Placental Abruption
Authors
INTRODUCTION
Placental abruption has been defined as the complete or partial separation of a normally located placenta from its uterine site before the delivery of the fetus. This definition differentiates this process from placenta previa, in which the placenta is implanted in an abnormal anatomical position covering the internal cervical os. The condition is also referred to as abruptio placentae, ablatio placentae, and accidental hemorrhage. Classic descriptions emphasize its occurrence in the third trimester of pregnancy, although the process may occur earlier in gestation.
Premature placental separation is suspected clinically when a gravid patient presents with the triad of sudden onset of antepartum vaginal bleeding, a distinctive tender uterus with increased resting tone, and hypertonic or hyperactive uterine contractions. The finding at delivery of adherent clots, hematoma, or hemorrhage to the placenta or membranes, with depression or disruption of the underlying placental tissue, confirms the diagnosis. If the event was recent, the underlying placental tissue may not show this depression.
Placental abruption can display a wide spectrum of severity, varying from the full-blown picture through minor degrees of separation. External bleeding is noted in approximately 80% of patients. When the hemorrhage is concealed, as it may be in 20% of patients, the diagnosis of placental abruption may be delayed,1 although an astute obstetrician will pursue clinical signs and symptoms until a satisfactory diagnosis is reached and the mother and fetus are treated appropriately. Maternal hemodynamic status, coagulation profile, and fetal condition are important clinical parameters in the assessment of severity. Some authors have used various clinical and laboratory parameters to classify patients, as in the following grading system:
Grade I: Mild. This group accounts for 40% of all cases; it includes antepartum hemorrhage of uncertain cause. There may be slight vaginal bleeding and uterine irritability. Maternal blood pressure usually is normal, and there is no maternal coagulopathy or fetal distress. The diagnosis of this class of abruptio placentae is confirmed on postpartum detection of a small retroplacental clot.
Grade II: Intermediate. This accounts for 45% of all cases. This diagnosis is based on the classic features of abruptio placentae with uterine hypertonicity, but the fetus still is alive. There is a greater amount of vaginal bleeding (mild to moderate), hypofibrinogenemia, and fetal distress. Blood pressure is maintained, but the pulse rate may be elevated and postural blood volume deficits may be present.
Grade III: Severe. This accounts for 15% of all cases. In such cases, the fetus is always dead. Usually, heavy vaginal bleeding occurs, although in some cases this may be concealed. Maternal hypotension, hypofibrinogenemia, and thrombocytopenia are present, along with a tetanic uterus. This type is further subdivided into grade IIIA, in which overt coagulopathy is not present, and grade IIIB, when an overt coagulopathy results.2
This grading system may be helpful in establishing a therapeutic plan, but caution should be used because it is important to remember that placental abruption is a dynamic process and maternal–fetal status can change quickly.
EPIDEMIOLOGY
In general, uterine bleeding during the second half of pregnancy is a relatively common complication and occurs in approximately 6% to 8% of all pregnancies.3 Regardless of cause, it is associated with an increased incidence of preterm births and perinatal deaths. Whereas up to 20% of these bleeding episodes have been attributed to placenta previa and 30% to placental abruption,4 at least half are of undetermined etiology. Placental abruption of various degrees occurs in approximately 1% of all pregnancies5 or 1 in 100 births. A recent study has shown that abruption is associated with a perinatal mortality rate of 119 per 1000 births, in comparison to a rate of 8.2 per 1000 births in the reference United States population.6
In the past, placental abruption was most common in older women of lower socioeconomic status, in women who were poorly nourished, and in those with five or more previous pregnancies. A recently recognized cause of abruption is the epidemic abuse of benzoylmethylecgonine, cocaine, an alkaloid prepared from the leaves of the Erythroxyline coca plant.7, 8 A patient with a pregnancy complicated by premature placental separation is at increased risk for recurrence of abruptio placentae in a subsequent pregnancy.
Recently, our group conducted a retrospective cohort study and found that women with preeclampsia, small for gestational age infants, and placental abruption in their first pregnancy (conditions that constitute ischemic placental disease) are at substantially increased risk of recurrence of any or all these conditions in their second pregnancy.9 This epidemiologic evidence supports a common etiologic mechanism present in these conditions, and placental abruption appears to be one of the possible clinical manifestations of ischemic placental disease. The concept of ischemic placental disease will be further discussed later in this chapter.
HISTORICAL DEVELOPMENT
Edward Rigby, an English physician, in a classic essay in 1776, first defined and distinguished between the two main types of third trimester bleeding arising from either low-lying or normal implantation of the placenta.10 The hemorrhage attributed to a low implantation, or placenta previa, in which the placenta must separate for delivery to occur, was labeled “unavoidable,” whereas premature separation of a normally implanted placenta was called “accidental.”
Baudelocque, in 1819, expanded this term to concealed accidental hemorrhage. Unfortunately, because of inadequate elucidation of the clinical symptoms, the concept of such an entity as abruptio placentae was refuted or largely ignored in the years following. It was not until 1861, when Hicks presented 23 cases of concealed hemorrhage before the London Obstetrical Society, that interest in the topic was renewed.
Goodell annotated and described 106 instances of concealed hemorrhage. The documentation of this pathologic picture was continued by others and finally culminated in 1901 with Holmes' extensive survey of the literature, which included 199 new cases. Holmes also introduced the term ablatio placentae. DeLee, who in 1892 described the condition as abruptio placentae because of the rupture of vascular elements, later attended a patient with uncontrollable uterine hemorrhage in association with placental abruption and postulated a hemophilia-like condition.11 Subsequently, similar observations were made by Couvelaire (uteroplacental apoplexy),12 Williams,13 and Wilson,14 who postulated that a toxic material called hemorrhagin released from the placenta or fetus into the maternal circulation caused the clotting defect.
Dieckmann, in 1936, first suggested a causal relationship between low fibrinogen levels and hemorrhage in premature separation of the placenta.15 The efficacy of fibrinogen therapy was reported. The work of Pritchard has been invaluable in elucidating the pathogenesis and treatment of the complications of abruptio placentae.16
INCIDENCE AND TEMPORAL TRENDS
Placental abruption complicates approximately 1% of all singleton pregnancies, and the incidence is at least doubled in twin gestations. A recent, population-based epidemiologic study in the United States comprising 7,465,858 singleton and 193,266 twin births found that abruption was recorded in 0.59% and 1.22% of singleton and twin births, respectively.17 For the incidence of placental abruption, the twin to singleton relative risk was 2.1.
