Operative Hysteroscopy
Authors
INTRODUCTION
Modern hysteroscopy was introduced in the early 1970s, as instruments were improved and modified to provide easier manipulation within the uterine cavity.1 The main objective was to achieve tubal sterilization via the hysteroscope. Sterilization, particularly by electrocoagulation, proved unsatisfactory and risky, however; and attention turned to other therapeutic applications of hysteroscopy.2 During the 1980s, the use of the hysteroscope as a therapeutic tool grew rapidly; today, most uterine conditions that once required a laparotomy and a hysterotomy can be treated via hysteroscopy.3,4
INSTRUMENTATION
The Hysteroscope
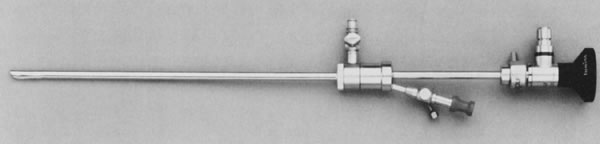
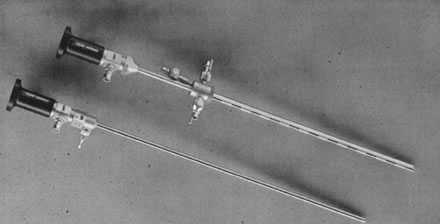
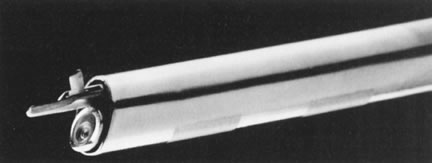
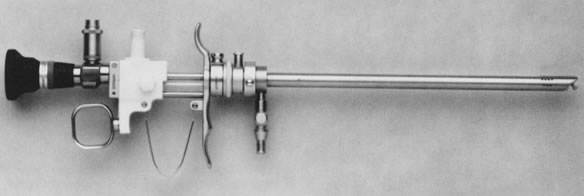
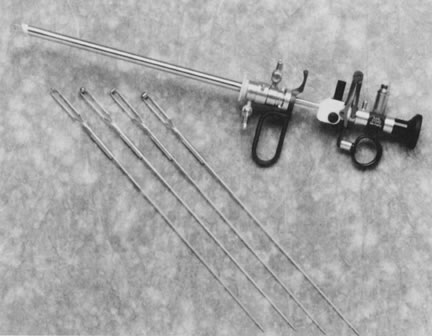
There are two types of hysteroscopes: rigid and flexible. The rigid type is more commonly used. The rigid hysteroscope consists of a telescope with a 4-mm outer diameter and a Foroblique vision of 30°. The outer sheath varies in outer diameter from 7 to 8 mm, and contains ports for instillation of the distending medium and its optional retrieval via catheters; also, there is an operative channel for French size 7 instrumentation. Because the hysteroscope cannot always be introduced atraumatically after cervical dilatation, an obturator fitting the outer sheath is also provided to simulate a smooth, blunt dilator. Most rigid telescopes contain a rod lens system, as designed by Professor Hopkins, which provides a larger angle of view and brighter image than the original “bead” lens. The most versatile direction of view for hysteroscopy is the Foroblique 30° angle; the 180°, 0°, 15°, and 25° angles may be more beneficial for the resectoscope. The depth of visual field of these telescopes is about 2 to 3 cm, with slight magnification (4x to 5x) using a liquid distending medium.
Most rigid operative hysteroscopes require assembly. The outer sheath must be attached to a bridge that includes the operating channel, but compact sheaths providing inflow and outflow channels as well as operating channels in a single unit are available (Weck).
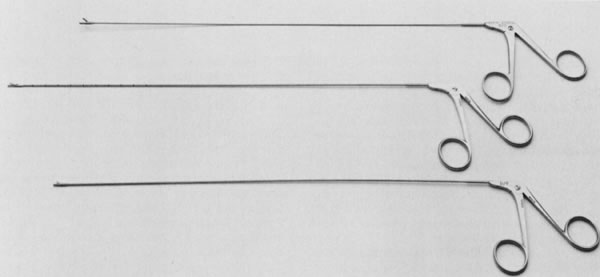
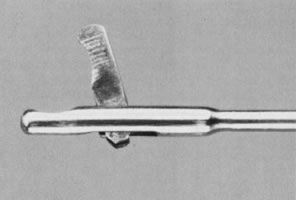
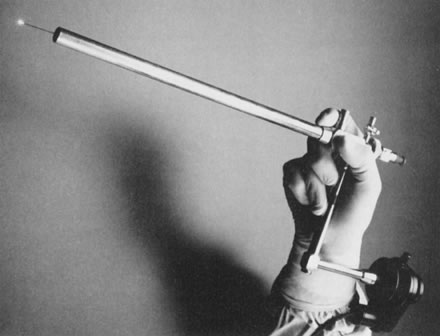
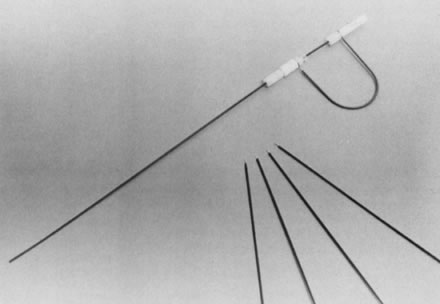
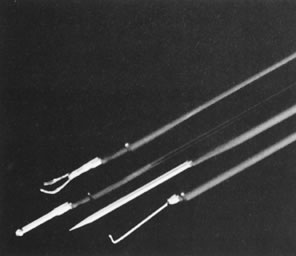
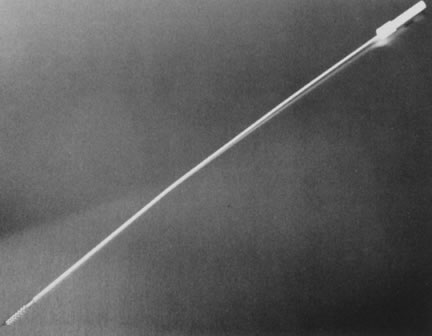
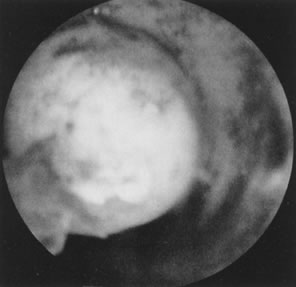
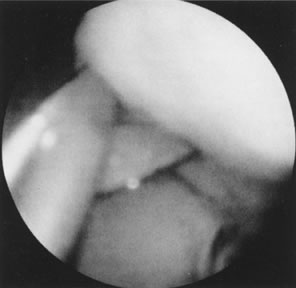
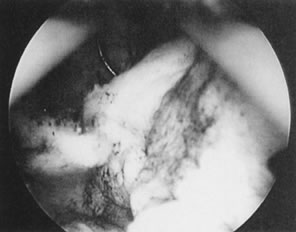
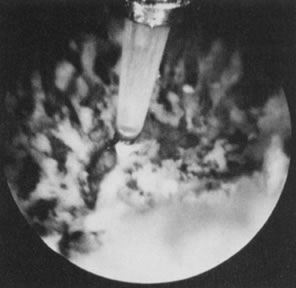
Ancillary instruments for use through rigid hysteroscopes are of three types: flexible, semi-rigid, and rigid. The flexible ancillary instruments (biopsy forceps, grasping forceps, scissors) were used originally; they were fragile, cumbersome, and needed frequent replacement. Semi-rigid instruments have replaced flexible instrumentation because they provide easier manipulation and more durability. They are easier to introduce through the operating channel and can be manipulated more precisely and quickly than the flexible instruments; they bend slightly, but cannot be bent to 90° without breaking. They are the instruments of choice when mechanical instrumentation is required for hysteroscopy. The rigid or so-called optical instruments fixed at the end of the operating bridge are sturdier and can also be used through the hysteroscope. They require a perfect panoramic view and must be manipulated with caution. They are cumbersome to use, because the whole instrument must be moved toward the target, and the panoramic view may be impaired when approaching target tissues. The rigid operative instrument must be carefully introduced into the uterus to avoid perforation (Figs. 1, 2, 3, 4, 5, and 6).
|
|
|
|
|
|
Flexible and steerable hysteroscopes are available with an outer diameter of 4.9 mm and an operating channel of 2 mm. These instruments permit introduction of flexible instrumentation and offer steerability and flexion inside the uterus for better viewing of the uterotubal openings and the lateral aspects of the uterine wall. These instruments are flexible but lack the capabilities of the semi-rigid instruments; they are small and fragile and may not withstand or permit extensive intrauterine manipulations. They permit tubal cannulation because their steerability simplifies the technique. They can direct fiber lasers laterally, providing better access to the lateral walls of the uterus, which can be difficult with rigid instrumentation. The flexible operating instruments seem better suited for operating at the uterotubal cones than do the rigid instruments.
