Placenta Previa and Accreta
Authors
INTRODUCTION
Although relatively rare, placenta previa and accreta account for a large percentage of maternal morbidity and mortality in modern obstetrics. Hemorrhage is a major complication of abnormal placentation, and early diagnosis and intervention in these conditions can more readily enable the physician to minimize the risks to mother and fetus. The current widespread use of ultrasound in obstetrics has greatly advanced our ability to diagnose and manage abnormal obstetric bleeding.
CLASSIFICATION
Placenta previa is classified by the degree of encroachment upon the internal cervical os. In total placenta previa, the cervical os is completely covered by the placenta. In partial placenta previa, the cervical os is partly covered by the placenta. In marginal placenta previa, the edge of the placenta is considered to be at the margin of the internal os.
The term low-lying placenta has been used when the placental edge does not reach the cervical os, but is close enough to be palpated by an examiner's finger.1 The current distinction of low-lying placenta, however, does not rely on digital cervical examination. Instead, it is described as a placental edge that approaches to within 2 cm of the cervix on ultrasound examination. The most accurate measurement is obtained by endovaginal scanning.
Invasive placentas are classified according to the degree of myometrial invasion. In placenta accreta, the abnormally adherent placental villi are attached directly into the myometrium, but do not invade it. In a placenta increta, the villi invade the myometrium. When the placental villi penetrate through the myometrium, reaching the serosal surface of the uterus, then a placenta percreta is present (Fig. 1).
|
INCIDENCE
It is well established that the incidence of placenta previa increases with advancing age and higher parity. Surgical history, especially if a previous cesarean section was performed for placenta previa, is linked to recurrent development of placenta previa and, more importantly, placenta accreta. Most studies report an overall incidence of placenta previa between 1 in 150 and 1 in 300 patients (3–6/1000).2, 3, 4, 5, 6, 7, 8, 9, 10, 11 Placenta previa has been reported to result in maternal death in 3/1000 cases, and also has been noted to predispose patients to abruptio placenta.6
Placenta accreta, increta, and percreta occur much less frequently, from 1 in 1600 to 1 in 12,000 patients.3, 4, 12, 13, 14, 15, 16, Placenta accreta occurs most commonly, followed in decreasing frequency by placenta increta and placenta percreta.17, 18 For our purposes, we refer to all three conditions under placenta accreta. Confirmation of placenta accreta requires histopathologic methods, and so it is possible that incidence is underreported when the condition is focal or not associated with performance of a hysterectomy. Likewise, in cases of retained placenta where manual removal or sharp curettage is necessary, it is difficult to make the diagnosis of placenta accreta as there is no uterine specimen for pathological diagnosis. Placenta accreta often occurs in combination with placenta previa. In the presence of placenta previa, accreta will also be noted in 24–67% of cases, increasing with the number of prior uterine scars.4
These abnormalities of placentation are ominous conditions, contributing significantly to maternal morbidity and mortality12 and accounting for 1.7% of all maternal deaths in the United States.19 The association of both placenta previa and placenta accreta with extensive maternal hemorrhage and transfusion is well documented. The unfortunate sequela of this connection is that in order to achieve hemostasis, many women may require emergent hysterectomy with its inherent surgical risks, additional blood loss, and subsequent loss of reproductive capacity.
As preterm intervention and delivery is often required in cases of placenta previa or placenta accreta, these conditions become significant contributors to perinatal morbidity and mortality as well, accounting for as many as 24% of perinatal deaths.20 In one study, up to 11% of previas were fatal to the fetus or neonate, with coexisting abruptio placenta in 41% of cases.8 Placenta accreta in the presence of placenta previa has been reported to account for a mortality rate of 1 death in 2400 births.
ETIOLOGY/PATHOGENESIS
The etiologies of placenta previa and accreta are not well understood; however, several hypotheses have been advanced. Placenta previa is noted more often in the second trimester, and frequently resolves as the pregnancy progresses.21 For this reason, a widely accepted view is that there normally exists an apparent placental migration, with one edge of the placenta growing while the opposite edge atrophies. It has been noted that the placenta initially will occupy from one half to one third of the uterine wall. By term, however, no more than one fourth to one sixth of the uterine surface is covered.22 This change in ratio permits a degree of apparent placental movement. In placenta previa, it is postulated that there is an impairment of this normal placental progression away from the cervical os. It is believed that this migration is impaired in women with surgically scarred uteri, which is why they are at greater risk for placenta previa. The uterus itself is made up of several different areas, with differential growth rates of each area. In the first 7 months of pregnancy, the relatively muscular upper portion of the uterus grows faster than the lower segment. Toward the end of pregnancy, the lower segment begins to develop, and can grow quite rapidly. Failure of this differential growth may occur when the lower uterine segment is scarred, also contributing to the occurrence of a placenta previa.4
Smoking seems to increase the risk of previa via a hypoxemia-related mechanism. Nicotine has a vasoconstricting effect on uteroplacental perfusion in smoking mothers. Placental studies have demonstrated decreased vascularization and pronounced changes in the broad basement membrane of mothers who smoked cigarettes.23 Tominaga and Page24 have postulated that increasing the placental surface area would be an effective method of coping with the relative hypoxia experienced by smokers. This hypothesis is supported by observations that in comparison with nonsmokers, mothers who smoke have heavier, thinner placentas with larger surface areas.25 Increased carbon monoxide combined with hypoxemia may result in compensatory placental hypertrophy, which may also increase the likelihood of placental encroachment on the cervical os.26 There is a strong similarity between the changes seen in smoking mothers and those seen at high altitudes.27 This supports the theory that hypoxia is a determinant of placenta previa in mothers who smoke.
Placenta accreta is associated with a thin, incompletely developed or absent decidua basalis. In normal uteri, the decidua basalis and its protective membranous barrier (Nitabuch's layer) are thinner and less developed in the lower uterine segment than in the fundal region. Damage to the endometrium and uterine scarring are strongly implicated, as there is an increased association of placenta accreta in surgically scarred uteri. It has been proposed that the decidua basalis deficiency allows chorionic villi to implant directly into the myometrium. Placenta accreta has been described to occur in up to 15% of cases of placenta previa and in 67% of cases where placenta previa occurs in a patient with previous cesarean section for placenta previa. Decidua basalis absence or deficiency has been noted in the histopathologic studies of accreta patients by several authors.4, 17, 28 Another study, confirming the absence of decidua basalis, also noted that trophoblastic tissue was morphologically and immunohistologically normal.29 This supports the concept that the development of accreta is due primarily to a uterine deficiency or damage and not to any abnormalities of the trophoblast itself.