The incidence of abruption has been increasing in the United States and in other western societies. An analysis of the National Hospital Discharge Survey data (1979–1987) indicates that the incidence of abruption increased 28.7% between 1979 and 1980 (8.2/1000 pregnancies) and 1987 (11.5/1000 pregnancies).5 Although the reason for this increase was unknown, the authors conclude that most of the increase occurred among women who were likely to be socially and financially disadvantaged. In a Norwegian population, the authors noted that the frequency of placental abruption increased from 5.3 per 1000 births in 1971 to 9.1 per 1000 births in 1990.18
In 2005, our group used the National Hospital Discharge Summary data (1979-2001) to examine temporal trends in the rate of placental abruption among black and white women in the United States.19 Trends in abruption were assessed for the periods 1979 through 1981 and 1999 through 2001. The rate of abruption increased 92% (95% CI, 88, 96) among black women between 1979–1981 (0.76%; n = 13,584 women) and 1999–2001 (1.43%; n = 18,960 women). Among white women, the rate increased by 15% (95% CI, 14,16) over the same period, from 0.82% (n = 66,186 women) in 1979–1981 to 0.94% (n = 59,284 women) in 1999–2001. This temporal increase in rates of abruption may reflect a true increase in risk, or may be the result of improved diagnosis of both abruption and its determinants.19
Conversely, at some institutions, the frequency of severe abruptio placentae is decreasing.20 Major causes of this have been attributed to the lower parity of reproductive women and the development of improved resources for emergency care at these institutions.21
ETIOLOGY
Despite numerous clinical and epidemiologic studies, the etiology of placental abruption is yet to be precisely determined, but it is thought to be a disease of the decidua and uterine blood vessels. Several conditions continue to be associated with abruption. However in more than 40% of cases, no cause can be identified.22 Chronic factors include maternal vascular disease, chronic and pregnancy-induced hypertension (PIH), cigarette smoking, drug ingestion, nutritional deficiency, uterine anomalies and tumors, supine hypotension syndrome, antiphospholipid syndrome, congenital thrombophilias (including activated protein C resistance, deficiencies of protein C, protein S, and antithrombin III), hyperhomocystinemia, and, rarely, congenital hypofibrinogenemia.
Acute factors include maternal trauma, decompression of the overdistended uterus, and perhaps the acute vascular changes secondary to cocaine abuse. Amniocentesis has been a rare cause of abruption. Other factors such as a short umbilical cord and chorioamnionitis have been associated with abruptio placentae. Placental abruption also has been reported after the insertion of catheter tip intrauterine pressure transducers.23 Evidence and strength of associations linking some of these conditions with abruption are summarized later and in Table 1.
Table 1. Evidence and strength of association linking major risk factors with placental abruption based on published studies
| Evidence | ||
| Risk Factors | Strength | RR or OR |
| Maternal age and parity | + | 1.1–3.7 |
| Cigarette smoking | ++ | 1.4–2.5 |
| Cocaine and drug use | +++ | 5.0–10.0 |
| Multiple gestations | ++ | 1.5–3.0 |
| Chronic hypertension | ++ | 1.8–5.1 |
| Mild and severe preeclampsia | ++ | 0.4–4.5 |
| Chronic hypertension + preeclampsia | +++ | 7.8 |
| Premature rupture of membranes | ++ | 1.8–5.1 |
| Oligohydramnios | + | 2.5–10.0 |
| Chorioamnionitis | ++ | 2.0–2.5 |
| Dietary/nutritional deficiency | +/− | 0.9–2.0 |
| Male fetus | +/− | 0.9–1.3 |
RR, relative risk; OR, odds ratio.
*These estimates are the ranges of RR or OR found in independent studies.
Maternal Age and Parity
Advanced maternal age and multiparity have been associated with an increased risk for placental abruption. However, they often are interrelated, and studies have produced inconsistent results. Although some studies have found women of advanced maternal age (but not parity) to be at an increased risk for abruption,24, 25, 26, 27 others have demonstrated that parity plays an important role in the etiology of placental abruption.28, 29 On the contrary, the U.S. Perinatal Collaborative Project performed from 1959 to 1966 and a population-based study failed to show a relationship between placental abruption and either maternal age or parity.30
In 1996, Ananth and colleagues demonstrated by using population-based cohort data from Nova Scotia, Canada that young, multiparous women (aged 20–24 years and parity of 3 or higher) were at a 3.2-fold increased risk for abruptio placentae compared with nulliparous women aged 25–29 years.31 However, neither maternal age nor parity were independent risk factors for abruption. A larger, population-based retrospective cohort study in the United States found that the risk for abruption among women with singleton gestations was 1.85-fold higher among multigravid (3 or higher) women aged younger than 20 years, relative to primigravid women aged 25–29 years.17 In this same study, the risk for placental abruption among twin births was the highest among multigravid (3 or higher) women aged 35–49 years (relative risk 1.52).17 The implications of an age or parity effect on the increased incidence of abruption are not clear. For instance, whether the increased risk for abruption seen among young, multiparous women reflects a true biologic risk or is a reflection of other confounding factors is not clearly evident.
Maternal Vascular Disease
It has long been recognized that many patients with placental abruption also exhibit chronic hypertension or PIH. Although this is true for abruption overall, it appears that the more severe or higher grades have the strongest association with hypertension.26, 32 Attention has focused on the arterial or afferent segment of the placental circulation to determine if pathologic changes could be attributed to hypertension. Williams previously had described degenerative changes in the intima of the small uterine arteries and postulated a relationship of preexisting toxemia.33 McKelvey's histologic examination of normal placentas at term showed degenerative lesions in the intima of the arterioles of the upper decidua basalis.34 Hertig demonstrated an acute degenerative arteriolitis with subsequent atheroma formation and fibroplastic deposition in the intima of the same vessels.35 He believed that these changes were pathognomonic of toxic separation; they were later deemed to be related to preexisting vascular disease. Subsequent investigation has shown that intimal changes of the spiral arterioles are more severe with hypertensive complications of pregnancy.
Some studies demonstrate an elevated risk of abruption among those with hypertensive diseases, with odds ratios ranging from 1.8 to 4.5,3, 36 whereas others show inconclusive results.29, 37, 38 This discrepancy may be at least partly caused by inconsistent definitions of preeclampsia. In addition, none of the earlier studies separated chronic hypertension and preeclampsia and other types of hypertension to determine the risk for abruption.
We recently set out to evaluate whether the increased risk of placental abruption among women with chronic hypertension is modified by PIH and fetal growth restriction.39 Compared to normotensive women with appropriately grown babies, the risk for abruption was 2.4-fold higher (95% CI, 2.3, 2.5) among women with chronic hypertension as an isolated condition. However, if women experienced either fetal growth restriction and/or PIH, the risks were substantially higher (RR 3.8; 95% CI, 3.6, 4.1) and (RR 7.7; 95% CI, 6.6, 8.9), respectively.39
In summary, vascular disease plays a predisposing role in the disruption of the placental bed in some abruptions. Because hypertension has been shown to cause arteriolar degeneration, the compromised afferent blood supply to the placenta has been emphasized. In addition, superimposed arteriolar spasm would tend to aggravate the ischemia. Perhaps the entire entity may be a progressive stress or accelerated degeneration of an already defective vasculature of the placental bed.