An inherent drawback to the flexible hysteroscopes is diminution in the image due to light transmission by fibers, rather than by rod lenses, which causes a slightly grainy image. Also, the high cost of this sophisticated instrumentation should be considered.
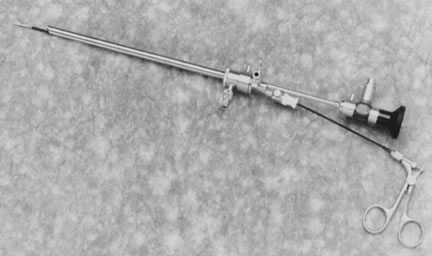
The Resectoscope
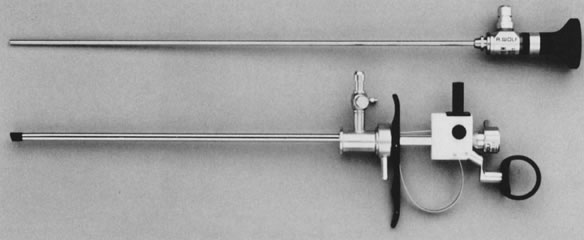
The urologic resectoscope has been adapted to gynecology by changing its shape and size and adding continuous-flow systems.
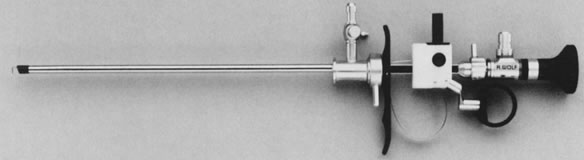
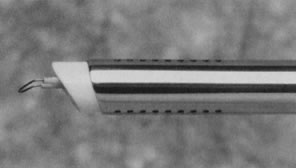
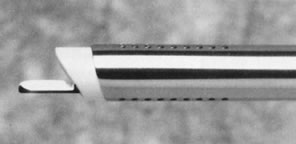
The resectoscope includes a straightforward telescope (0°), or one slightly deviated in a Foroblique fashion (15–25°), with a 3.5–4 mm outer diameter and an outer sheath 8–9 mm in diameter. Two concentric sheaths provide the mechanism for a continuous-flow system. The inner sheath provides the inflow, and the outer sheath (with several distal fenestrations and a small ceramic tip to prevent thermal conduction) provides the outer flow. There are smaller outer-diameter (6- and 5-mm OD) sheaths, but the ideal seems to be 8 mm OD or 24 French size. The thick cervical canal is sometimes difficult to dilate to more than 8 mm. An important component of the resectoscope is the bridge, which includes built-in mechanisms with a spring-loaded system to manipulate the electrode from front to back; this also encases the telescope. By activating the spring mechanism, the electrodes can be moved about 4 cm into the visual field of the objective lens, providing a clear, unobstructed view of the uterine cavity.
Although the usual approach with the hysteroscope is to place the fiberoptic cord connection down, providing slight upward vision of the uterine cavity, the initial orientation with the resectoscope is the opposite. The cord must face up, so that the Foroblique vision is directed downward to allow observation of the electrode. The electrical activation of the resectoscope with the connected electrode is obtained by connection of an electrical cord to a high-frequency electrosurgical unit (Figs. 7, 8, 9, 10, 11, 12, and 13).
|
|
|
|

|
|
|
Ancillary Instrumentation
To obtain the best visualization, a good light source is needed. The xenon lamp is excellent for performing operative procedures with the hysteroscope and/or the resectoscope. Other light sources may not provide such good visualization.
Electrosurgical units with wattage display and an attached return electrode monitor are necessary when operating with a resectoscope; appropriate grounding of the patient is necessary.
Operative hysteroscopy without video systems is cumbersome and tiring for the endoscopist because the operator not using video systems must be in continuous ocular contact with the proximal end of the endoscope. The assistant and other personnel cannot participate in the operation. With the resectoscope, use of the monitor is even more important, particularly because magnification and visualization provided by the new cameras increase the field of view and allow detailed observation of the lesions to be treated, and the operation is performed with more comfort and speed (Fig. 14).
|
Energy Sources
Fiberoptic lasers and electrosurgery can be used with the hysteroscope. Fiberoptic lasers are best suited for hysteroscopic surgery, not only because these lasers can be transmitted through the fiber inserted into the operating channel, but also because these lasers are not blocked by fluids and can be easily directed to any area of the uterine cavity. The neodymium:yttrium- aluminum-garnet (Nd:YAG) laser is most commonly used, particularly for endometrial ablation, because it is attracted by the purplish tissue and because it destroys tissue protein by coagulation with its frontal, back, and lateral scattering. The depth of penetration of 4–5 mm makes it suitable for endometrial ablation. This laser is in the infrared portion of the spectrum, with a 1064-nm wavelength, and is specifically absorbed by tissue protein.
Although the “bare” fiber is most useful for endometrial ablation, the new sculptured or extruded fibers can also be used to cut tissues such as adhesions, or for division of a uterine septum, because of their decreased scattering and their concentration and focusing of the beam to produce cutting and minimal coagulation. Sapphire tips can be attached to the quartz fiber of the Nd:YAG, but these fibers should not be used in the uterine cavity. The need for cooling with coaxial channels increases the amount of fluid injected into the uterine cavity and may cause serious accidents if gaseous coolants are chosen, because these gases must be introduced at the rate of about 1 L/min (Fig. 15).
|
Electrosurgery also can be performed through the hysteroscope, particularly to obtain precise coagulation or cutting with specially shaped electrodes. Use of these electrodes, designed to be passed through the hysteroscope, is not often needed, however, and the resectoscope with appropriately shaped electrodes is most suitable for most of these procedures (Figs. 16, 17, and 18).
|
|
|
DISTENDING MEDIA FOR OPERATIVE HYSTEROSCOPY
Fluids of low or high viscosity are the most commonly used distending media for operative hysteroscopy.
Low-Viscosity Fluids
Low-viscosity fluids are of two types: fluids containing electrolytes and fluids devoid of electrolytes. The most important feature in operative hysteroscopy is an appropriate distention of the uterine cavity for an unobstructed panoramic view. This is obtained with an adequate distending medium providing continuous distention and washing of the uterine cavity. Unfortunately, most hysteroscopes do not have a continuous-flow system; therefore, they require adjuncts such as polyethylene catheters to retrieve fluid, debris, mucus, or blood when an operative procedure is performed. The continuous retrieval of the injected fluid does not offer a good measure of inflow and outflow, and chances of excessive fluid intravasation increase.
LOW-VISCOSITY FLUIDS WITH ELECTROLYTES.
In general, when performing operative hysteroscopy with mechanical tools or with the laser, it is important to use a distending medium containing electrolytes, particularly sodium. Sodium is the main cation needed to maintain a balanced homeostasis, should intravasation occur. Sodium will permit urinary output and decrease the threshold for possible fluid overload; although fluid overload could occur, the threshold would be higher than when fluids without electrolytes are used.
The low-viscosity fluids with electrolytes used for operative hysteroscopy are: normal saline, dextrose 5% in half normal saline (0.45 NaCl), and Ringer's lactate, a balanced solution that permits adequate visualization. All provide similar visualization and should be used when no electrosurgical energies are required.
LOW-VISCOSITY FLUIDS WITHOUT ELECTROLYTES.
When electrosurgery is required and, specifically, when the resectoscope is used, only fluids devoid of electrolytes should be used. Electrolytes are conductive and may erratically disperse the electricity, with possible injury to other organs. The most commonly used fluids for electrosurgery in the uterine cavity are dextrose 5% in water, glycine 1.5%, sorbitol 3%, and Cytal (sorbitol 3%, + 0.5% of mannitol) or mannitol 5%. These media do not contain electrolytes and can be used safely when activating the resectoscope. Dextrose 5% in water with an osmolarity of 256 mOsm can be used safely when activating the resectoscope. Because it is usually packaged in plastic or glass 1-L bottles, a pump is required for its delivery to provide adequate distention of the uterine cavity; unless it is a mechanical pump, it is cumbersome to improvise by compressing the plastic bag, because the fluid can easily be eliminated and requires many impractical replacements.