RISK FACTORS
Most of the risk factors that predispose a patient to placenta previa will also predispose them to placenta accreta/increta/percreta. Indeed, the presence of placenta previa is a well-recognized risk factor for placenta accreta.4, 30, 31 The most important risk factors for placenta previa and accreta are age, parity, and a history of uterine surgery. In their definitive 1985 paper, Clark and associates4 noted an 11-fold increase in the incidence of placenta previa among mothers older than 40 years when compared to those younger than 20 years. A more recent long-term epidemiologic study found that for all races there was a five-fold increase in the occurrence of placenta previa for women more than 35 years compared to those less than 20 years of age.6 Other studies have also found an association between age and occurrence of previa.2, 11, 30, 31 Some authors have proposed that age may be a more important determinant than parity.32, 33 Clark and co-workers noted a seven-fold increase in previa among women with a parity greater than five when compared to nulliparous patients, and nearly all papers mention the rising risk of placenta previa with increasing parity.11, 30, 31, 32, 33, 34 One of the most dramatic risk factors for placenta previa or accreta is clearly the presence of previous cesarean section. Although mothers with one previous cesarean had a 2.5-fold increase in the risk of previa, this number multiplied dramatically with increasing number of cesarean sections, peaking at mothers with four or more uterine incisions, who experienced a 38-fold increase in the incidence of placenta previa.4, 31 These results have been confirmed in numerous subsequent studies.3, 6, 10, 11, 35, 36 Additionally, placenta previa has been noted to increase with the number of elective or spontaneous abortions experienced.11, 20, 37, 38 This may be by a similar mechanism to cesarean section. However, because the presence of either induced or elective abortions increases the parity of the patient, the increase in parity may be the more important factor.
Multiple gestations have been commonly mentioned as increasing the risk of previa, because there is a greater amount of placental tissue present in these gestations. However, in one study of 1.8 million Swedish births, the incidence of previa was found to be exactly equal in singleton and twin gestations.39 Another study of 1253 twin mothers found no difference in the frequency of placenta previa between twin and singleton pregnancies, although there was a three-fold increased risk of abruptio placenta among the mothers of twins.40
Smoking has been convincingly linked as a significant risk factor for placenta previa, with a dose-dependent increase of risk.5, 26, 39, 41, 42, 43, 44 Smokers had a relative risk of 2.6–4.4 for placenta previa.26 Placenta previa babies were delivered sooner, at a lower birth weight and with a greater mortality of 14.9/1000 deaths. Cocaine use has shown a mild association with previa,5 and diethylstilbestrol (DES) exposure in utero has been connected with placenta previa as well. Different studies have reported increased risks for previa or accreta among women of Asian origin,9 Thai women, and women of Papua New Guinea.28
Overall, any circumstances that tend to cause uterine damage, myometrial scarring, or deficient development of the decidua may predispose a patient to these placental abnormalities. Other authors have noted conditions not previously mentioned that have been associated with increased risk: myotonic dystrophy, adenomyosis, Asherman's syndrome, congenital uterine malformation, previous cornual pregnancy, histories of curettage, endometritis, hysterotomy, peripartum infection, previous retained placenta, radiation therapy, tubal reimplantation surgery, or presence of uterine fibroids.4, 17, 18, 28, 45, 46, 47, 48, 49, 50, 51 In his exhaustive historical review of 612 accreta cases, Fox18 noted normal uteri and lack of all risk factors in only 1.4% of women with placenta accreta.
CLINICAL PRESENTATION
The classic presentation of placenta previa is painless vaginal hemorrhage in a previously normal pregnancy, which may be an isolated or recurrent event. The initial event usually does not occur until the second trimester.52 Bleeding occurs due to disruption of the placental attachment to the lower uterine segment. In the earliest weeks hemorrhage is usually associated with vaginal examination or intercourse. The amount of bleeding is usually proportional to the degree of placenta previa.52 Patients with a complete placenta previa bleed earlier and heavier than do those with a partial or marginal previa. Clinical presentation of placenta previa can differentiate it from abruptio placentae, another common cause of bleeding in the second half of pregnancy. Bleeding episodes that often cease within 1 or 2 hours; an absence of abdominal discomfort; and a normal fetal heart tracing on electronic monitoring usually characterize placenta previa. On the other hand, abruptio placentae is associated with continuous bleeding; moderate to severe abdominal discomfort; fetal tachycardia followed by bradycardia with loss of variability and decelerations; occasional coagulation defects, including disseminated intravascular coagulation (DIC); and associated history of hypertension or preeclampsia, cocaine use, abdominal trauma, or polyhydramnios. On physical examination the uterus tends to be soft and fetal parts readily palpable. With placenta previa, the presenting part is unengaged and malpresentation is common, seen in up to 50% of cases.52
Most cases of placenta accreta are not discovered until the third stage of labor, when the patient is noted to have an abnormally adherent placenta that requires manual removal or has postpartum hemorrhage secondary to partial placental separation.18
DIAGNOSIS
Historically, the diagnostic confirmation of placenta previa had been through retrospective findings at cesarean delivery53 or on palpation during double set-up examination. However, because of difficulties in defining the exact location of the placental bed during an emergency operation and the obvious implications of the double set-up exam, sonography has become the most accurate and commonly used method for diagnosing placenta previa.53, 54 In fact, most cases are diagnosed incidentally at mid-trimester ultrasound. Before Gottesfeld and co-workers55 first reported on the usefulness of transabdominal sonography for localization of the placenta, angiography, radiography, radioisotope scanning, and digital examination of the placenta were used for diagnosis of the placenta previa.56, 57, 58 Although far from perfect, with false-positive rates of 3–7% and false-negative rates up to 2%, transabdominal sonography is currently the standard in the diagnosis of placenta previa.55, 59, 60, 61 Explanations proposed to account for the false-positive error rate, summarized by Langlois and colleagues,52 include placental conversion, overdistention of the urinary bladder, low-lying myometrial contraction, or leiomyomas and extraembryonic blood clots.