As previously stated, we have introduced the concept of ischemic placental disease, under which we include the 3 clinical conditions of preeclampsia, small for gestational age births, and placental abruption. These conditions share several similarities, as evidenced by uterine and umbilical Doppler studies, placental histology, and biochemical factors. For example, lesions characteristic of placental ischemia (such as hemosiderin deposition, necrosis, and atherosis) are commonly found in placentas of pregnancies complicated by all 3 clinical conditions.9 Numerous studies have also shown that both preeclampsia and SGA, especially at preterm gestational ages, are associated with failure of trophoblast invasion and abnormal Doppler findings in both the uterine and umbilical arteries.40 One potential mechanism for the development of ischemic placental disease is inadequate or aberrant production of factors responsible for angiogenesis at the maternal-fetal interface.40 This aberration can lead to reduced vascular development and/or fetal hypoxia. Examples of such proteins include VEGF (vascular endothelial growth factor), PlGF (placental growth factor), sFlt-1 (soluble fms-like tyrosine kinase-1 receptors), and soluble Endoglin.
With regards to the three conditions of preeclampsia, small for gestational births, and placental abruption, the strengths of the associations with placental histology, abnormal Doppler findings, and biochemical factors is greater at preterm gestations, and also when there is more than one condition present. Therefore, taken together, ischemic placental disease at preterm gestations may be etiologically different from those that occur at term gestations, and this observation is supported by epidemiologic studies, placental histologic data, and Doppler velocimetry findings.40
Trauma
Maternal trauma, whether sustained during an automobile accident, from falls, or from physical abuse, is a significant cause of abruptio placentae. Most reports in the literature stress that abruptio placentae is the major pregnancy complication after blunt abdominal trauma and the leading cause of fetal death after automobile accidents associated with maternal survival.41 Maternal trauma accounts for 1–2% of severe or grade III abruptions. Likewise, abruptio placentae complicates 1–5% of minor injuries and 40% to 50% of major ones (life-threatening).41 Physicians should continue to emphasize the importance of lap and shoulder restraints for their pregnant patients traveling by automobile. Careful consideration of abruptio placentae should be undertaken when the history of an automobile accident or other maternal trauma is noted. The occurrence of abruption may not be able to be predicted based on the severity of abdominal trauma. Abruptions have occurred after seemingly minor maternal injuries. Therefore, all patients sustaining abdominal trauma, especially after a motor vehicle accident, should be monitored closely for signs of clinical abruption and fetomaternal hemorrhage, even if the trauma severity appears mild. A minimal amount of trauma can produce a mild abruption that can progress to severe over the course of 24 hours.42 Certainly, pregnant women involved in high-speed accidents should also be deemed at high risk for abruption regardless of presentation and/or restraint use and must require evaluation. A recent case-control study found that pregnant women involved in severe automobile accidents, i.e., higher speed (>30 mph) or injury severity score, were more likely to have abruptio placentae.41 Because the placenta does not contain elastic tissue, it cannot expand and contract. By contrast, because the uterus contains elastic tissue, it can react to acceleration–deceleration forces by changing its shape. Very high pressures can be generated in the uterus during abrupt deceleration, and high-pressure and marked distortion create a shearing effect on the placental attachment, which results in abruption.43
A complete workup should be performed in suspected cases, including a sufficient period of maternal and fetal observation, along with fetal heart rate monitoring. Recommendations include continuous monitoring for at least 24 hours, and even up to 48 hours, because of possible delayed abruption (seen up to 5 days after trauma).44 Those who should receive at least 24 hours of continuous fetal heart rate monitoring include patients with six or more contractions per hour, abdominal or uterine tenderness, vaginal bleeding, evidence of hypovolemia, or those with nonreassuring fetal heart rate patterns.45 In the absence of uterine activity along with a reassuring fetal heart rate tracing, the duration of monitoring may be less. In a pregnant trauma patient, the admission white blood cell count (WBC) may also be useful in assessment for placental abruption.46 The white count (WBC × 103/mm3) has been found to be significantly elevated in patients with abruption versus those without (27 ± 4.6 vs. 17 ± 7.8; p = 0.005), along with the band count (10 ± 6.6% vs. 4 ± 6.1%; p = 0.03). Therefore, a WBC more than 20,000/mm3 on admission should raise one's suspicion of the possibility of abruptio placentae. Conversely, a WBC of 20,000/mm3 or less may be associated with a very small, if any, risk for abruption, because the negative predictive value is 100%.46
Other traumatic etiologies of abruption include separation of the placenta in a twin gestation after delivery of the first twin with subsequent decompression, attempted external cephalic version, and drainage of amniotic fluid associated with polyhydramnios (in rare cases after amniocentesis for maturity studies). In the case of polyhydramnios, the abruption can occur both from the needle insertion and from the loss of fluid and uterine decompression. Rapid decompression should be avoided. A short umbilical cord (<20 cm) may be a factor in some abruptions. Excessive fetal traction on the placenta either before or during labor also can result in premature separation.
Supine Hypotensive Syndrome
Approximately 10% of pregnant women at term display a significant decrease in blood pressure in the supine position.1 This decreased peripheral pressure is presumed to be secondary to compression of the aorta and vena cava by the gravid uterus and to blockage of the uterine veins at the pelvic sidewalls. Supine hypotension generally is relieved by placing the patient in the lateral decubitus position. Isolated case reports suggest a relationship between placental abruption and the supine hypotensive syndrome. However, the absence of a higher incidence of abruption in patients with large infants or multiple gestations makes it unlikely that supine hypotension is of major clinical significance.