Glycine 1.5% is an amino acid that degrades in ammonia, serine, and glyoxylic acid. If excessive quantities of this substance are intravasated, central nervous system toxicity may occur as a result of hyperammonemia. When using this substance, one should take special care to measure inflow and outflow; fluid not accounted for has probably been intravasated. In general, no more than 700 mL of unaccounted fluid should be allowed. When this occurs, the patient's vital signs, pulse oximetry, urine output, and, specifically, serum sodium should be evaluated. Any changes in these parameters should cause the physician to stop the procedure.
Glycine packaged in 3-L plastic bags is employed to distend the uterine cavity by using gravity and a high flow or urologic tubing. If the 3-L plastic bag is elevated 3 or 4 feet above the level of the patient, the pressure obtained will be sufficient to distend the uterus without the need of a pump. Inflow, outflow, and fluid deficit are measured as the procedure is performed.
Sorbitol 5% is a reduced sugar and also is packaged in 3-L plastic bags. It has an osmolality of 165 mOsm/L and provides good visualization similar to that provided by glycine. Urologists also have used Cytal, a component of sorbitol and mannitol, because mannitol may provide slight diuresis in these patients. Cytal must be used cautiously because diuresis may be accompanied by natriuresis, and if hyponatremia is present, this diuretic–natriuretic effect may worsen the situation.
High-Viscosity Fluids (Hyskon)
Hyskon, a derivative of dextran, is a 32% dextran solution with a molecular weight of 70,000 (mixed in 10% dextrose-in-water solution) that provides excellent visualization because of its crystal-clear solution. Its viscosity permits its use in small amounts for operations; it does not mix with blood, making it ideal for operative procedures. Because intravasation may occur during operative hysteroscopy, the amount used should be limited. Problems with this medium are related to the hyperosmotic properties of the substance, because it may absorb fluids, producing noncardiogenic pulmonary edema. Intravasation of excessive amounts of Hyskon may also cause coagulopathies. Intravasation of this high-viscosity fluid is perhaps due to the pressure required to instill it and the difficulty in retrieving the fluid that is injected into the uterine cavity. When using Hyskon, therefore, it is important to measure the amount injected and to calculate the amount retrieved, so as not to allow more than 400–500 mL of Hyskon to be lost in the system.
When using low-viscosity fluids, it is important to be aware of the volume of fluid that is not recovered from the patient. Fluids with electrolytes may permit more fluid to be absorbed by the patient without serious sequelae, but despite their electrolyte content, they do not prevent pulmonary edema should the fluid absorbed be excessive. Those fluids without electrolytes pose another problem (lack of electrolytes) to the patient if excessive absorption occurs. Therefore, it is important both to measure fluid deficit and be cognizant that the lack of electrolytes permits less fluid to be absorbed by the patient, because lack of electrolytes may precipitate fluid overload and cause hyponatremia.
Although Hyskon is most useful for operative hysteroscopy, particularly with mechanical tools or lasers, it is cumbersome to use with electrosurgery because it produces caramelization around electrodes and instruments, causing the need for frequent cleaning and replacement, and its viscosity does not permit retrieval after infusion. With any method, however, the amount of fluid must be carefully monitored to prevent excessive intravasation resulting in fluid overload, pulmonary edema, and coagulopathies.
Because of its viscosity, Hyskon must be injected under pressure, with a 50-mL plastic syringe connected to the inflow port of the hysteroscope. Alternatively, a mechanical pump is available to perform this task automatically.
TECHNIQUE OF OPERATIVE HYSTEROSCOPY AND RESECTOSCOPY
Technique of Operative Hysteroscopy
Once the patient is selected for operative hysteroscopy, the technique does not vary, whether performed under local, regional, or general anesthesia. The patient is placed in the dorsal-lithotomy position, and the vulva, vagina, and cervix are cleaned with an antiseptic solution. A vaginal speculum with an open side is introduced, and the cervix is grasped anteriorly with a single-tooth tenaculum. The cervical canal is then gradually dilated to number 7 or 8 Hegar, depending on the outer diameter of the instrument. The hysteroscope attached to its light source, then irrigating solution is introduced atraumatically. When an obturator is used, the outer sheath and the obturator are gently passed through the endocervical canal up to the internal cervical os, where the obturator is removed and replaced with a bridge and telescope. When low-viscosity fluids are used, a polyethylene catheter of 2.4 mm OD and 1.6 mm ID is introduced up to the end of the hysteroscope, and then the distending fluid is run under pressure, washing out mucus, debris, and blood clots. Once a complete evaluation of the uterine cavity has been performed, the specific operative procedure begins. When the operative hysteroscope has only one operating channel, the polyethylene catheter must be removed before insertion of the operating instrument.
When video cameras are used, it is important to maintain the camera in one position and to manipulate the hysteroscope clockwise and counterclockwise to visualize the uterine cavity aided by the Foroblique view of the telescope.
Laparoscopy, if necessary to monitor the hysteroscopic operation and/or evaluate the pelvic organs, should be performed first in the sequence. Then, while the laparoscope is in place, hysteroscopy and hysteroscopic surgery can be performed. Dimming the light of the laparoscope permits the assistant to observe the translucency of the hysteroscopic light.
Technique of Resectoscopy
With the resectoscope, a similar technique is used. The instrument is assembled, and an obturator is used to insert the two assembled concentric cannulas in the endocervical canal until the internal cervical os is reached. The obturator is then removed and replaced with the operating bridge and telescope. The inflow high-flow urologic tube is connected to the inner cannula, and the tubing for exit is also attached to the outer port of the resectoscope to collect the fluid. When the appropriate electrode has been selected, the system is activated by opening the inflow and outflow ports. It is important to wait for a continuous flow of the distending fluid so the uterine cavity is cleansed of blood clots and debris before beginning an evaluation or operation. The proper energy source and power must be selected and the electrical cord connected to the resectoscope. With monopolar current, the patient should be appropriately grounded with a returning plate system. Only fluids without electrolytes should be used.5,6
During the procedure, inflow and outflow should be monitored carefully to determine the amount of fluids lost during the operation.
THERAPEUTIC APPLICATIONS OF HYSTEROSCOPY
The therapeutic applications of hysteroscopy are rapidly expanding, in great part because of the improvement in instrumentation, improvement in energies and delivery systems of the distending media, and availability of video systems that enhance visualization with added magnification (Table 1).
Table 1. Therapeutic applications of hysteroscopy
Targeted biopsies
Removal of endometrial polyps
Removal of submucous leiomyomas
Division of uterine septa
Removal of “lost” IUDs and other foreign bodies
Lysis of intrauterine adhesions
Endometrial ablation(laser, electrosurgery)
Tubal cannulation (tubal obstruction)
Chorionic villus sampling
Tubal occlusion (electrocoagulation, cryocoagulation, chemical mechanical)
Hysteroscopic Biopsies Under Visual Control
Biopsy of an abnormal endometrial lesion is essential, particularly a lesion suspected to be malignant or premalignant. Hysteroscopy offers the possibility of choosing the area in need of biopsy. A biopsy forceps of sufficient diameter to allow appropriate tissue sample should be used; when appropriate, several biopsies of the same lesion should be taken to obtain adequate specimens.
Removal of Intrauterine Foreign Bodies
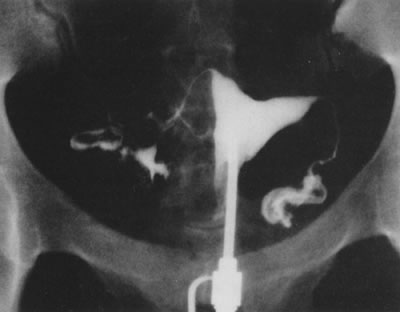
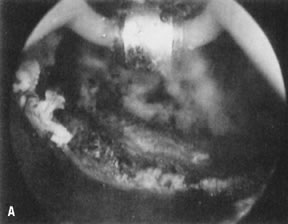
Hysteroscopy is the best method of removing partially embedded or fragmented intrauterine devices (IUDs) misplaced within the uterine cavity. Using a semirigid or rigid grasping forceps, this can be accomplished easily by grasping the device or its tail, and withdrawing the hysteroscope once the device is fixed at the end of the endoscope. Removal of these devices under visual control prevents unnecessary trauma to the uterus by blind manipulations and permits visual appraisal of the condition of the device regarding embedment or fragmentation (Figs. 19 and 20).7
|

|

Hysteroscopic Removal of Endometrial Polyps and Submucous Leiomyomas
A polyp can be removed by blind methods, including forceps or curettes, but the diagnosis can be obtained consistently only by direct visualization. By visually detecting the polyps, it is easy to detach them from the endometrial cavity by hysteroscopy, and their removal is simple. By whatever method they are removed, it is important to check that the total polyp has been removed, because often only a portion of the polyp is detached from its anchoring pedicle.