Placental conversion is the main source of the false-positive results of the first and second trimester diagnosis of placenta previa. Various studies have indicated that the incidence of placenta previa in mid-gestation is more frequent than at term.55, 62, 63, 64 The explanation of placental conversion, supported by most authors, is based on the theory that the uterus grows at a faster rate than the placenta as pregnancy progresses. This differential growth rate results in a decrease in the proportion of the inner uterine surface that is covered by placenta. Thus, with time, an initially diagnosed low-lying placenta appears to be carried away from the os toward the fundus.
Overdistention of the maternal urinary bladder is sometimes cited as a cause of false-positive diagnosis of placenta previa.38, 44, 45, 46, 65 Apposition of the anterior and posterior walls of the lower uterine segment may decrease the length of this segment and falsely suggest a placenta previa. Although some authors recommend the routine use of post-voiding scans, other doubt their usefulness, citing the difficulties of visualizing the placenta and its relationship to the os without a full bladder.38
Focal low-lying myometrial contractions may also distort the lower uterine segment and contribute to a previa misdiagnosis. Myometrial contractions can either simulate placental tissue or shorten the distance between the placental edge and the internal os. Townsend and co-workers66 documented myometrial contractions in 16% of the false-positive diagnoses and recommended repeat scanning after 30 minutes if the myometrial thickness exceeds 1.5 cm.31, 47
Morrison48 demonstrated that the lower uterine segment develops continuously throughout pregnancy. Normal lower uterine segment varies from 0.5 cm from the internal os at 20 weeks' gestation to 5 cm at 38 weeks. Therefore, the fixed limitation of the distance between the lower uterine segment and the internal os to within 5 cm for diagnosis of placenta previa will cause several false-positive results early in the third trimester.
Low-lying leiomyomas and extraembryonic blood clots can be easily confused with low-lying placenta and cause false-positive results. Moreover, accurate localization of placenta via the transabdominal route can be difficult in the presence of obesity and posterior or lateral placentation. The acoustic shadow of the fetal head in a vertex presentation may prevent an accurate localization of a low placenta.67
Transabdominal sonography becomes increasingly difficult as the third trimester progresses, predominantly because of attenuation of sound by the presenting part of the fetus.68, 69 Several techniques, including external fetal manipulation, overdistension of the maternal urinary bladder,and Trendelenburg positioning, have been used to elevate the presenting part of the fetus from the pelvis and facilitate visualization of the cervix.68, 69, 70, 71 However, such maneuvers can be uncomfortable for the patient, distort the appearance of the cervix, and are frequently unsuccessful late in the third trimester.69, 70, 71 Because of these limitations, alternative techniques are needed to complement transabdominal sonography for the diagnosis of placenta previa.69 Transvaginal and transperineal sonography are frequently used with transabdominal studies.
There is little doubt that transabdominal sonography will remain as the first-line diagnostic means for the localization of placenta previa.54 However, an emerging body of evidence suggests the superiority of transvaginal sonography in this respect and supports its use as a second-line investigation to avoid the complications of misdiagnosis of placenta previa due to false-positive or false-negative results.
Brown and colleagues first described the use of transvaginal sonography to evaluate the lower uterine segment and cervix during pregnancy in 1986.72 Transvaginal ultrasound not only circumvents many problems faced by transabdominal sonography, but also possesses certain inherent characteristics that improve diagnostic accuracy.54 The sound waves travel a shorter distance from the tip of the vaginal probe to the pelvic organs than they do from the tip of the abdominal probe.54, 67 This enables the use of a higher frequency ultrasound wave generator, which in turn increases picture resolution.54, 67 Transvaginal ultrasonography avoids the disturbances caused by body habitus, bladder overdistention, and acoustic shadowing of fetal parts.54 Tan and co-workers54 demonstrated that transvaginal sonography ruled out placenta previa in 12 cases out of 70 (17%) thought to be placenta previa by transabdominal ultrasound. Leerentveld and colleagues73 reported a positive predictive value of 93.3% and a negative predictive value of 97.6% of transvaginal sonography. Farine and co-workers74 reported a positive predictive value of 71%, but a negative predictive value of 100%.
Despite the higher accuracy of transvaginal sonography, it remains underutilized in the diagnosis of placenta previa.54 This is mainly because of safety concerns. Vaginal manipulation in cases of suspected placenta previa runs against the grain of classic obstetric teaching.54 However, recent data in many studies suggest that sonography is a safe technique. None of the authors encountered any evidence of vaginal bleeding, preterm labor, premature rupture of membranes, or vaginitis.54, 61, 67, 73 Tan and co-workers54 attributed the safety of transvaginal sonography to the fact that the vaginal probe is inserted under direct ultrasonic visualization, and hence direct contact with the cervix is avoided. There is still a fair distance between the tip of the vaginal probe and the cervix when the lower uterine segment comes into focus because the focal range of the vaginal probe is 2–7 cm. Therefore, if the transducer is closer to the target than its focal length, the image may be blurred and out of focus.61
Timor-Tritsch and Yunis61 evaluated the safety of transvaginal ultrasonography in the diagnosis of placenta previa by determining whether the angle between the cervix and the vaginal probe is sufficient for alignment of the probe with the cervix. They concluded that the anatomic relationship between the vagina and cervix, as reflected in the measured angle between the two (greater than 44°), makes inadvertent insertion of the probe into the internal cervical os virtually impossible.
Transvaginal sonographic placental localization appears to be a simple, reliable, and safe technique,73 and it is recommended as a second-line diagnosis in patients who are diagnosed to have minor placenta previa by transabdominal sonography.54 Transperineal sonography is another technique for imaging the cervix during the third trimester of pregnancy, allowing cervical visualization in most patients in whom transabdominal sonography of this area is unsuccessful.69 Although transvaginal ultrasound is more commonly used to complement transabdominal studies, a transperineal approach provides a more convenient means of imaging the cervix and lower uterus without requiring specialized equipment, vaginal penetration, or external fetal manipulation.75 Hertzberg and colleagues75 demonstrated that the greatest value of transperineal sonography was in helping to exclude placenta previa in patients in whom the cervix was not seen on transabdominal sonography. In such cases, transperineal sonography will usually show the internal surface of the cervix without overlying placental tissue, allowing confident exclusion of placenta previa. In a significant minority of patients with placenta previa, however, transperineal sonography will show a placenta previa that was not seen with transabdominal sonography.