Cigarette Smoking, Dietary Deficiency, and Drug Use
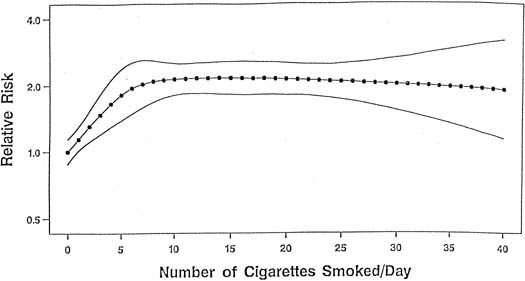
Although the mechanism linking tobacco smoke to the development of placental abruption still is unclear, several studies have found smoking to be a risk factor for abruption, whereas other studies show that the strength and magnitude of association between smoking and placental abruption were inconsistent. A recent meta-analysis, however, on the association between smoking during pregnancy and abruption, based on 1,385,352 pregnancies, indicates that smoking was associated with a 90% increase in the odds of developing abruption.47 This yielded a population attributable risk of 20%, indicating that 20% of abruption cases are potentially preventable if women quit smoking. These authors found a dose–response relationship between the average number of cigarettes smoked per day and the abruption risk. The relative risk increased in proportion to the increasing number of cigarettes smoked per day (Fig. 1). At 10 or more cigarettes per day, the relative risk remained fairly constant at 2.1, which suggests a possible “saturation” effect at 10 cigarettes.
|
Several potential mechanisms relating smoking to the development of placental abruption have been proposed. Based on pathologic examination, Spira and colleagues suggest that smoking leads to chronic hypoxia, which in turn produces placental enlargement, increasing the risk for placental abruption.48 Christianson also found placentas of smokers to be enlarged and to have lesions characteristic of underperfusion of the uterus.49 Others speculate that smoking may cause endothelial changes, which subsequently lead to vasoconstriction and rigidity of the arteriolar walls, resulting in placental underperfusion. This, in turn, may lead to ischemia of the decidua basalis, with eventual decidual necrosis and hemorrhage.50
A recent study also examined the relationship between smoking and preeclampsia and between smoking and preeclampsia superimposed on chronic hypertension.3 When compared with nonsmoking normotensive women, smokers with severe preeclampsia were at 5.9-times greater risk for abruption. Among smokers with preeclampsia superimposed on chronic hypertension, the relative risk for abruption was 7.8.
Other authors attribute an increased frequency of placental abruption to anemia or deficiencies of folic acid, vitamin A, or calcium.28 These deficiencies probably reflect the overall poor nutrition in women of a lower socioeconomic group, who are more prone to this complication. In addition, folate deficiency is related to hyperhomocystinemia, which itself has been found in women with placental abruption (see section on hyperhomocystinemia later).
During the 1980s, cocaine abuse reached epidemic proportions among Americans and still is widespread. Many case reports of pregnant women using cocaine, having transient episodes of hypertension, and subsequent placental abruptions with its associated complications, have been reported in the literature.51, 52 Fetal deaths secondary to placental abruption have been reported in women abusing cocaine during pregnancy.53 A recent meta-analysis also confirms that cocaine use during pregnancy causes abruption,54 and another study involving more than 17,000 women found that the association existed even after adjustment for several confounding factors.55
Cocaine is an alkaloid prepared from the leaves of the coca plant.7, 8 It can be administered intranasally;56 injected subcutaneously, intramuscularly, or intravenously; or administered orally, vaginally, sublingually, or rectally.57, 58 In particular, a form of cocaine freebase called “rock” or “crack,” because of the popping sound made when the user heats it,59, 60 has become extremely popular. Cocaine acts by blocking the presynaptic reuptake of the neurotransmitters norepinephrine and dopamine. Therefore, there is an excess of transmitter at the postsynaptic receptor sites,61 resulting in activation of the sympathic nervous system and producing vasoconstriction, tachycardia, an abrupt increase in blood pressure, and a predisposition to ventricular arrhythmia and seizures.61 Placental vasoconstriction also occurs,62 decreasing blood flow to the uteroplacental–fetal unit.63 The hypertension and vasoconstriction probably are responsible for the placental abruptions that are encountered in women soon after the intake of cocaine.63 It should be noted that cocaine abuse may be an etiologic factor in large and unusually early abruptions.52
Congenital Hypofibrinogenemia and Dysfibrinogenemia
Several case reports linking congenital hypofibrinogenemia and recurrent placental abruption appear in the obstetric literature. Ness and coworkers describe a patient who had a history of recurrent abruptio placentae and subsequently was found to have congenital hypofibrinogenemia.64 The patient had no bleeding problems in the nonpregnant state. Other members of the patient's family also displayed decreased fibrinogen levels. Pritchard has theorized that the hypercoagulable, hyperfibrinogenemic state of the normal pregnancy plays a role in maintaining placental attachment and controlling small placental separations and hemorrhage that often occur.32
A recent study has also described a patient having placental abruption in whom dysfibrinogenemia was subsequently diagnosed.65 It was discovered that her father and brother also had dysfibrinogenemia found through coagulation studies. This is an autosomal-dominant disorder that is caused by genetic mutations that create dysfunctional fibrinogen resistant to thrombin cleaving. These patients have greater risks for obstetric complications, such as spontaneous abortion and postpartum thrombosis, when compared with the general population.65
Hyperhomocystinemia and Other Congenital Thrombophilias
Homocysteine remethylation to the essential amino acid methionine depends on folate and vitamin B12. Enzyme deficiencies involved in homocysteine remethylation and folate and vitamin B12 metabolism, as well as malnutrition and malabsorption of these vitamins, may result in hyperhomocysteinemia.66 One enzyme involved in the remethylation of homocysteine to methionine is methylenetetrahydrofolate reductase (MTHFR), of which there are several documented mutations in this gene (C677T and A1298C). Hyperhomocystinemia induces endothelial cell injury and dysfunction and leads to premature arteriosclerosis and thromboembolism.67 Elevated homocysteine levels have also been shown to damage the vascular endothelium and result in placental vasculopathy.68 The relation between mild hyperhomocystinemia and complications in pregnancy leading to placental abruption has been demonstrated by several studies.69, 70, 71 One study found that of 84 women with a history of placental abruption or infarction, hyperhomocystinemia was found in 31%,69 whereas another study showed a 26% incidence.70 Owen and associates found hyperhomocystinemia in 29% of women with unexplained abruptio placentae.72 Interestingly, a recent study found that combined heterozygosity for MTHFR mutations C677T and A1298C was detected in 22.2% of their population of abruption cases.68 They suggest that combined heterozygosity for these two MTHFR mutations may represent a genetic marker for abruption. These authors also found that the A1298C mutation occurred significantly more frequently in mothers with abruptio placentae as compared with the control cohort. In addition, the combination of hyperhomocystinemia and thrombotic factors like activated protein C resistance, protein C, protein S, antithrombin, and factor V Leiden increases the risk for placental abruption three to seven times.73
Hyperhomocystinemia can be treated with a combination of folic acid and vitamin B6 (pyridoxine). Folic acid enhances remethylation of homocysteine to methionine and vitamin B6 is a cofactor for cystathionine-beta synthase activity, which converts homocysteine to cystathionine.70 It is not known whether normalization of hyperhomocystinemia by periconceptional folate administration favors pregnancy outcome in women with placental abruption or infarction.69 There seems to be no evidence of adverse effects of high folic acid levels or vitamin B6 levels on mothers during pregnancy that are caused by the supplementation dosages.