Although large endometrial polyps, particularly when pedunculated, are easily removed by hysteroscopic guidance, the removal of submucous leiomyomas requires more experience. Several methods are available. When the leiomyoma is smaller than 2 to 3 cm and is pedunculated, mechanical transection of the pedicle expedites its removal. Nonetheless, myomas larger than 3 cm with thick pedicles, or sessile myomas, must be removed by segmental shavings with a resectoscope and a cutting loop. This is performed systematically until the uterine wall is reached, when resection should stop. With experience, the endoscopist learns tactile appraisal provided by the resecting loop to distinguish fibrous myomatous tissue from myometrium. In addition, he or she can visually appraise the fibrotic tissue and the fascicularis aspect of the myometrium. When myomas penetrate deeply into the uterine wall, laparoscopy should be considered to monitor the hysteroscopic-resectoscopic operation transabdominally (Color Plate 1A to F; Figs. 21, 22, 23, 24, 25, and 26).8, 9, 10, 11, 12, 13, 14, 15, 16, 17
|

|

|
|
|

|

|
The Nd:YAG laser or other fiberoptic lasers (e.g., the argon or KTP-532) can also be used as operating instruments to transect the pedicle of a pedunculated leiomyoma or to aid in morcellation, particularly for larger leiomyomas located at the fundal region, which may be difficult to remove with a resectoscope.18
The advent of gonadotropin-releasing hormone (GnRH) analogues has facilitated the treatment of larger leiomyomas by reducing their size and vascularity. It has provided a method of preoperatively controlling the bleeding in patients with submucous myomas. This allows better preparation of the uterine cavity for resectoscopy, by causing atrophy of the endometrium. The patient is able to reestablish preoperatively normal physiologic iron stores and hemoglobin and hematocrits once bleeding ceases.19
Another adjunct in the management of patients with submucous myomas has been vaginal sonography to evaluate the uterine walls for other leiomyomas (size, number, and location) and to evaluate the submucous leiomyoma for penetration into the uterine wall, measuring thickness as a guide for resectoscopic removal to avoid shaving small portions of an intramural myoma that merely impinge on the uterine cavity (Table 2).20
Table 2. Hysteroscopic myomectomy for abnormal bleeding
Type of Myomas | |||||||||
Author | No. Patients | Pedunculated | Sessile | Method | IUD* | E/P† | Antibiotics | Cure (%) | Recurrent (%) |
Haning et al. (1980) | 1 | – | + | Resectoscope | – | + | + | 1 | – |
DeCherney and Polan (1983) | 8 | + | + | Resectoscope | Foley | + | + | 8 | – |
Neuwirth (1983) | 28 | + | + | Resectoscope | Foley | + | + | 17 (60.7) | 8 (28.5) |
Lin et al.(1986) | 13 | + | – | Resectoscope (9) | Foley | + | + | 9 (69.2) | 4 (30.7) |
Hallez and Perino (1988) | 300 | + | + | Resectoscope | + | + | + | 299‡ | – |
Baggish (1989) | 23 | + | + | Nd:YAG Laser | Foley (5 patients) | – | + | NR§ | NR§ |
Valle (1990) | 52 | + | – | Semi-rigid scissors | – | – | – | 52 (100.0) | 12 (20.0) |
Donnez et al. (1990) | 60 | 48 | 12 | Nd:YAG laser | – | – | – | 48 (80.0) | 12 (20.0) |
Loffer (1990) | 53 (10 were polyps) | 18 | 25 (2 patients had 2 procedures) | Resectoscope | NR§ | – | – | 40 (93.0) | 3 (6.9) |
Corson and Brooks (1991) | 92 | 92 | – | Resectoscope | NR§ | – | + | 65 (81.2)# | 15 (18.7)# |
Derman et al. (1991) | 94 | 94 (2 intraoperative laparotomies) | – | Resectoscope | Rubber balloon | + | + | 69 (75.0) | 23 (24.5) |
Wamsteker et al.(1993) | 51 | 25 | 26 (several patients had 2–3 procedures) | Resectoscope | – | – | + | 48 (94.1) | 3 (5.9) |
Emanuel et al. (1999) | 285 | 73 | 266 | Resectoscope | – | – | + | 225 (78.8)¶ | 41 (14.4) |
Totals | 1040 | 881 (81.2) | 109 (10.5) | ||||||
*IUD, Intrauterine device
†E/P, Estrogen/Progesterone
‡1 patient required laparotomy
§NR, Not Reported
#From 80 patients
¶17 lost to follow up
Modified from Siegler AM, Valle RF: Therapeutic hysteroscopic procedures. Fertil Steril 50:685, 1988.
Division of Symptomatic Uterine Septa
Uterine septa may be the cause of reproductive problems, particularly miscarriages, in about 20% of women affected by these uterine anomalies.21 Hysteroscopy has been used successfully to treat these conditions by simple transection or by coagulation-resection. Uterine remnants have poor visualization, seldom bleed upon division, and therefore can be easily divided under hysteroscopic view. Before hysteroscopy is attempted, however, laparoscopic or ultrasonographic examination of the uterus is mandatory to rule out a bicornuate uterus. Furthermore, concomitant laparoscopy helps the hysteroscopist in the transection of a uterine septum to avoid possible injury to the fundal area of the uterus, once the septum has been divided. Division of the uterine septum is relatively easy when the septum is thin and partial, but broad septa that extend the total length of the uterine corpus are challenging and require experience in operative hysteroscopy. The septum is transected systematically in the midline, avoiding drifting to the posterior or anterior wall. By advancing the hysteroscopic division of the septum systematically and visualizing the tubal openings, the hysteroscopist becomes aware of myometrial thickness. When the junction between the septum and myometrium begins, small arteries may be seen pulsating. If these are cut, they bleed upon division, indicating that the septum has been transected completely. With the symmetric visual view of the uterotubal junctions and the laparoscopic uniform translucency of the hysteroscopic light, the hysteroscopist can safely transect the uterine septum without danger of perforation.
At the completion of the procedure, the intrauterine pressure produced by the distending fluid may be lowered to less than 50 mmHg, and areas of bleeding may be observed. Usually, small bleeders stop on their own, but if the number of active arterial bleeders is significant, these can be individually coagulated with a pinpoint electrode (Figs. 27, 28, and 29).22, 23, 24, 25
|

|

|
The resectoscope may also be used to transect the septum, adding the advantage of coagulation-transection, which is most beneficial when dealing with very broad septa. A special straight knife or a loop oriented forward can be used for this purpose, using the blended current for simultaneous cutting and coagulation. Care should be taken not to overcorrect the defect, because bleeding may not be a warning sign of invading myometrium when blended current (cutting/coagulating) is used. Only fluids without electrolytes should be used, and laparoscopic monitoring is most helpful (Fig. 30).26
|
The uterine septum can also be transected using fiber lasers. The Nd:YAG adapted with a sculptured or extruded tip cuts on contact; the argon or KTP-532 can also be adapted with a sharp fiber. Precautions similar to those when using an electrical knife should be undertaken to avoid uterine perforation.27, 28
It is important to evaluate patients with pregnancy wastage who also have uterine septa, to rule out genetic, endocrine, or metabolic problems. The best indication for the hysteroscopic treatment of a uterine septum is pregnancy wastage. This operation is relatively simple, and division of the uterine septum seems most reasonable in infertile patients who need to undergo laparoscopy for unexplained infertility, and in patients who are candidates for insemination and have a uterine septum. Similarly, patients who require in vitro fertilization or any other reproductive technology procedure may benefit from hysteroscopic treatment of the septum, even if they never have achieved a pregnancy.