The cervix is almost always seen on transperineal sonograms, but the lower edge of the placenta may be beyond the field of view.75 Therefore, transperineal sonography is a valuable procedure to complement transabdominal studies, but not to replace them.
Accurate interpretation of transperineal sonograms requires the same precautions as in the evaluation of transabdominal sonograms,75 and inherent in the procedure are the same sources of false-positive results. The potential value of magnetic resonance imaging (MRI) for placental localization has been investigated in several centers.76, 77 MRI offers two major advantages over ultrasound that may make it particularly suitable for evaluating third trimester bleeding and diagnosis of placenta previa. These advantages are potentially better tissue differentiation and an ability to highlight blood.78 Excellent maternal soft tissue definition can be obtained; both placenta and cervix have a characteristic appearance. Therefore, the relationship of the lower edge of the placenta to the internal cervical os can be accurately determined.
Despite the encouraging research results, MRI diagnosis of placenta previa is still an experimental technique and is not widely used in a clinical setting. Disadvantages associated with MRI for diagnosis of placenta previa include: (1) safety concerns regarding moving a patient from labor and delivery to a radiology suite; (2) the relatively lengthy examination (typically 30–60 minutes); (3) long-term safety in pregnancy has yet to be established; and (4) MRI scans are more costly than ultrasound examination.78 Although there is some evidence for using MRI as a complementary technique to ultrasound, these barriers effectively preclude its use in most patients.
The diagnosis of placenta accreta usually is made at delivery, when it becomes apparent the placenta is abnormally adherent. The diagnosis can be confirmed after surgery with histopathologic examination of the uterus or by biopsy of the placental bed. The characteristic histopathologic feature of this condition is absence or poor development of decidua basalis.79 Diagnosis before delivery would allow adequate surgical preparation to decrease maternal morbidity and mortality. Although it is possible to do so, placenta accreta is rarely diagnosed antenatally.80
The sonographic characteristics of a placenta accreta are the absence of the normal retroplacental clear space, placental tissue contiguous with myometrium, and prominent placental venous lakes and uterine vascularity.79, 80 Absence of the hypoechoic zone is thought to represent a defect in decidua basalis and adjacent myometrium, whereas the vascular changes may be a result of alternative vascular patterns associated with an abnormal basal plate.79, 81
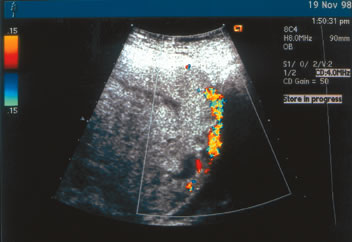
Rosemond and Kepple80 described a case in which abnormal sonographic findings were appreciated only with transvaginal color Doppler sonography. When Doppler flow studies of the normal retroplacental clear space are performed, multiple venous flow signals are seen in this area.80, 82 Absence of this space represents abnormal placentation. In a case of placenta percreta diagnosed at our institution (Fig. 2), the interface between the placenta and the maternal urinary bladder is essentially absent. Transabdominal color Doppler studies were diagnostic in this patient, and placenta percreta was subsequently confirmed at cesarean delivery.
|
Color flow Doppler sonography is also particularly useful in identifying hypervascularity beneath the placental attachment site. This technique highlights the areas of increased vascularity and reveals a continuum of lacunar flow from the placenta through the myometrial layer without an intervening clear space. However, sonographic findings are not pathognomonic for placenta accreta.80 Callen and Filly33 documented absence of a retroplacental clear space in 27 of 100 cases examined prospectively; but none of these patients had placenta accreta.
Antepartum diagnosis of these invasive placental conditions may allow for the placement of arterial catheters preoperatively in case it is necessary to perform uterine artery embolization by interventional radiology, which is designed to lessen the risk of catastrophic hemorrhage. Foreknowledge of placental invasion can also provide the opportunity for additional patient counseling, blood product availability, and an appropriate surgical team to be assembled for the delivery.
TREATMENT
Historically, placenta previa and accreta have been one of the major causes of mortality and morbidity. Often the bleeding may necessitate early delivery, along with its concurrent risks for the premature neonate.83 Prenatal management of placenta previa remains controversial. Although there is a consensus that patients should be confined to bedrest, and that pelvic rest should also be observed, there is no agreement on whether hospitalized bedrest is safer or more effective.84, 85, 86 Most authors agree that patients can be expectantly managed as outpatients until the first bleeding episode. Subsequent management should be individualized to the circumstances, including gestational age, severity of hemorrhage, patient's ability to comply with bedrest, and patient's proximity to the hospital. Various strategies have been tried to prolong pregnancy in the face of nonacute bleeding. Cervical cerclage has been found ineffective in prolonging gestation or decreasing eventual need for blood usage.87 Originally the most common treatment for placenta previa with associated bleeding was the delivery of the infant. With the advent of tocolytic use, it became more common to adopt a conservative management strategy. Tocolytic treatment decreases the amount of uterine contractions, which can also decrease any bleeding. A study by Towers and colleagues found that the use of tocolytics in the management of third trimester bleeding did not increase morbidity or mortality when used in a controlled tertiary setting.88 Similar findings had been reported earlier by other authors.89
In cases of complete placenta previa, if patients remain otherwise stable, documentation of fetal lung maturity and elective cesarean delivery are usually advocated at 35–36 weeks' gestation.60, 89 D'Angelo and Irwin found that most of the severe bleeding episodes they reported in their study occurred after 36 weeks.84 Elective cesarean also allows for use of a regional anesthetic in an otherwise stable patient. In fact, in a retrospective analysis of a 22-year experience, Frederickson noted a significant increase in intraoperative blood loss and the subsequent need for hysterectomy when a general anesthetic was used in cases of placenta previa.90
Management of partial placenta previa is varied. Although double set-up examinations are often mentioned both in reference texts and in the literature, in reality, this is rarely performed in the modern clinical practice. Most practitioners use ultrasound to assess the degree of previa when delivery decisions are being made. There is agreement that when the placental edge is at least 2 cm from the cervical edge, and the fetus is in vertex presentation, it is usually safe to allow the patient a trial of vaginal labor.91 One reason that bleeding is within an acceptable range in these conditions is that the fetal head will act as a tamponade to stop or diminish the bleeding at the placental edge. In most cases, when the placental edge is less than 2 cm from the cervical os, it is considered preferable to proceed with elective cesarean to prevent massive hemorrhage and its complications.