Other maternal congenital thrombophilias have been found in patients with abruptio placentae, such as protein S and protein C deficiencies,70 along with antithrombin III deficiency. Also, resistance to activated protein C from factor V Leiden mutation has been found frequently (25%–30%) in patients with placental abruption,74, 75 and the authors suggest that the occurrence of abruption should lead clinicians to seek this diagnosis.74 In 2007, a retrospective, case-control study conducted in the Czech Republic found that the heterozygous form of factor V Leiden was present in 20 of 142 cases (14.1%) in the placental abruption group, compared to 10 of 196 (5.1%) in the control group (odds ratio 3.0, 95% CI 1.4-6.7).76 Therefore, the authors concluded that factor V Leiden was a significant risk factor for placental abruption.
Pregnant patients with antiphospholipid antibody syndrome, which involves two antibodies (lupus anticoagulant and anticardiolipin antibody) that are believed to cause thrombosis, may experience not only recurrent pregnancy loss, preeclampsia, and intrauterine growth restriction but also placental abruption.77 In patients with placental abruption, deVries and coworkers report a 13% prevalence of anticardiolipin antibodies (versus 4% in the general population).70 A recent study has found that compared with a control group, the prothrombin gene mutation was significantly more prevalent (18.5%) in women with abruption (odds ratio of 5.8).78
Association With Prolonged Preterm Premature Rupture of the Membranes
Premature rupture of the membranes (PROM) is a common obstetric complication, occurring in approximately 10% to 15% of pregnancies.79, 80 Previous studies suggest that women with prolonged preterm PROM are at an increased risk for having placental abruption.81, 82, 83, 84 Nelson found a three-fold to eight-fold increased risk for abruption in patients who were followed-up expectantly after prolonged preterm PROM. In their case reports, patients had significantly decreased amniotic fluid.85 Vintzileos and associates retrospectively studied 298 patients with prolonged PROM and noted those with severe oligohydramnios (<1 cm) to be at particular risk for abruptio placentae.84
Results of a meta-analysis based on pooled data from four studies indicate that PROM is associated with a three-fold increased risk for abruption.86 The meta-analysis, however, revealed widespread disagreement among study results. Methodologic inconsistencies among these studies in the definition of both preterm PROM and placental abruption may have contributed to this disagreement. For instance, two studies defined preterm PROM as ruptured membranes not followed by the initiation of labor or delivery within 24 hours and that resulted in preterm delivery (<37 weeks of gestation).82, 84 In other studies, however, the definition of preterm PROM was not reported. The clear lack of consensus with preterm PROM on the definition of minimum latency time (between membrane rupture and the onset of labor) makes comparison of study results difficult.
In a retrospective cohort study derived from the 1988 National Maternal and Infant Health Survey, it was found that the risk of abruption was 3.58-fold higher (95% CI 1.74–7.39) among women with preterm PROM (2.29%) compared with women with intact membranes (0.86%).87 The risk was higher either in the presence of intrauterine infections or oligohydramnios.
There appear to be several plausible biologic mechanisms that may be responsible for the increased risk for placental abruption in relation to preterm PROM. Vintzileos and colleagues conclude that infections do not seem to be implicated in the mechanism by which preterm PROM predisposes to the development of abruptio placentae.80 This finding was supported by our recent data, because we observed preterm PROM and intrauterine infections to be independent risk factors for abruption.87 Nelson and associates speculated that an acute reduction in the uterine volume and intrauterine surface area as a consequence of preterm PROM could ultimately lead to a disruption in the site of placental attachment, thereby resulting in abruption.85
Association With Elevated MSAFP (Maternal Serum Alpha-Fetoprotein) Levels
A relationship has been found between unexplained elevated MSAFP levels in the second trimester and pregnancy complications such as placental abruption.88 One group found that in such women presenting with preterm labor, there was an increased relative risk for abruption.89 Bartha and associates measured MSAFP at the time of admission in women presenting with preterm labor and intact membranes.90 They found elevated levels of MSAFP in two thirds of patients subsequently found to have placental abruption.
Association with first-birth Cesarean section
Two recent population-based retrospective cohort studies have found that women who have a cesarean first birth have an increased risk of placental abruption in a second pregnancy, when compared with women who had a vaginal first birth.91, 92
Other Etiologic Factors
Other possible associations that have been noted in the literature include abruptio placentae after snake bite,93 nipple stimulation,94 and prostaglandin E2 use.95 Uterine fibroids, especially when located behind the implantation site of the placenta, also may predispose to abruption.
RECURRENCE
A pregnant woman with previous abruptio placentae should be monitored with caution. The recognition of a strong recurrence risk for abruption in subsequent pregnancies was recently quantified in a meta-analysis.86 The incidence of recurrent abruption was increased by approximately 20-fold to 30-fold in subsequent pregnancies when an earlier pregnancy was complicated by placental abruption (Table 2). The relative risk was less than 9.0 in only two of the 11 studies examined. Unfortunately, the management of such patients remains difficult because there is no good prospective way to predict if and when an abruption might occur.
Table 2. Placental abruption in the first and subsequent pregnancies and relative risk of recurrent abruption
| Risk (%) | Relative | ||
| Authors | Preg 1 | Preg 2+* | Risk† |
| Abdella | 1.17 | 5.8 | 5 |
| Hibbard & Jefcoate | 1.16 | 17.3 | 15 |
| Hibbard & Hibbard | 1.07 | 17.8 | 17 |
| Paintin | 0.73 | 6.5 | 9 |
| Rasmussen | 0.64 | 4.4 | 7 |
| Paterson & Mills | 0.55 | 15.6 | 28 |
| Porter | 0.52 | 12.8 | 25 |
| Karegard | 0.44 | 4.5 | 10 |
| Yla-Outinen | 0.21 | 3.1 | 15 |
| Pritchard | 0.20 | 11.0 | 55 |
| Pritchard et al. 1991 | 0.12 | 12.0 | 100 |
Preg, pregnancy.
*Incidence of abruption in pregnancies 2+ was estimated as the proportion of pregnancies 2+ that were complicated by abruption, given that the first pregnancy was complicated by abruption.
†Relative risk is the ratio of the incidence of abruption in pregnancies 2+ to the incidence in pregnancy 1.
Adapted from Ananth CV, Savitz DA, Williams MA et al: Placental abruption: A meta-analysis of its incidence, and its association with hypertension and prolonged rupture of membranes. Obstet Gynecol 88:309, 1996.