The results of hysteroscopic surgery for the uterine septum in terms of reproductive outcome have been encouraging, comparing well with and even surpassing previous results of abdominal metroplasties. The hysteroscopic treatment of the symptomatic uterine septum is the method of choice to treat this condition because of the obvious gains in performing this operation endoscopically, particularly avoiding laparotomy and hysterotomy and their accompanying morbidity; the decrease in hospitalization and inconvenience for the patient; the decrease in cost; and the avoidance of a routine cesarean section (Table 3).29, 30, 31, 32, 33, 34
Table 3. Hysteroscopic metroplasty
Pregnancy | ||||||||||
Author | No. patients | Medium | Technique | IUD* | E/P† | Antibiotics | Term | Premature | Abortion | In Progress |
Edstrom (1974) | 2 | Dextran 70, 32% | Rigid biopsy forceps | + | + | – | – | 19 weeks | – | – |
Chervenak and Neuwirth (1981) | 2 | Dextran 70, 32% | Scissors adjacent to hysteroscope | + | + | + | 1 | – | – | – |
Rosenberg et al. (1981) | 1 | Dextran 70, 32% | Flexible scissors | N/A‡ | N/A‡ | N/A‡ | N/A‡ | – | – | – |
Daly et al. (1983) | 25 | Dextran 70, 32% | Flexible scissors | – | + | – | 7 | – | 1 | – |
Perino et al. (1985) | 11 | CO2 | Flexible, semi-rigid scissors | + | – | – | N/A‡ | – | – | – |
DeChemey et al. (1986) | 72 | Dextran 70, 32% | Resectoscope | – | – | – | 58 | – | 4 | 4 |
Corson and Batzer (1986) | 18 | Dextran 70, 32% CO2 | Resectoscope and rigid scissors | – | – | – | 10 | 1 | 2 | 2 |
Fayez(1986) | 19 | Dextran 70, 32% | Rigid scissors | Foley Catheter | – | + | 14 | – | – | – |
March and Israel (1987) | 91 | Dextran 70, 32% | Flexible scissors | + | + | – | 44 | 4 | 7 | 7 |
Valle (1987) | 59 | D5W/Dextran 70, 32% | Flexible, semi-rigid | – | + | + | 44 | 2 | 5 | – |
Choe and Baggish (1992) | 19 | Dextran 70, 32% | Nd:YAG with bare or sculptured fibers | Foley Catheter | + | + | 10 | 1 | 1 | 3 |
Fedele et al. (1993) | 102 | Dextran 40, 10% in normal saline | Semi-rigid scissors (80) | +(21) | +(39) | + | 45 | 10 | 11 | NA‡ |
Valle (1996) | 124 | D5 in 1/2 saline | Semi-rigid scissors (98) | – | + | + | 84 | 7 | 12 | - |
Totals | 545 | 317 (78.3%) | 26 (6.4%) | 43 (10.6%) | 18 (4.4%) | |||||
*IUD, intrauterine device
†E/P, Estrogen/Progesterone
‡NA, Not Applicable
Modified from Siegler AM, Valle RF: Therapeutic hysteroscopic procedures. Fertil Steril 50:685, 1988.
Treatment of Intrauterine Adhesions
Hysteroscopy is the standard method for treatment of intrauterine adhesions; it allows for selective division of adhesions without damaging the surrounding healthy endometrium and offers an excellent alternative to reestablish the symmetry and architecture of the uterine cavity. The use of semirigid hysteroscopic scissors has improved lysis of adhesions when the adhesions are extensive and composed of thick connective tissue and/or are located at the uterotubal cones. In this situation, because of the thinning of the uterine wall, laparoscopy is mandatory to monitor the dissections and warn the hysteroscopist of perforation. Tubal patency is evaluated, and peritoneal and adnexal adhesions are assessed and frequently treated endoscopically.35, 36, 37, 38
Although alternative methods for the surgical transection of adhesions can be used, such as the resectoscope and/or fiber lasers with a low energy output, the mechanical approach using hysteroscopic scissors seems more logical, particularly to avoid peripheral damage to the remaining healthy endometrium, which will be the reservoir for rapid uterine cavity reepithelialization after treatment (Figs. 31, 32, 33, 34, and 35; see Color Plate 1G, ).39, 40
|

|

|
|
|

When adhesions are extensive and composed of fibrotic connective tissue, a uterine splint in the form of a No. 8 pediatric indwelling catheter, with 3 or 3.5 mL of saline, is placed inside the uterine cavity after the division of adhesions and is left in place for a week. Concomitant prophylactic antibiotics are used during and after the procedure, particularly when splints are left in place. Vibramycin is given 100 mg twice daily orally for a week, or intraoperative cefazolin (Kefzol) 1 g IV is given, followed by cephalexin (Keflex) 500 mg four times daily orally for 6–7 days. To aid reepithelialization, oral conjugated estrogens are prescribed (Premarin 2.5 mg twice daily for a 30-day cycle) with terminal progesterone, medroxyprogesterone acetate (Provera) 10 mg per day orally for the last 5 days of the artificial cycle to allow withdrawal bleeding. When total uterine cavity occlusion has been treated, this cycle may be repeated once or even twice.
At the completion of the hormonal treatment, a hysterosalpingogram is performed to assess the uterine cavity to determine if further surgery may be necessary or if the patient may be allowed to attempt conception.
The cumulative results reported with hysteroscopic treatment of intrauterine adhesions have shown the reestablishment of normal menstruation in over 90% of the patients treated. Nonetheless, the reproductive outcome has paralleled the severity of the disease, with an overall pregnancy rate of 60% to 70%, demonstrating that the more extensively the uterine cavity is occluded by adhesions, and the older the adhesions are, the poorer the prognosis is (Table 4).41, 42, 43, 44
Table 4. Hysteroscopic lysis of intrauterine adhesions*
Reproductive outcome | ||||||
Menses normal | Pregnancy | Term | ||||
Author | No. patients | Medium | Technique | No. (%) | No. (%) | No. (%) |
Levine and Neuwirth (1973) | 10 | Hyskon | Flexible scissors | 5 (50) | 2 (20) | – |
Edstrom (1974) | 9 | Hyskon | Biopsy forceps | 2 (22) | 1 (11) | 1 (11) |
Siegler and Kontopoulos (1981) | 25 | CO2 | Target abrasion/scissors/ curettage | 13 (52) | 11 (44) | 12 (44.4) |
March and Israel (1985) | 38 | Hyskon | Flexible scissors | 38(100) | 38 (100) | 34 (79.1) |
Neuwirth et al. (1982) | 27 | Hyskon | Scissors alongside | 20 (74) | 14 (51.8) | 13 (48.1) |
Sanfilippo et al. (1982) | 26 | CO2 | Curettage | 26 (100) | 6 (100) | 3 (50) |
Hamou et al. (1983) | 69 | CO2 | Target abrasion | 59 (85.5) | 20 (51.3) | 15 (38.4) |
Sugimoto et al. (1984) | 258 | Hyskon/normal saline | Target abrasion/Kelly forceps | 180 (69.7) | 143 (76.4) | 114 (79.7) |
Wamsteker (1984) | 36 | Hyskon | Scissors/biopsy forceps | 34 (94.4) | 17 (62.9) | 12 (44.4) |
Friedman et al. (1986) | 30 | Hyskon | Resectoscope/scissors | 27 (90) | 24 (80) | 23 (76.6) |
Zuanchong and Yulian (1986) | 70 | Normal saline | Biopsy forceps/flexible scissors | 64 (84.3) | 30 (85.7) | 17 (48.5) |
Valle and Sciarra (1988) | 187 | D5 W/Hyskon | Flexible/semirigid/rigid scissors | 167 (89.3) | 143 (76.4) | 113 (79.7) |
Lancet and Kessler (1988) | 98 | Hyskon | Felxible scissors/ electosurgery | 98 (100) | 86 (87.8) | 77 (89.5) |
Pabuccu et al. (1999) | 40 | Glycine | Murphy probe scissors | 33 (82.5) | 27 (67.5) | 23 (57.5) |
Feng et al. (1999) | 365 | Dextrose 5% | Biopsy forceps/scissors | 294 (83.7) | 156 (83.8)* | 145 (92.9) |
Totals | 1298 | 1060 (87.5) | 718 (72.3) | 603 (87.2) | ||
*Of 186 desiring pregnancy
Modified from Siegler AM, Valle RF, Lindemann HJ. et al. Therapeutic Hysteroscopy. Indications and Techniques, p. 103. St Louis, CV Mosby, 1990.
Hysteroscopic Tubal Cannulation
Fallopian tube obstruction is a significant cause of infertility in about 30% of infertile women. Proximal obstruction of the fallopian tubes occurs in about 10% to 20% of women who undergo hysterosalpingography as part of their infertility evaluation.45, 46 Laparoscopy is used to rule out physiologic spasms and to evaluate other fallopian tube or pelvic pathology. When proximal fallopian tube obstruction is confirmed by laparoscopy, surgical reconstruction can be used to treat this condition. Because patients operated on for this condition do not consistently show fibrosis of the occluded area, but often show simple occlusion or obstruction by debris or proteinaceous material plugging the tubal lumen, as demonstrated by Sulak and colleagues,47 tubal cannulation has been used as the initial method to treat these patients.
