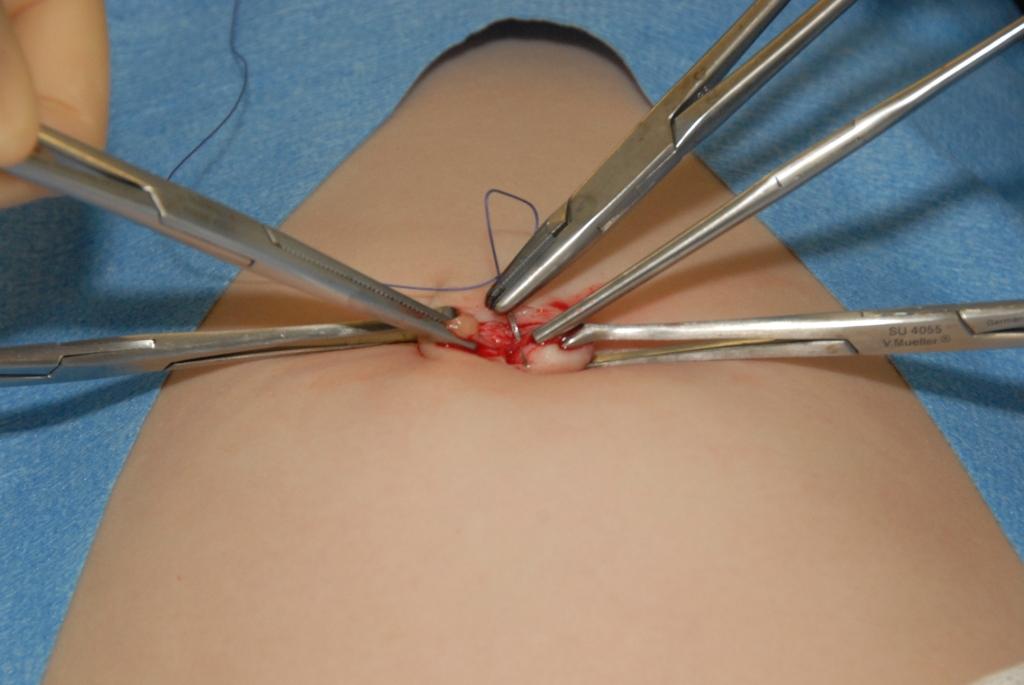 Fig. 4. Suture (2-0 Vicryl on UR6 needle) placed in the fascia
Fig. 4. Suture (2-0 Vicryl on UR6 needle) placed in the fascia
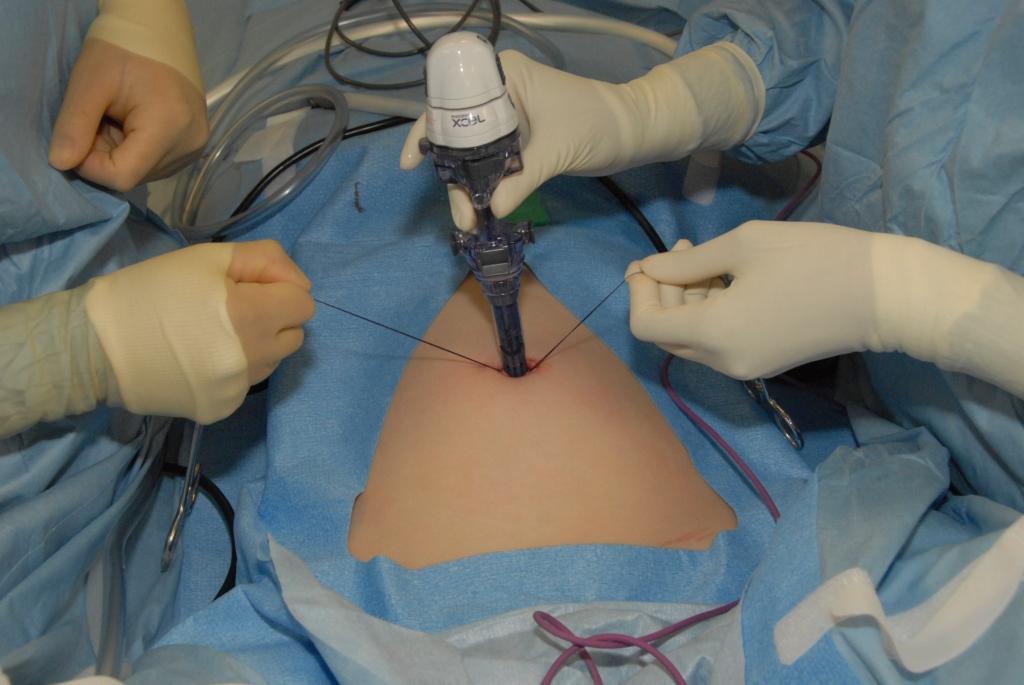 Fig. 5. Hasson port (Ethicon Xcel) placed in the abdomen
Fig. 5. Hasson port (Ethicon Xcel) placed in the abdomen
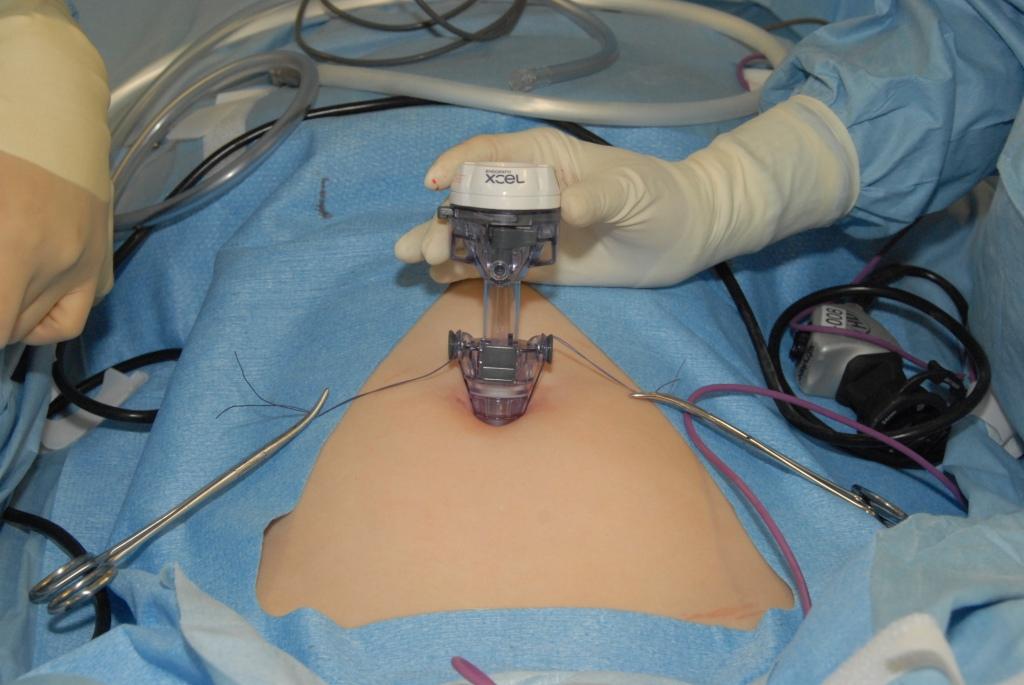 Fig. 6. Port secured with the suture
Fig. 6. Port secured with the suture
REFERENCES
Ahmad G, Duffy JM, Phillips K, Watson A. Laparoscopic entry techniques. Cochrane Database Syst Rev. 2008(2):CD006583. |
|
Hasson HM. A modified instrument and method for laparoscopy. Am J Obstet Gynecol 1971;110(6):886-887. |
|
Trocars: safety and selection. Emergency Care Research Institute. Health Devices. 1998;27(11):376-399. |
|
Hasson HM, Rotman C, Rana N, Kumari NA. Open laparoscopy: 29-year experience. Obstet Gynecol 2000;96(5 Pt 1):763-766. |
|
Mac Cordick C, Lecuru F, Rizk E, et al. Morbidity in laparoscopic gynecological surgery: results of a prospective single-center study. Surg Endosc 1999;13(1):57-61. |
|
Yuzpe AA. Pneumoperitoneum needle and trocar injuries in laparoscopy. A survey on possible contributing factors and prevention. J Reprod Med 1990;35(5):485-490. |
|