The etiology and risk factors that are associated with recurrent abruptions are unknown. Using data from the Collaborative Perinatal Project (1959–1966), Misra and Ananth examined the incidence of placental abruption in the first pregnancy only (n = 10,774) and in first and second pregnancies (n = 6,529) during the original study period.96 Placental abruption occurred in 1.7% (n = 182) of first pregnancies and in 2.2% (n = 143) of first and second pregnancies. Previous abruptions increased the risk for subsequent abruptions significantly, with an odds ratio of 3.2. Causes of abruption for the first and second pregnancies were different. The number of cigarettes smoked per day during pregnancy, preeclampsia, and weight gain were strong risk factors in the first pregnancy, whereas placental infarcts and smoking duration were associated with an increased risk for abruption in the second, but not first, pregnancies. These results indicate that risk factor profiles of abruption in first and second pregnancies may be different, implying heterogeneous etiologies.
A high risk of recurrence should be expected in all women with antiphospholipid syndrome and congenital thrombophilias. These women should be treated with aspirin and heparin, but such treatment does not guarantee that placental abruption will not occur in future pregnancies.
Recently, our group conducted a retrospective cohort study and found that women with preeclampsia, small for gestational infants, and placental abruption in their first pregnancy (conditions that constitute ischemic placental disease) are at substantially increased risk of recurrence of any or all these conditions in their second pregnancy.9 This epidemiologic evidence supports a common etiologic mechanism present in these conditions, and placental abruption appears to be one of the possible clinical manifestations of ischemic placental disease.
PATHOLOGY
Gross Findings
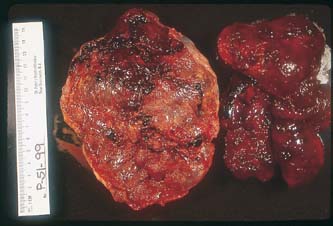
The hallmark of the clinical diagnosis of placental abruption is the presence of a retroplacental or any adherent clots, hematoma, or hemorrhage of variable size to the placenta or membranes with or without depression, disruption, or compression of the maternal placental surface (Figs. 2 and 3). The clots usually are dark, firm, and adherent, in contrast to the red, soft, nonadherent clots formed during physiologic placental separation in the third stage of labor. Occasionally, when the pathologic process is rapid and leads to total placental separation, the depressed area and the clots just described may not be seen.
|
|

Microscopic Findings
Microscopic examination of the placenta, and the uterus if it has been removed, shows variable structural changes in the decidua basalis, uterine muscularis, chorionic plate, and intervillous architecture. In normal pregnancies, uterine spiral arteries will undergo transformation from muscular arterioles to low-resistance, dilated vessels.88 Such changes occur as a result of trophoblastic invasion during the first (10–16 weeks) and second (16–20 weeks) trimesters.88 In patients with placental abruption, however, pathologic changes in the placental bed show a high incidence of vascular abnormalities. The most common finding (60%) is absence of physiologic transformation of uteroplacental arteries.97 This results in decreased placental blood flow and dysfunctional endothelial responses to vasoactive substances. These abnormal placental vessels may predispose to ischemia and rupture of involved vessels, thus causing placental abruption.98 One or more signs of vasculopathy can be seen, such as atherosis, narrowing, necrosis, and thrombosis, as in patients with vascular disease.73 Anomalies in vessels deep in the myometrium, including vessel occlusion with surrounding myometrial hemorrhage, are seen in 33% of the cases.97 Decidual hematomas, thrombosis of the vessels, and focal necrosis are common, together with recent infarcts. These may be extensive enough to involve large areas of the chorionic plate. Congestion of the capillaries of the chorionic villi often is present. Placental abruption often develops simultaneously with placental infarction, which also markedly increases the risk for fetal or neonatal death. Placental infarcts are predominantly caused by spiral artery occlusion in the myometrium or decidua.69 Organized (older) infarcts and hemosiderin granules in the decidua and chorion are seen in cases of chronic abruption. One study, which examined placentas histologically, suggests that the acute clinical catastrophe of abruptio placentae is a long-term process frequently preceded by intrauterine bleeding and hemosiderin deposition.98 The authors found hemosiderin deposition in the placenta to be significantly more common in preterm births than in term deliveries.
In instances of severe premature separation of the placenta, widespread hemorrhages are seen throughout the uterine muscularis and serosa, with blood dissecting into the broad ligaments and under the pelvic peritoneum. This classic picture was first described by Couvelaire as uteroplacental apoplexy.12 An underlying hemorrhagic diathesis usually was involved. Grossly, there even may be fissures on the serosal surface of the uterus, with evidence of active bleeding and hemoperitoneum. Blood effusions also can occasionally be seen beneath the tubal serosa and in the substance of the ovaries, presumably from uterine bleeding through the tubes or across the serosa.20 Extravasation of blood imparts a dark violaceous hue to the uterine serosa and broad ligaments. Microscopic examination confirms diffuse infiltration of blood and widespread edema in the muscularis, with disruption of muscle bundles and smaller blood vessels. Multiple thrombi are found in the smaller veins. Extravasation of blood is most severe in the region of prior placental attachments. In addition to uterine bleeding, focal hemorrhages sometimes occur in the ovaries, kidneys, adrenals, liver, gastrointestinal tract, heart, and central nervous system.
Thompson and coworkers studied the renal lesions of PIH and abruptio placentae by biopsy and found similar glomerular lesions in both kidneys.99 These include swelling and slight proliferation of endothelial cells, an increase in mesangial cells and matrix, and granular deposits derived from fibrinogen within the endothelial cells and the mesangial matrix. They further suggest that in abruptio placentae and PIH, thromboplastin is released from the placental site and causes disseminated intravascular coagulation (DIC). This process is further complicated because of the impairment of the fibrinolytic mechanisms in pregnancy.
Some authors have found a correlation between abruptio placentae and chorioamnionitis. A case-control study found the incidence of histologic chorioamnionitis to be higher in cases of abruption (30%) versus the control group (22.9%), but the difference was not statistically significant.22 Another group found a high incidence of silent histologic chorioamnionitis in cases of preterm abruption (41%) compared with controls (4%).100 They also demonstrated that chorioamnionitis is seven-times more likely to occur in patients with abruption than in the control group.100 Evidence of histological, not clinical, chorioamnionitis was also found to be increased in patients with placental abruptions in yet another study.101
Recently, our group set out to determine whether abruption was associated with an increased incidence of histologic chorioamnionitis among singleton gestations.102 In preterm gestations, chorioamnionitis was present in 31% and 13% of abruption cases and controls, respectively (OR 3.6, 95% CI 1.7, 10.5). In term gestations, the corresponding rates were 35% and 20%, respectively (OR 2.8, 95% CI 1.3, 6.1). We also found that severe chorioamnionitis was 7.2 (95% CI 1.6, 20.1) and 18.3 (95% CI 2.2, 150.4) times more common in abruption patients at preterm and term gestations, respectively.102 These observations suggest that the histologic findings in abruption are accompanied by severe inflammation, in both preterm and term gestations.