New soft, small-caliber catheters have significantly facilitated this procedure, adapting angiographic techniques with coaxial catheters to cannulate the fallopian tubes (see Color Plate 1H).
The hysteroscopic approach offers the advantage of ruling out tubal spasms under laparoscopy and guiding catheters directly into the fallopian tubes under direct vision. The concomitant use of laparoscopy allows assessment of tubal patency and provides an opportunity to evaluate and/or treat other pelvic conditions, such as pelvic adhesions and endometriosis.
Tubal cannulation has variations, particularly the use of straight coaxial catheters versus catheters with distal balloons to distend the cornual tubal regions; from the published data, however, the outcome does not vary with these techniques, and the simplicity of simple coaxial catheters to cannulate the fallopian tubes makes them attractive to the practitioner. Although dilatation of a vessel to flatten an atheroma is useful, in the intramural portion of the fallopian tubes in which the obstruction must be released, dilatation is not necessary because the fallopian tube quickly recovers its normal anatomy after distention.48, 49, 50, 51, 52
The results of tubal cannulation are promising. The successful visualization of the fallopian tubes at cannulation by hysteroscopy has shown a 70% to 92% patency. The intrauterine pregnancy rate was about 47%, and the ectopic pregnancy rate about 8%, in 50 patients after a follow-up period of 12 months.53, 54, 55, 56, 57, 58
Only those patients who fail tubal cannulation and who demonstrate true fibrotic occlusion require microsurgical tubal reconstruction (Table 5).59
Table 5. Results of hysteroscopic cannulation of proximal tubal obstruction
Author | No. of | Catheter | Complications | Pregnancies |
Confino et al. (1986)50 | 1/0 | Balloon | 1 | — |
Daniell and Miller (1987)51 | 1/0 | Urologic | 0 | 1 |
Sulak et al. (1987)52 | 2/0 | Epidural | 0 | 1 |
Confino et al. (1988)53 | 12/5 | Balloon | 3 | 2 |
Novy et al. (1988)54 | 10/1 | Cornual set | 1 | 2 |
Deaton et al. (1990)55 | 11/4 | Urologic | 2 | 6 (3 ectopic) |
Lin et al. (1990)56 | 10/0 | Urologic | — | 5 (1 ectopic) |
Flood and Grow (1993)57 | 27/3 | Cornual set | 4 | 15 |
Total | 74/13 (17.5%) | 11 (14.8%) | 32 (43.2%) |
Although most tubal cannulations can be performed with a rigid operative hysteroscope, the introduction of flexible operative hysteroscopes with a 4.9-mm OD offers a useful alternative for tubal cannulation, particularly when the tubal openings are angulated and difficult to localize with rigid endoscopes, and anatomic variations in the uterine configuration make localization difficult. The steerability of these endoscopes greatly facilitates tubal cannulation by aligning the endoscope in direct opposition to the proximal tubal ostia, simplifying the procedure and reducing failures.
Endometrial Ablation
Significant numbers of patients undergo hysterectomy for treatment of abnormal uterine bleeding of a nonorganic origin that fails to respond to hormonal treatment. Many attempts to use conservative methods to treat bleeding without a hysterectomy have failed. Recently, endometrial destruction by laser energy or electrosurgery has been used to accomplish this objective in an ambulatory setting. Because the number of women requiting this treatment is substantial (it has been calculated that more than 700,000 hysterectomies are performed annually in the United States, and of those, 20% may be due to dysfunctional uterine bleeding), conservative alternatives for treatment have a major role.60, 61
There are two methods of accomplishing endometrial ablation: laser endometrial ablation and electrosurgical endometrial ablation.
LASER ENDOMETRIAL ABLATION.
Laser endometrial ablation is performed with the Nd:YAG laser, with a wavelength of 1064 nm, in the near infrared (invisible) portion of the light spectrum. This laser is useful for endometrial ablation both because of its penetration of 4–5 mm and because it can be transferred through fluids without losing its energy. Because of its special property of frontal, lateral, and back scattering, which creates deep craters in the tissue when applied in contact with the tissue, it helps in the destruction of the endometrium and of the superficial portion of the myometrium.
The technique of laser endometrial ablation requires an operative hysteroscope and fluids with electrolytes, specifically sodium, because of the time required for the procedure and the large amount of fluids necessary during this procedure. The “bare” quartz fiber, 0.6 mm in diameter, is introduced, after it has been tested for spot size and functioning, and the endometrial ablation begins. Two techniques are available to complete this task. One is the “dragging” or touch technique, accomplished by direct contact between the bare quartz fiber and the tissue: first the uterotubal cornual junctions and then the anterior and posterior uterine walls. Care should be taken not to destroy the endocervical tissue to avoid cervical stenosis (Fig. 36).62
|
The second technique, the nontouch or “blanching” technique, can be used by firing the laser with a quartz fiber 1 or 2 mm away from the tissue. This is particularly useful at the uterotubal cones, where the thinnest portion of the myometrium may reach only 3.5 to 4 mm. With blanching, it is often difficult to differentiate between tissue that has been coagulated and tissue that has not been coagulated; therefore, it is important to divide the uterine cavity in segments to permit more systematic endometrial destruction. Many physicians prefer a combination of these two techniques, using the nontouch technique at the cornual regions and accomplishing the rest by the dragging or touch technique (Fig. 37).63, 64, 65
|

The results of endometrial ablation with the Nd:YAG laser show a 95% resolution of the abnormal bleeding and about a 5% failure rate. The aim of this procedure is not to create amenorrhea but to resolve the abnormal, excessive uterine bleeding.66
ENDOMETRIAL ABLATION BY ELECTROSURGERY.
Using the resectoscope and a special electrode, the endometrium may be resected or coagulated. The initial technique to accomplish endometrial destruction was resection with use of the loop electrode. The difficulty in maintaining a uniform depth of resection makes this technique cumbersome, however. Furthermore, because resection could predispose to more fluid intravasation and immediate postoperative bleeding, physicians were prompted to use the alternative method of endometrial coagulation with thicker roller-bar or roller-ball electrodes, which can accomplish endometrial destruction just by coagulation. This technique is simpler, faster, and as effective as resection, and the instrumentation and electrical power units required are less expensive than those required for laser ablation. In general, pure coagulating current of 40 to 50 W or, alternatively, pure cutting current of 100 to 120 W, can be used to accomplish this procedure. Because the electrical current used is unipolar, grounding of the patient is necessary to complete the electrical circuit, and no electrolytes should be used with the distending media. The possibility of fluid overload and water intoxication must be carefully monitored, measuring precisely the inflow and outflow of fluids used and deducting the deficit of fluid not recovered.67, 68, 69, 70, 71, 72, 73, 74
The results obtained with endometrial ablation by electrosurgery are similar to those achieved with lasers. Nonetheless, it seems that the failure rate is slightly higher (5% to 10%), as one would expect, because electrosurgery may not be as predictable as the laser energy, particularly when visual appraisal of the thermal damage cannot predict uterine wall penetration (Fig. 38).66, 74, 75
|

All patients undergoing endometrial ablation benefit from hormonal preparation to stop bleeding and produce atrophy of the endometrium, making the actual technique simpler and more efficacious. The thinner the endometrium, the better the chance of penetrating the superficial portion of the myometrium and destroying those deeper glands that may be the source of reepithelialization. Although progesterones occasionally have been used to atrophy the endometrium, the pseudodecidual reaction they produce impairs visualization, and the response of the endometrium is somewhat erratic. Danazol 800 mg a day for 4 to 6 weeks has also been used, although patient compliance is not as uniform because of its side effects. Leuprolide acetate (Lupron) is an excellent alternative and can be given in its depot form 3.75 mg IM with two doses 1 month apart; the operation is performed 2 to 3 weeks after the second injection. Alternatively, a 7.5-mg IM depot injection can be used as a single dose, although some patients may not achieve enough endometrial atrophy despite the shortening of the flare-up phase of these agonists.66
Complications of Operative Hysteroscopy
Operative hysteroscopy involves the possibility of serious complications, as compared with diagnostic hysteroscopy. Uterine perforation, fluid overload from distending media, infection, and associated injuries related to laser or electrosurgical energies are the most common complications related to operative hysteroscopy.