Placenta accreta, increta, and percreta remain among the greatest treatment challenges in modern obstetrics. Massive hemorrhage can easily accompany these conditions. Often patients may exit the operating room in an extremely critical condition, and it is common for disseminated intravascular coagulation (DIC)92 and acute respiratory distress syndrome (ARDS)93 to develop, with a subsequent prolonged intensive care episode.
The most important component of successful management of invasive placental conditions remains preparation. The optimal management will involve the cooperation of members of a multidisciplinary team headed by the obstetrician and including neonatology, anesthesia, blood bank, urology (if bladder involvement is suspected), general surgery, and possibly interventional radiology. It is desirable, if possible, to have uterine artery catheters placed before surgery, because this has been shown in many series to decrease the risk of massive hemorrhage.94 In his 5-year series, Hansch and co-workers had extensive hemorrhage in only of one of six patients. In four patients, bleeding was controlled by uterine artery embolization (UAE), and one patient had prophylactic catheters placed but did not require embolization. In the authors' experience at Evanston Northwestern Healthcare, this approach has been taken in four patients with known placenta percreta, with satisfactory results in three and one patient who did not require use of embolization after preoperative placement of catheters. There are also reports of successful use of argon laser for hemostasis management.93, 95 Paradoxically, after surgery, it is crucial that these women receive thromboprophylaxis, because they are at increased risk of thrombosis due to longer surgical times and the extensive pelvic dissection and manipulation often required.96
COMPLICATIONS
Advances in antenatal surveillance and early diagnosis have led to significant improvements in outcomes associated with placenta previa. Current surgical, anesthetic, and blood component therapeutics have also greatly improved maternal and fetal morbidity and mortality. Nonetheless, placenta previa and placenta accreta continue to present clinical challenges with many associated complications. Hemorrhage remains the major complication of abnormal placentation, often necessitating premature delivery with its own perinatal impact.31 Emergent surgical intervention due to hemorrhage is associated with multiple risks and may require hysterectomy to control blood loss. Although most patients with placenta previa will not require blood transfusion, those who do may have significant blood product requirements. One study of blood bank utilization in placenta previa patients found that 14.6% of patients required transfusion, and 6.3% went on to require hysterectomy.97 Most transfusions were for 1–3 units of packed red cells; however, one patient required 25 units, and another who developed a coagulopathy eventually received 58 units of blood products. In the experience of this institution, we have had similar utilization patterns, where patients require either modest or massive amounts of blood products.
Neonatal complications of placenta previa and accreta are varied. In one study of neonatal outcomes in nearly 93,000 pregnancies, there was a 0.3% rate of placenta previa.83 Among these pregnancies neonatal complications significantly associated with placenta previa were major congenital anomalies, respiratory distress syndrome (secondary to premature delivery), and anemia. The perinatal mortality rate associated with placenta previa was 2.30% versus 0.78% for controls. In addition, the chronic bleeding associated with a placenta previa may be associated with fetal growth restriction, perhaps due to chronic mild hypoxia.
Another complication may be vasa previa, where the placental blood vessels cross the cervical os in advance of the presenting fetal part.98 The major concern is the propensity of these vessels, which lack the protection of either the placental bed or the Wharton's jelly, to become lacerated when the membrane ruptures, with catastrophic results.99 Both of the authors referenced have advocated using Doppler ultrasonography to diagnose vasa previa before delivery, avoiding the potential for laceration or vessel compression and bradycardia. Undiagnosed vasa previa has had a reported mortality of between 33% and 100%.100
Optimal outcomes with vasa previa depend on accurate antenatal diagnosis and cesarean delivery prior to membrane rupture. The impact of antenatal diagnosis of vasa previa was reviewed in a multicenter retrospective study.101 It was determined that, in the absense of prenatal diagnosis, the perinatal mortality was 56%, whereas 97% of babies survived when vasa previa was diagnosed prior to labor. In asymptomatic patients with vasa previa cesarean delivery should be planned for 36–37 weeks. Although amniocentesis is generally recommended for planned delivery prior to 39 completed weeks, the risk of rupture of membranes, fetal exsanguination and death outweighs the relative risks of lung immaturity and respiratory distress syndrome. Therefore, amniocentesis for fetal lung maturity is not generally required prior to delivery in patients with vasa previa. Delivery should take place in an institution where adequate facilities for neonatal resuscitation and blood transfusions are readily available. Finally, the surgical approach should be planned with review of the location of the vessels on ultrasound and avoiding injury to them during cesarean delivery. Figure 3 demonstrates intact membranes at cesarean section with vessels traversing the lower segment and precariously coursing across the interval cervical os. Even under such controlled conditions, careful dissection is necessary to avoid injury to these vessels prior to delivery of the baby.
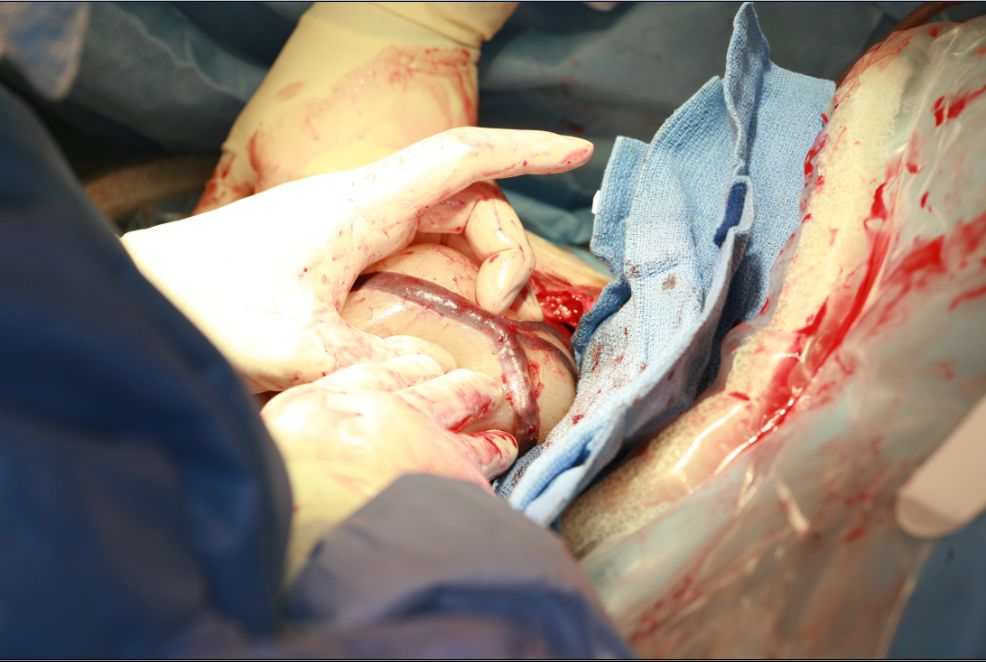 Fig. 3. Intact membranes at cesarean section with vessels traversing the lower segment and precariously coursing across the interval cervical os. (Courtesy of H. Jacob Saleh.)