PATHOPHYSIOLOGY
The magnitude of the placental surface that becomes separated from the maternal blood supply determines the clinical picture by affecting the amount of acute blood loss from the mother and the decrease in oxygen supply to the fetus, leading to fetal distress or possible death. Patients with a small placental detachment may be asymptomatic.
Although the cause is unknown, premature separation of the placenta and the intramyometrial hemorrhage probably results from rupture of an uteroplacental artery with extravasation of blood under arterial pressure between myometrial bundles. Blood tracking to the decidua basalis results in placental separation and resultant fetal hypoxia, whereas hemorrhage toward the serosal surface of the uterus produces the typical ecchymosis of the Couvelaire uterus.97 The initial event presumably is hemorrhage into the decidua basalis, most commonly from damaged or ruptured small maternal decidual arteries, with the formation of a hematoma. The decidua separates because of localized anoxic necrosis and pressure resulting from bleeding into a confined space; it splits along natural planes in a fashion similar to that occurring normally in the third stage of labor. As the hematoma expands, disruption and separation of the basal plate from the decidua increases until complete placental detachment results. Compression from the hematoma obliterates the overlying intervillous space. Further damage of placental vessels adds to the insult, and the process can be self-perpetuating. It is this expanding force that in some cases accounts for the infusion of decidual debris, rich in thromboplastin, into the maternal venous lakes and systemic circulation. This process accounts for the phenomenon of DIC and its accompanying complications. Ultimately, destruction of placental tissue in the involved area occurs.
The hematoma that results may remain localized and may not extend to a point at which it becomes manifest clinically. Subsequent organization of this concealed area of infarction may be identified as a white placental infarct at the time of delivery. Ramsey has shown that the arterioles and veins that supply and drain the intervillous space travel the same pathways.103 This is consistent with the fact that intradecidual and intervillous hemorrhages frequently remain localized. By contrast, the process may be so fulminating that brisk hemorrhage occurs, with complete detachment of the placenta and evidence of progressive uterine enlargement resulting from the accumulation of blood.
In most patients, the bleeding from placental separation extends to the edge of the placenta, at which point it may either break through the amniotic membranes and enter the amniotic fluid or, more frequently, continue to dissect between the chorion and decidua vera until it reaches the internal cervical os and vagina. Provided that no blockage exists (e.g., densely adherent membranes, cervical stenosis, a tightly fixed fetal head, a firm blood clot, or placenta previa), the blood exits from the vagina as revealed hemorrhage. The lower the insertion of the placenta on the uterine wall, the more likely that external hemorrhage will appear early in the process. The color of the blood varies from bright red to dark brown. Depending on the time elapsed since initiation of bleeding and the distance of implantation of the placenta from the cervical os, the hemorrhage may remain concealed and completely retained inside the uterus. This is more likely to occur when placental margins remain adherent to the uterine wall, blood gains access to and remains within the intra-amniotic cavity, and the fetal head remains closely applied to the lower uterine segment so that blood cannot escape around it. If the concealed hemorrhage dissects through the amniotic membranes to discolor the amniotic fluid, it often produces the classic “port wine” discoloration that is almost pathognomonic of abruption. Most patients with abruptio placentae, however, have “mixed” bleeding, containing elements of external and internal hemorrhage. It is important to remember that the amount of vaginal bleeding often is only a small portion of the total lost from the circulation and is not necessarily a reliable indicator of the severity of the condition. The uterine musculature may be irritated by a developing retroplacental hematoma, and this causes contractions that also may direct blood externally. Sometimes, the presence of grossly bloody and blood-tinged amniotic fluid may be the first clue that placental separation has taken place.
Concept of Ischemic Placental Disease
Our group has recently reported on the type and frequency of the maternal and fetal conditions leading to indicated preterm birth.104 The most frequent conditions were preeclampsia, small for gestational age, and placental abruption. We found that 53% of the indicated preterm births (< 35 weeks) had one or more of these three conditions present. Because these conditions share several similarities (as evidenced by uterine and umbilical Doppler studies, placental histology, and biochemical placental factors), we have introduced the term "ischemic placental disease," under which we include these 3 clinical conditions. It may be that these conditions may be different clinical manifestations of a common etiology (defective/inadequate placentation). The pathophysiology of ischemic placental disease involves impaired trophoblastic invasion of maternal spiral arteries, followed by placental hypoxia, release of thrombin/inflammatory factors, and then endothelial cell activation and damage. It is important to note that ischemic placental disease at preterm gestations is etiologically different from those that occur at term gestations.40 Accordingly, preterm placental abruption may have the same pathophysiology as that just described for ischemic placental disease. Therefore, placental abruption appears to be one of the possible clinical manifestations of ischemic placental disease.
Placental Abruption as A Chronic Process
It is widely believed that placental abruption is an acute event. However, it may be the end-result of a chronic process. Our group recently found that any episode of vaginal bleeding at <20 weeks gestation conferred an increased risk of placental abruption (adjusted RR 1.6, 95% CI 1.3, 1.8).105 The greatest risk occurred with bleeding in both the first two trimesters (RR 3.1, 95% CI 2.3, 4.1). We also found that the presence of chronic lesions in the placenta, decidua, membranes, or umbilical cord was generally associated with an increased relative risk of abruption. Due to the observation that placental inflammatory lesions carries an increased risk of abruption, this suggests that the pathophysiologic and etiologic basis for abruption lies in more of a chronic inflammatory process (rather than an acute event), which may be the final manifestation of the chronic process.105
DIAGNOSIS
Placental abruption accounts for approximately one third of all cases of antepartum hemorrhage. In most patients, the diagnosis is made either during the third trimester or during labor. The classic, clinical hallmark is vaginal bleeding, which may be present in up to 80% to 90% of cases. Concealed hemorrhage may occur in 10% to 20% of cases.106 The differential diagnosis in patients presenting with antepartum bleeding includes placenta previa, premature labor, genital tract trauma, carcinoma of the cervix or vagina, coagulation defects, and hemorrhagic cystitis. Patients with placental abruption most commonly present with the triad of abdominal pain, abnormal uterine tenderness, and vaginal bleeding after the 20th week of pregnancy. However, abdominal pain may be present in up to only 50% of cases and is probably caused by hypertonic contractions or extravasation of blood into the myometrium. A recent study examining 198 women with placental abruption found that the most common manifestations were: vaginal bleeding (70%), abdominal pain (51%), bloody amniotic fluid (50%), and fetal heart rate abnormalities (69%).107 An important fact was also that in 19% of cases, neither bleeding nor pain was present. Therefore, it is important to remember that these signs are not always present, and absence of such symptoms does not exclude the diagnosis. Most cases of severe hemorrhage usually occur before labor and have a concealed component. Milder cases tend to occur during labor, with intermittent episodes of vaginal bleeding.