Corson SL, Chandler JG, Way LW. Survey of laparoscopic entry injuries provoking litigation. J Am Assoc Gynecol Laparosc 2001;8(3):341-347. |
|
Chapron CM, Pierre F, Lacroix S, Querleu D, Lansac J, Dubuisson JB. Major vascular injuries during gynecologic laparoscopy. J Am Coll Surg 1997;185(5):461-465. |
|
Champault G, Cazacu F, Taffinder N. Serious trocar accidents in laparoscopic surgery: a French survey of 103,852 operations. Surg Laparosc Endosc 1996;6(5):367-370. |
|
Nezhat C. Operative Gynecologic Laparoscopy: Principles and Techniques. New York: McGraw-Hill, 1995:79-96. |
|
Brill AI, Nezhat F, Nezhat CH, Nezhat C. The incidence of adhesions after prior laparotomy: a laparoscopic appraisal. Obstet Gynecol 1995;85(2):269-272. |
|
Yin L, Witten C, Neidelman S. Letter to manufacturers of laparoscopic trocars. In: FDA, Center for Devices and Radiological Health, Rockville, MD, Aug 23, 1996. |
|
Bonjer HJ, Hazebroek EJ, Kazemier G, et al. Open versus closed establishment of pneumoperitoneum in laparoscopic surgery. Br J Surg 1997;84(5):599-602. |
|
Larobina M, Nottle P. Complete evidence regarding major vascular injuries during laparoscopic access. Surg Laparosc Endosc Percutan Tech 2005;15(3):119-123. |
|
Pasic RP, Kantardzic M, Templeman C, Levine RL. Insufflation techniques in gynecologic laparoscopy. Surg Laparosc Endosc Percutan Tech 2006;16(1):18-23; discussion 23-14. |