Fig. 3. Intact membranes at cesarean section with vessels traversing the lower segment and precariously coursing across the interval cervical os. (Courtesy of H. Jacob Saleh.)
CONCLUSION
Placenta previa, placenta accreta, and vasa previal are significant and sometimes catastrophic causes of third trimester bleeding and are today more prevalant causes of maternal and perinatal morbidity and mortality. Leading the list for this increased incidence is the rising rate of cesarean section. Advances in ultrasonography and Doppler imaging have allowed the obstetrician to accurately diagnose these conditions in the antenatal period and better develop treatment strategies with planned delivery in well-equipped facilities.
REFERENCES
Cunningham FG et al: Williams Obstetrics, 18th ed. New York, McGraw Hill, 2001 |
|
Ananth CV, Wilcox AJ, Savitz DA et al: Effect of maternal age and parity on the risk of uteroplacental disorders in pregnancy. Obstet Gynecol 88: 511, 1996 |
|
Chattopadhyay SK, Kharif H, Sherbeeni MM: Placenta praevia and accreta after previous caesarean section. Eur J Obstet Gynecol Reprod Biol 52: 151, 1993 |
|
Clark SL, Koonings PP, Phelan JP: Placenta previa/accreta and prior cesarean section. Obstet Gynecol 66: 89, 1985 |
|
Handler AS, Mason ED, Rosenberg DL et al: The relationship between exposure during pregnancy to cigarette smoking and cocaine use and placenta previa. Am J Obstet Gynecol 170: 884, 1994 |
|
Iyasu S, Saftlas AK, Rowley DL et al: The epidemiology of placenta previa in the United States, 1979-1987. Am J Obstet Gynecol 168: 1424, 1993 |
|
MacGillivray I, Davey D, Isaacs S: Placenta praevia and sex ratio at birth. Br Med J 292: 371, 1986 |
|
Naeye RL: Placenta previa: Predisposing factors and effects on the fetus and surviving infants. Obstet Gynecol 52: 521, 1978 |
|
Taylor VM, Peacock S, Kramer MD et al: Increased risk of placenta previa among women of Asian origin. Obstet Gynecol 86: 805, 1995 |
|
To WW, Leung WC: Placenta previa and previous cesarean section. Int J Gynaecol Obstet 51: 25, 1995 |
|
Zhang J, Savitz DA: Maternal age and placenta previa: A population-based, case-control study. Am J Obstet Gynecol 168: 641, 1993 |
|
Benzineb NF, Battikh O, Sfar R: Placenta accreta, ten cases. J Gynecol Obstet Biol Reprod 24: 751, 1995 |
|
Mahmood TA, Kok KP: A review of placenta accreta at Aberdeen Maternity Hospital, Scotland. Aust N Z J Obstet Gynaecol 30: 108, 1990 |
|
Makhseed M, el-Tomi N, Moussa MA: A retrospective analysis of pathological placental implantation: Site and penetration. Int J Gynaecol Obstet 47: 127, 1994 |
|
Rashbaum WK, Gates EJ, Jones J et al: Placenta accreta encountered during dilation and evacuation in the second trimester. Obstet Gynecol 85: 701, 1995 |
|
Sfar E, Zine S, Chaar N et al: Analysis of placenta accreta risk factors. Rev Fr Gynecol Obstet 89: 202, 1994 |
|
Breen JL, Neubecker R, Gregori CA et al: Placenta accreta, increta, and percreta: A survey of 40 cases. Obstet Gynecol 49: 43, 1977 |
|
Fox H: Placenta accreta, 1945-1969. Obstet Gynecol Surv 27: 475, 1972 |
|
Atrash HK, Koonin LM, Lawson HW et al: Maternal mortality in the United States, 1979-1986. Obstet Gynecol 76: 1055, 1990 |
|
Brenner WE, Edelman DA, Hendricks CH: Characteristics of patients with placenta previa and results of “expectant management.” Am J Obstet Gynecol 132: 180, 1978 |
|
Comeau J, Shaw L, Marcell CC et al: Early placenta previa and delivery outcome. Obstet Gynecol 61: 577, 1983 |
|
Young GB: The peripatetic placenta. Radiology 128: 183, 1978 |
|
Asmussen I: Ultrastructure of the human placenta at term. Acta Obstet Gynecol Scand 56: 119, 1977 |
|
Tominaga T, Page EW: Accommodation of the human placenta to hypoxia. Am J Obstet Gynecol 94: 679, 1966 |
|
Christianson RE: Gross differences observed in the placentas of smokers and nonsmokers. Am J Epidemiol 110: 178, 1979 |
|
Williams MA, Mittendorf R, Lieberman E et al: Cigarette smoking during pregnancy in relation to placenta previa. Am J Obstet Gynecol 165: 28, 1991 |
|
McClung J: Effects of high altitude on human birth. In Observations on Mothers, Placentas, and the Newborn in Two Peruvian Populations, pp 76–139. Cambridge, MA, Harvard University Press, 1969 |
|
Barss A, Misch KA: Endemic placenta accreta in a population of remote villagers in Papua New Guinea. Br J Obstet Gynaecol 97: 167, 1989 |
|
Earl U, Bulmer JN, Briones A: Placenta accreta: An immunohistological study of trophoblast populations. Placenta 8: 273, 1987 |
|
Miller DM, Chollet JA, Goodwin TM: Clinical risk factors for placenta previa—placenta accreta. Am J Obstet Gynecol 177: 210, 1997 |
|
Zaki ZMS, Bahar AM, Ali ME et al: Risk factors and morbidity in patients with placenta previa accreta compared to placenta previa non-accreta. Acta Obstet Gynecol Scand 77: 391, 1998 |
|
Rasmussen S, Albrechtsen S, Dalaker K: Obstetric history and the risk of placenta previa. Acta Obstet Gynecol Scand 79: 502, 2000 |