Operative hysteroscopy requires experience in diagnostic hysteroscopy and should not be undertaken as the first step in any hysteroscopic therapeutic procedure. Necessary instrumentation should be available and precautions taken, such as concomitant laparoscopy for extensive operative procedures that risk uterine perforation. Operative hysteroscopy is best performed in the operating room with the patient under general anesthesia, except when minor interventions are performed, such as the removal of IUDs, biopsy of some endometrial lesions, and division of mild filmy adhesions that only partially connect the uterine walls.
The manipulation of instruments within the uterine cavity, therefore, should be performed with caution and delicacy, and when difficult manipulations are necessary, concomitant laparoscopy should be liberally used.
The distending media, particularly low-viscosity fluids, should be carefully monitored as to the amount infused and the amount recovered, to measure serially the deficit of these fluids, particularly when fluids without electrolytes are used. When the operations are prolonged or require significant dissections, urine output should be monitored, as well as vital signs and pulse oximetry, in conjunction with the anesthesiologist. Prudent use of diuretics when necessary may be helpful, and the operation should be stopped should any of these variables be abnormal.76, 77, 78, 79
Bleeding may occur during an operative procedure, particularly during the division of a uterine septum or the removal of a leiomyoma, and immediate hemostasis should be accomplished with either electrosurgery or mechanical tamponade. Although infection has not been a major problem for operative hysteroscopy, caution should be exercised in patients who undergo extensive operations, and prophylactic antibiotics should be used if deemed necessary, particularly in infertility patients and patients who may be at risk for infection.80, 81
Laser energy should not be used without knowledge of the physics and properties of these lasers as well as the interaction of these lasers with tissues. Safety measures should be taken to protect the operator from back-scattering of the fiberoptic lasers, using appropriate filters, safety goggles, or, alternatively, video systems as protection from retinal injuries. In addition, precautions should be taken to protect patients from deeper laser penetration to avoid uterine perforation. Similarly, electrosurgical energies should be used with caution and understanding of the biophysical properties of these energies. Specific precautions should be taken regarding the use of the different electrodes available and their properties, the effects on tissue, and the drawbacks.
When a patient has a background of specific indications and there are no contraindications, and when meticulous attention is paid to details in the different aspects of operative hysteroscopy, an operator can perform these techniques safely and with minimal or no complications.
SUMMARY AND CONCLUSIONS
The therapeutic applications of hysteroscopy have multiplied, and their efficacy has been increased and enhanced by the availability of modern instruments and new technology. Methods of uterine distention have been improved and their safety enhanced. Energy modalities such as laser and electrosurgery have been added to the armamentarium of operative hysteroscopy, extending the therapeutic applications even further.
Modern therapeutic hysteroscopic procedures have replaced invasive therapeutic approaches such as laparotomy and hysterotomy for metroplasties, microsurgical treatment of cornual fallopian tube obstruction, the removal of submucous leiomyomas, and the treatment of extensive intrauterine adhesions. Many other therapeutic applications are on the horizon, and perhaps with newer technological innovations a practical use of transcervical salpingoscopy and the application of hysteroscopy to new reproductive technologies such as zygote intrafallopian transfer (ZIFT), gamete intrafallopian transfer (GIFT), and intratubal insemination may be accomplished in the near future. Hysteroscopy remains a promising platform to one day achieve transcervical tubal sterilization.
REFERENCES
Edstrom KGB: Intrauterine surgical procedures during hysteroscopy. Endoscopy 6: 175, 1974 |
|
Sciarra JJ, Butler JC, Speidel JJ (eds): Hysteroscopic Sterilization. New York, Intercontinental Medical Book, 1974 |
|
Siegler AM, Valle RF, Lindemann HJ et al: Therapeutic Hysteroscopy. Indications and Techniques. St. Louis, CV Mosby, 1990 |
|
Valle RF: Therapeutic hysteroscopy in infertility. Int J Fertil 29: 143, 1984 |
|
DeCherney AH, Polan ML: Hysteroscopic management of intrauterine lesions and intractable uterine bleeding. Obstet Gynecol 61: 392, 1983 |
|
Neuwirth RS: Hysteroscopic management of symptomatic submucous fibroids. Obstet Gynecol 62: 509, 1983 |
|
Valle RF, Sciarra JJ, Freeman DW: Hysteroscopic removal of intrauterine devices with missing filaments. Obstet Gynecol 49: 55, 1977 |
|
Neuwirth RS: A new technique for an additional experience with hysteroscopic resection of submucous fibroids. Am J Obstet Gynecol 131: 91, 1978 |
|
Hallez JP, Netter A, Cattier R: Methodical intrauterine resection. Am J Obstet Gynecol 156: 1080, 1987 |
|
Siegler AM, Valle RF: Therapeutic hysteroscopic procedures. Fertil Steril 50: 685, 1988 |
|
Valle RF: Hysteroscopic removal of submucous leiomyomas. J Gynecol Surg 6: 89, 1990 |
|
Loffer FD: Removal of large symptomatic intrauterine growths by the hysteroscopic resectoscope. Obstet Gynecol 76: 836, 1990 |
|
Corson SL, Brooks PG: Resectoscopic myomectomy. Fertil Steril 55: 1041, 1991 |
|
Derman SG, Rehnstrom J, Neuwirth RS: The long-term effectiveness of hysteroscopic treatment of menorrhagia and leiomyomas. Obstet Gynecol 77: 591, 1991 |
|
Wamsteker K, Emanuel MH, de Kruif JH: Transcervical hysteroscopic resection of submucous fibroids for abnormal uterine bleeding: Results regarding the degree of intramural extension. Obstet Gynecol 82: 736, 1993 |
|
Donnez J, Gillerot S, Bourgonjou D et al: Neodymium:YAG laser hysteroscopy in large submucous fibroids. Fertil Steril 54: 1999, 1990 |
|
Emanuel MH, Wamsteker K, Hart AAM et al: Long-term results of hysteroscopic myomectomy for abnormal uterine bleeding. Obstet Gynecol 93: 743, 1999 |
|
Baggish MS, Sze EHM, Morgan G: Hysteroscopic treatment of symptomatic submucous myomata uteri with the Nd:YAG laser. J Gynecol Surg 5: 27, 1989 |
|
Perino A, Chianchiano N, Petronio M et al: Role of leuprolide acetate depot in hysteroscopic surgery: A controlled study. Fertil Steril 59: 507, 1993 |
|
Cohen L, Valle RF: Role of vaginal sonography and hysterosonography in the endoscopic treatment of uterine myomas. Fertil Steril 73: 1997, 2000 |
|
Valle RF: Clinical management of uterine factors in infertile patients. Semin Reprod Endocrinol 3:2, 149, 1985 |
|
Daly DC, Waiters CA, Soto-Albors CE et al: Hysteroscopic metroplasty: Surgical technique and obstetric outcome. Fertil Steril 39: 623, 1983 |
|
Valle RF, Sciarra JJ: Hysteroscopic treatment of the septate uterus. Obstet Gynecol 676: 253, 1986 |
|
Perino A, Mencaglia L, Hamou J et al: Hysteroscopy for metroplasty of uterine sepia: Report of 24 cases. Fertil Steril 48: 321, 1987 |
|
March CM, Israel R: Hysteroscopic management of recurrent abortion caused by septate uterus. Am J Obstet Gynecol 156: 834, 1987 |
|
DeCherney AH, Russell JB, Graebe RA et al: Resectoscopic management of mullerian fusion defects. Fertil Steril 45: 726, 1986 |
|
Candiani GB, Vercellini P, Fedele L et al: Argon laser versus microscissors for hysteroscopic incision of uterine septa. Am J Obstet Gynecol 164: 87, 1991 |