|
Chapron C, Cravello L, Chopin N, et al. Complications during set-up procedures for laparoscopy in gynecology: open laparoscopy does not reduce the risk of major complications. Acta Obstet Gynecol Scand 2003;82(12):1125-1129. |
|
Hanney RM, Carmalt HL, Merrett N, Tait N. Vascular injuries during laparoscopy associated with the Hasson technique. J Am Coll Surg 1999;188(3):337-338. |
|
Wherry DC, Marohn MR, Malanoski MP, et al. An external audit of laparoscopic cholecystectomy in the steady state performed in medical treatment facilities of the Department of Defense. Ann Surg 1996;224(2):145-154. |
|
A consensus document concerning laparoscopic entry techniques: Middlesbrough, March 19 - 20 1999. Gynaecol Endosc 1999;8(6):403-406. |
|
Ballem RV, Rudomanski J. Techniques of pneumoperitoneum. Surg Laparosc Endosc 1993;3(1):42-43. |
|
Hurd WW, Randolph JF, Jr., Holmberg RA, et al. Open laparoscopy without special instruments or sutures. Comparison with a closed technique. J Reprod Med 1994;39(5):393-397. |
|
Perone N. Laparoscopy using a simplified open technique. A review of 585 cases. J Reprod Med 1992;37(11):921-924. |
|
Gordon S, Maher P, Seman E. Open laparoscopy utilizing either a 5 mm or 10 mm standard intra-umbilical trocar. Gynaecol Endosc 2001;10(4):249-252. |