|
Callen PW, Filly RA: The placental-subplacental complex: A specific indicator of placental position on ultrasound. J Clin Ultrasound 8: 21, 1980 |
|
Williams MA, Mittendorf R: Increasing maternal age as a determinant of placenta previa, more important than increasing parity? J Reprod Med 38: 425, 1993 |
|
Hemminki E, Meriläinen J: Long-term effects of cesarean sections: Ectopic pregnancies and placental problems. Am J Obstet Gynecol 174: 1569, 1996 |
|
Taylor VM, Kramer MD, Vaughan TL et al: Placenta previa and prior cesarean delivery: How strong is the association? Obstet Gynecol 84: 55, 1994 |
|
Barrett JM, Boehm FH, Killam AP: Induced abortion: A risk factor for placenta previa. Am J Obstet Gynecol 141: 769, 1981 |
|
Taylor VM, Kramer MD, Vaughan TL et al: Placenta previa in relation to induced and spontaneous abortion: A population-based study. Obstet Gynecol 82: 88, 1993 |
|
Lilja GM: Placenta previa, maternal smoking and recurrence risk. Acta Obstet Gynecol Scand 74: 341, 1995 |
|
Spellacy WN, Handler A, Ferre CD: A case-control study of 1253 twin pregnancies from a 1982-1987 perinatal database. Obstet Gynecol 75: 168, 1990 |
|
Andres RL: The association of cigarette smoking with placenta previa and abruptio placentae. Semin Perinatol 20: 154, 1996 |
|
Castles A, Adams EK, Melvin CL et al: Effects of smoking during pregnancy: Five meta-analyses. Am J Prev Med 16: 208, 1999 |
|
Ananth CV, Savitz DA, Luther ER: Maternal cigarette smoking as a risk factor for placental abruption, placenta previa, and uterine bleeding in pregnancy. Am J Epidemiol 144: 881, 1996 |
|
Chelmow D, Andrew DE, Baker ER: Maternal cigarette smoking and placenta previa. Obstet Gynecol 87: 703, 1996 |
|
Lauria M, Cotton D: Placenta previa and accreta. In Sciarra JJ (ed): Gynecology & Obstetrics, Vol 2, Chap 49. Philadelphia, Lippincott Williams & Wilkins, 1994 |
|
Morrison JE: Placenta accreta: A clinicopathologic review of 67 cases. Obstet Gynecol Annu 7: 107, 1978 |
|
Finberg HJ: Uterine synechiae in pregnancy: Expanded criteria for recognition and clinical significance in 28 cases. J Ultrasound Med 10: 547, 1991 |
|
Woolcott RJ, Nicholl M, Gibson JS: A case of placenta percreta presenting in the first trimester of pregnancy. Aust N Z J Obstet Gynaecol 27: 258, 1987 |
|
Rivlin ME: Recurrent placenta praevia accreta J Obstet Gynaecol Br 74:938, 1967 |
|
Pridjian G, Rich NE, Montag AG: Pregnancy hemoperitoneum and placenta percreta in a patient with previous pelvic irradiation and ovarian failure. Am J Obstet Gynecol 162: 1205, 1990 |
|
Freeman RM: Placenta accreta and myotonic dystrophy: Two case reports. Br J Obstet Gynaecol 98: 594, 1991 |
|
Langlois SLP, Miller AG: Placenta previa: A review with emphasis on the role of ultrasound. Aust N Z J Obstet Gynaecol 29: 110, 1989 |
|
Taipale P, Hiilesmaa V, Ylostalo P: Diagnosis of placenta previa by transvaginal sonography screening at 12–16 weeks in a nonselected population. Obstet Gynecol 89: 364, 1997 |
|
Tan NH, Abu M, Woo JLS et al: The role of transvaginal sonography in the diagnosis of placenta praevia. Aust N Z J Obstet Gynaecol 35 (1): 42, 1995 |
|
Gottesfeld KR, Thomson HE, Holmes JH et al: Ultrasonic placentography: A new method for placental localization. Am J Obstet Gynecol 96: 538, 1966 |
|
Howell RJS: Haemorrhage from the placental site. Clin Obstet Gynaecol 13: 633, 1986 |
|
Young GB: The peripatetic placenta. Radiology 128: 183, 1978 |
|
Wheeler PC, Stevens EM, Reeves L: A modified method of radioisotopic placenta localization. Am J Obstet Gynecol 93: 961, 1965 |
|
Laing FC: Placenta previa: Avoiding false negative diagnosis. J CLIN ULTRASOUND 9: 109, 1981 |
|
Cotton BD, Read JA, Paul RH et al: The conservative aggressive management of placenta previa. Am J Obstet Gynecol 137: 687, 1980 |
|
Timor-Tritsch IE, Yunis RA: Confirming the safety of transvaginal sonography in patients suspected of placenta previa. Obstet Gynecol 81: 742, 1993 |
|
Varna TR: The implications of low implantation of the placenta detected by ultrasonography in early pregnancy. Acta Obstet Gynecol Scand 60: 265, 1981 |
|
Rizos N, Doran TA, Miskin M et al: Natural history of placenta praevia ascertained by diagnostic ultrasound. Am J Obstet Gynecol 133: 287, 1979 |
|
Laing FC: Ultrasound evaluation of obstetric problems relating to the low uterine segment and cervix. In Sanders RC, James AE (eds): The principles and practice of ultrasonography in obstetrics and gynecology, 3rd ed, p 663. New York, Appleton-Century-Crofts, 1985 |
|
Meyer MB, Joanas BS, Tonascia JA: Perinatal events associated with maternal smoking during pregnancy. Am J Epidemiol 103: 464, 1976 |
|
Townsend RR, Laing FC, Nyborg DA, Jeffrey RB, Wing, VW: Technical factors responsible for 'placental migration': sonographic assessment. Radiology1986; 160: 105-108. |
|
Farine D, Fox HE, Jakobson S et al: Vaginal ultrasound for diagnosis of placenta previa. Am J Obstet Gynecol 159: 566, 1988 |