|
Choe JK, Baggish MS: Hysteroscopic treatment of septate uterus with neodymium-YAG laser. Fertil Steril 57: 81, 1992 |
|
Fayez JA: Comparison between abdominal and hysteroscopic metroplasty. Obstet Gynecol 68: 399, 1986 |
|
Daly DC, Maier D, Soto-Albors C: Hysteroscopic metroplasty: Six years experience. Obstet Gynecol 73: 201, 1989 |
|
Siegler AM, Valle RF, Lindemann HJ et al: Hysteroscopic metroplasty. In Siegler AM, Valle RF, Lindemann HJ et al: Therapeutic Hysteroscopy. Indications and Techniques, pp 62–81. St Louis, CV Mosby, 1990 |
|
Hassiakos DK, Zourlas PA: Transcervical division of the uterine septa. Obstet Gynecol Surv 5: 165, 1990 |
|
Fedele L, Arcaini L, Parazzini F et al: Reproductive prognosis after hysteroscopic metroplasty in 102 women: Life-table analysis. Fertil Steril 59: 768, 1993 |
|
Valle RF: Hysteroscopic treatment of partial and complete uterine septum. Int J Fertil 41: 310, 1996 |
|
Schenker JG, Margalioth EJ: Intrauterine adhesions: An updated appraisal. Fertil Steril 37: 593, 1982 |
|
March CM, Israel R, March AD: Hysteroscopic management of intrauterine adhesions. Am J Obstet Gynecol 130: 653, 1978 |
|
Valle RF, Sciarra JJ: Current status of hysteroscopy in gynecologic practice. Fertil Steril 32: 619, 1979 |
|
Valle RF, Sciarra JJ: Intrauterine adhesions: Hysteroscopic diagnosis, classification, treatment, and reproductive outcome. Am J Obstet Gynecol 158: 1459, 1988 |
|
Friedman A, Defazio J, DeCherney AH: Severe obstetric complications following hysteroscopic lysis of adhesions. Obstet Gynecol 67: 864, 1986 |
|
Newton JR, Mackenzie WE, Emens MJ et al: Division of uterine adhesions (Asherman's syndrome) with the Nd-YAG laser. Br J Obstet Gynaecol 96: 102, 1989 |
|
March CM, Israel R: Gestational outcome following hysteroscopic lysis of adhesions. Fertil Steril 36: 455, 1981 |
|
Siegler AM, Valle RF, Lindemann HJ et al: Intrauterine adhesions. In Siegler AM, Valle RF, Lindemann HJ et al: Therapeutic Hysteroscopy. Indications and Techniques, pp 82–105. St Louis, CV Mosby, 1990 |
|
Pabuccu R, Stay V, Orhion E et al: Hysteroscopic treatment of intrauterine adhesions is safe and effective in the restoration of normal menstruation and fertility. Fertil Steril 68: 1141, 1994 |
|
Feng ZC, Yang B, Shao J et al: Diagnostic and therapeutic hysteroscopy for traumatic intrauterine adhesions after induced abortions: A clinical analysis of 365 cases. Gynaecol Endosc 8: 95, 1999 |
|
Valle RF: Tubal cannulation. Obstet Gynecol Clin North Am 22: 519, 1995 |
|
Siegler AM: Hysterosalpingography. Fertil Steril 40: 139, 1983 |
|
Sulak PJ, Letterie GS, Coddington CC et al: Histology of proximal tubal occlusion. Fertil Steril 48: 437, 1987 |
|
Valle RF: Tubal catheterization for sterilization purposes. In Gleicher N (ed): Tubal Catheterization Procedures, pp 139–160. New York, Wiley, 1992 |
|
Thurmond AS, Novy M, Uchida BT et al: Fallopian tube obstruction: Selective salpingography and recanalization. Radiology 163: 511, 1987 |
|
Confino E, Friberg J, Gleicher N: Transcervical balloon tuboplasty. Fertil Steril 46: 963, 1986 |
|
Daniell JF, Miller W: Hysteroscopic correction of cornual occlusion with resultant term pregnancy. Fertil Steril 48: 490, 1987 |
|
Sulak PJ, Letterie GS, Hayslip CC et al: Hysteroscopic cannulation and lavage in the treatment of proximal tubal occlusion. Fertil Steril 48: 493, 1987 |
|
Confino E, Friberg J, Gleicher N: Preliminary experience with transcervical balloon tuboplasty. Am J Obstet Gynecol 159: 370, 1988 |
|
Novy MJ, Thurmond AS, Patton P et al: Diagnosis of cornual obstruction by transcervical fallopian tube cannulation. Fertil Steril 50: 434, 1988 |
|
Deaton JL, Gibson M, Riddick DH et al: Diagnosis and treatment of cornual obstruction using flexible tip guidewire. Fertil Steril 53: 232, 1990 |
|
Lin BL, Iwata Y, Liu KH et al: Clinical applications of a new Fujinon operating fiberoptic hysteroscope. J Gynecol Surg 6: 8l, 1990 |
|
Flood JT, Grow DR: Transcervical tubal cannulation: A review. Obstet Gynecol Surv 48: 768, 1993 |
|
Thurmond AS, Novy MJ: Transcervical fallopian tube catheterization for management of proximal tubal obstruction. In Winfield AC, Wentz AC (eds): Diagnostic Imaging in Infertility, pp 192–207. Baltimore, Williams & Wilkins, 1992 |
|
Valle RF: Hysteroscopy in the evaluation of infertility. In Winfield AC, Wentz AC (eds): Diagnostic Imaging in Infertility, pp 117–150. Baltimore, Williams & Wilkins, 1992 |
|
Wingo PA, Huezo CM, Rubin GL et al: The mortality risk associated with hysterectomy. Am J Obstet Gynecol 152: 803, 1985 |
|
Grant J, Hussein IY: An audit of abdominal hysterectomy over a decade in a district general hospital. Br J Obstet Gynaecol 91: 73, 1984 |
|
Goldrath MH, Fuller TA, Segal S: Laser photovaporization of the endometrium for the treatment of menorrhagia. Am J Obstet Gynecol 140: 14, 1981 |
|
Loffer FD: Hysteroscopic endometrial ablation with Nd:YAG laser using a non-contact technique. Obstet Gynecol 69: 679, 1987 |
|
Lomano JM: Dragging technique versus blanching technique for endometrial ablation with the Nd:YAG laser in the treatment of chronic menorrhagia. Am J Obstet Gynecol 159: 152, 1988 |
|
Baggish MS, Baltoyannis P: New techniques for laser ablation of the endometrium in high-risk patients. Am J Obstet Gynecol 159: 287, 1988 |
|
Valle RF: Endometrial ablation for dysfunctional uterine bleeding: Role of GnRH agonists. Int J Gynaecol Obstet 41: 3, 1993 |
|
DeCherney AH, Diamond MP, Lavy G et al: Endometrial ablation for intractable uterine bleeding: Hysteroscopic resection. Obstet Gynecol 70: 668, 1987 |
|
Rankin L, Steinberg LH: Transcervical resection of the endometrium: A review of 400 consecutive patients. Br J Obstet Gynaecol 99: 911, 1992 |
|
Dwyer N, Hutton J, Stirrat GM: Randomized controlled trial comparing endometrial resection with abdominal hysterectomy for the surgical treatment of menorrhagia. Br J Obstet Gynaecol 100: 237, 1993 |
|
Magos AL, Baumann R, Lockwood GM et al: Experience with the first 250 endometrial resections for menorrhagia. Lancet 337: 1074, 1991 |
|
Vancallle TG: Electrocoagulation of the endometrium with the ball-end resectoscope. Obstet Gynecol 74: 425, 1989 |
|
Towsend DE, Richart RM, Paskowitz RA et al: “Rollerball” coagulation of the endometrium. Obstet Gynecol 76: 310, 1990 |
|
McLucas B: Endometrial ablation with the roller ball electrode. J Reprod Med 35: 1055, 1990 |
|
Daniell JF, Kurtz BR, Ke RW: Hysteroscopic endometrial ablation using the rollerball electrode. Obstet Gynecol 80: 329, 1992 |
|
Onbargi LC, Hayden R, Valle RF et al: Effects of power and electrical current density variations in an in vitro endometrial ablation model. Obstet Gynecol 82: 912, 1993 |
|
Witz CA, Silverberg KM, Burns WN et al: Complications associated with the absorption of hysteroscopic fluid media. Fertil Steril 60: 745, 1993 |
|
Garry R, Hasham F, Kokri MS et al: The effect of pressure on fluid absorption during endometrial ablation. J Gynecol Surg 8: 1, 1992 |
|
Arieff AI, Ayus JC: Endometrial ablation complicated by fatal hyponatremic encephalopathy. JAMA 270: 1230, 1993 |
|
Baggish MS, Brill AI, Rosenweig B et al: Fatal acute glycine and sorbitol toxicity during operative hysteroscopy. J Gynecol Surg 9: 137, 1993 |
|
Peterson HB, Hulka JF, Phillips JM: American Association of Gynecologic Laparoscopists 1988 Membership Survey on Operative Hysteroscopy. J Reprod Med 35: 590, 1990 |
|
Hulka JF, Peterson HB, Phillips JM et al: Operative Hysteroscopy. American Association of Gynecologic Laparoscopists 1991 Membership Survey. J Reprod Med 38:572, 1993 |