|
Bowie JD, Andreotti RF, Rosenberg ER: Ultrasonic appearance of the uterine cervix in pregnancy: the vertical cervix. Am J Roentgenol 140: 737, 1983 |
|
Hertzberg BS, Bowie JD, Caroll BA et al: Sonography of the cervix during the third trimester of pregnancy: Value of the transperineal approach. AJR Am J Roentgenol 157: 73, 1991 |
|
Lee TG, Knochel JQ, Melendez MG et al: Fetal evaluation: A new technique for placental localization in the diagnosis of previa. J Clin Ultrasound 9: 467, 1981 |
|
Artis AA, Bowei JD, Rosenberg ER et al: The fallacy of placental migration: Effect of sonographic techniques. AJR Am J Roentgenol 144: 79, 1985 |
|
Brown JE, Thieme GA, Shah DM et al: Transabdominal and transvaginal endosonography: Evaluation of the cervix and lower uterine segment in pregnancy. Am J Obstet Gynecol 155: 721, 1986 |
|
Leerentveld RA, Gilberts EC, Arnold MJ et al: Accuracy and safety of transvaginal sonographic placental localization. Obstet Gynecol 76: 759, 1990 |
|
Farine D, Peisner DB, Timor-Trich IE: Placenta previa: Is the traditional diagnostic approach satisfactory? J Clin Ultrasound 18: 328, 1990 |
|
Hertzberg BS, Bowie JD, Caroll BA et al: Diagnosis of placenta previa during the third trimester: Role of transperineal sonography. AJR Am J Roentgenol 159: 83, 1992 |
|
McGarthy SM, Stark DD, Filly RA et al: Obstetrical magnetic resonance imaging; maternal anatomy. Radiology 154: 421, 1985 |
|
Johnson IR, Symonds EM, Kean DM et al: Imaging the pregnant uterus with nuclear magnetic resonance. Am J Obstet Gynecol 148: 1136, 1984 |
|
Kay HH, Spritzer CE: Preliminary experience with magnetic resonance imaging in patients with third-trimester bleeding. Obstet Gynecol 78: 424, 1991 |
|
Shapiro JL, Sherer DM, Hurley JT et al: Postpartum ultrasonographic findings associated with placenta accreta. Am J Obstet Gynecol 167: 601, 1992 |
|
Rosemond RL, Keppe DM: Transvaginal color Doppler sonography in the prenatal diagnosis of placenta accreta. Obstet Gynecol 80: 508, 1992 |
|
Hoffman-Tretin JC, Koenigsberg M, Rabin A et al: Placenta accreta: Additional sonographic observations. J Ultrasound Med 11: 29, 1992 |
|
Smith DF, Foley WD: Real-time ultrasound and pulsed Doppler evaluation of the retroplacental clear area. J Clin Ultrasound 10: 215, 1982 |
|
Crane JMG, VanDenHof MC, Dodds L et al: Neonatal outcomes with placenta previa. Obstet Gynecol 93: 541, 1999 |
|
D'Angelo LJ, Irwin LF: Conservative management of placenta previa: A cost-benefit analysis. Am J Obstet Gynecol 149: 320, 1984 |
|
Baron F, Hill WC: Placenta previa, placenta abruptio. Clin Obstet Gynecol 41: 527, 1998 |
|
Droste S, Keil K: Expectant management of placenta previa: Cost-benefit analysis of outpatient treatment. Am J Obstet Gynecol 170: 1254, 1994 |
|
Cobo E, Conde-Agudelo A, Delgado J et al: Cervical cerclage: An alternative for the management of placenta previa? Am J Obstet Gynecol 179: 122, 1998 |
|
Towers CV, Pircon RA, Heppard M: Is tocolysis safe in the management of third-trimester bleeding? Am J Obstet Gynecol 180: 1572, 1999 |
|
Watson WJ, Cefalo RC: Magnesium sulfate tocolysis in selected patients with symptomatic placenta previa. Am J Obstet Gynecol 7: 167, 1990 |
|
Fredericksen MC, Glassenberg R, Stika CS: Placenta previa: A 22-year analysis. Am J Obstet Gynecol 180: 1432, 1999 |
|
Oppenheimer LW, Farine D, Ritchie JWK et al: What is a low-lying placenta? Am J Obstet Gynecol 165: 1036, 1991 |
|
Read JA, Cotton DB, Miller FC: Placenta accreta: Changing clinical aspects and outcome. Obstet Gynecol 56: 31, 1980 |
|
Hudon L, Belfort MA, Broome DR: Diagnosis and management of placenta percreta: A review. Obstet Gynecol Surv 53 (8): 509, 1998 |
|
Hansch E, Chitkara U, McAlpine J et al: Pelvic arterial embolization for control of obstetric hemorrhage: A five-year experience. Am J Obstet Gynecol 180: 1454, 1999 |
|
Scarantino SE, Reilly JG, Moretti ML et al: Argon beam coagulation in the management of placenta accreta. Obstet Gynecol 94: 825, 1999 |
|
Arcelus JI, Caprini JA, Motykie GD et al: Matching risk with treatment strategies in deep vein thrombosis management. Blood Coagul Fibrinolysis 10(suppl) 2: S37, 1999 |
|
Wing DA, Paul RH, Millar LK: Usefulness of coagulation studies and blood banking in patients with symptomatic placenta previa. Am J Perinatol 14 (10): 601, 1997 |
|
Chen KH, Konchak P: Use of transvaginal color Doppler ultrasound to predict vasa previa. J Am Osteopath Assoc 98 (2): 116, 1998 |
|
Lee W, Lee VL, Kirk JS et al: Vasa previa: Prenatal diagnosis, natural evolution, and clinical outcome. Obstet Gynecol 95: 572, 2000 |
|
Oyelese KO, Turner M, Lees C et al: Vasa previa: An avoidable obstetric tragedy. Obstet Gynecol Surv 54: 138, 1999 |
|
Oyelese Y, Cantanzarite, V, Prefumo, F, Lashley S, Schachter M, Tovbin, et al. Vasa Previa: the impact of prenatal diagnosis and outcomes. Obstet Gynecol 2004;103:937-42 |