The presence or absence of any of the previously mentioned symptoms and the degree of severity are directly proportional to the magnitude of the placental separation. The initial symptom may be a sudden, sharp, severe pain that persists or evolves into a poorly localized dull ache in the lower abdominal or sacral areas. It may disappear entirely or be followed by intermittent cramp-like pain corresponding clinically to uterine contractions. It has been reported that abruptio placentae is associated with preterm labor in more than 60% of cases.22 The uterus often does not relax completely between contractions, but in a few severe cases, it may become flaccid. The occurrence of high-frequency low-amplitude contractions and an increased baseline uterine tone often is seen in those with placental abruption. Patients often report nausea, vomiting, or dizziness. Except for mild cramping, some patients may remain asymptomatic. Remember that abruptio placentae also may present as preterm labor that appears to be idiopathic;108 as many as 10% of idiopathic preterm labor cases may be caused by concealed abruptio placentae.
In severe cases, the entire uterus develops a board-like rigidity, so that palpation of fetal parts and auscultation of fetal heart sounds are difficult. In less severe cases, the area of uterine tenderness and spasm varies and may be absent or confined to a limited area that often corresponds to the placental location. Clinically, this finding is dramatic, and a patient experiences excruciating pain when the site of the abruption is palpated. If the placenta is posteriorly implanted, uterine tenderness itself may be absent, but the patient may experience lower back pain.
Interference with the diffusion of oxygen in the intervillous area from the maternal to the fetal side is to be expected in placental abruption. Fresh meconium staining of the amniotic fluid may be found in artificial or spontaneous amniorrhexis, perhaps reflecting fetal stress or distress. Separation of 50% or more of the total effective placental area usually is incompatible with preservation of fetal life.
|
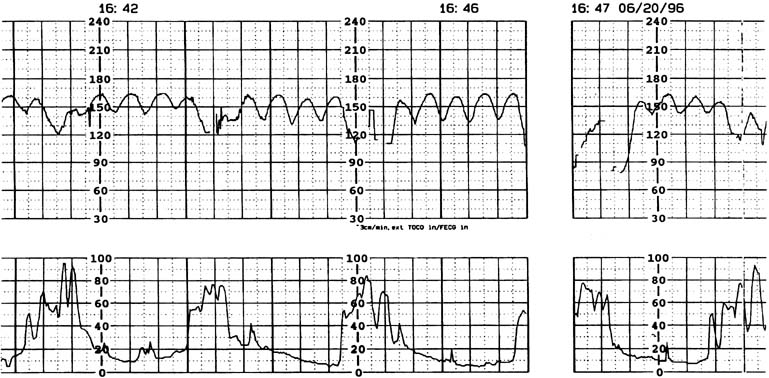
Continuous electronic fetal heart rate monitoring and uterine activity assist the clinician in the assessment of the severity of the abruption. Even if uterine contractions are irregular, their amplitude frequently exceeds that of normal labor, and the baseline tone often is increased. A rapidly enlarging uterus may reflect increasing concealed hemorrhage, which confirms the severity of the separation. Fetal heart rate monitoring may display various abnormalities, including tachycardia, loss of variability, sinusoidal pattern (Fig. 4), pseudosinusoidal pattern,109 or late decelerations. A recent study analyzed fetal heart rate tracings from 40 pregnant Japanese women with placental abruption.110 Eighty percent did not show normal fetal heart rate patterns. They also found that bradycardia and undetectable variability appeared more frequently in cases with larger separation compared to those with smaller separation. By contrast, 20% of women showed a normal fetal heart rate pattern throughout the monitoring period, regardless of the presence of clinically overt and macroscopically confirmed abruption.110 All these women showed a 5 minute Apgar score of 7 or greater, cord blood pH of 7.1 or greater, and separation <25%. However, it is important to remember that a normal heart rate tracing on admission in a patient with suspected abruptio placentae is not a cause for complacency. Rapid deterioration of fetal condition may occur in this situation. This concern cannot be overemphasized.
Maternal hypovolemia caused by extensive hemorrhage is manifested clinically by the cardinal signs of shock: a low or rapidly falling blood pressure, a rapid and weak pulse, generalized pallor with cold and clammy extremities, tachypnea, and agitation or lassitude. The intense compensatory vasoconstriction that results may yield a blood pressure within or above normal range, but it does so at the expense of decreased tissue perfusion in other areas of the body, and the patient is orthostatic.
Initial laboratory values may not be helpful in the diagnosis of abruptio placentae. A patient's hematocrit may be normal or low, depending on her initial hematologic status and the elapsed time interval in which compensatory hemodilution can occur. The leukocyte count is variable, but often there may be a mild or moderate leukocytosis. Coagulation defects manifested by decreased platelets, elevated prothrombin time (PT), decreased fibrinogen levels, and elevated fibrin split products are more likely to occur with abruption than with placenta previa, but their presence is not pathognomonic. Both the Kleihauer-Betke and CA-125 tests are of little clinical value in the workup of patients with placental abruption.111, 112
Patients with placenta previa often present with a clinical picture similar to abruption. Because the two conditions are managed differently, distinction is critical. Several authors emphasize the use of real-time ultrasonography for the diagnosis of third-trimester bleeding. The accuracy of ultrasonic diagnosis of placenta previa is highest by transvaginal ultrasound and is between 93% and 98%.113, 114 The availability of real-time ultrasonography on the labor and delivery suite allows a safe environment for rapid placental localization and exclusion of placenta previa.
Historically, ultrasonography has been less helpful, however, in the diagnosis of placental abruption, with sonographic evidence being rarely seen or difficult to identify. As a result, the sonographic diagnosis of abruptio placentae classically has been described as a diagnosis of exclusion when ultrasound has failed to show a placenta previa and other causes of vaginal bleeding have been ruled out. In the past, only few patients with clinical evidence of placental separation displayed the classic sonographic abnormalities of a retroplacental hypoechoic area or dissection of blood between the fetal membranes.115
With the routine use of ultrasonography to assess bleeding early in pregnancy, placental separations have been noted in the first and second trimesters. Many of these pregnancies, however, have subsequently progressed normally. Although most clinicians still rely mainly on ultrasonography to rule out placenta previa, it is important to note that the ability to diagnose placental abruption by ultrasonography depends partly on the stage of the process. If the abruption is mild or if bleeding occurs without a large accumulation of blood (i.e., it escapes externally), ultrasonographic findings may be negative.116
The detection rate of placental abruption by ultrasound has been reported in the literature to range anywhere from 2% to 50%.108, 113, 117 However, most studies were retrospective, performed before technologically advanced ultrasound machines came into existence, and did not encompass the wide spectrum of sonographic findings of abruption. Studies often also did not show consistent time intervals between onset of clinical symptoms, ultrasound examination, and delivery.
Sholl assessed 48 patients with a clinical diagnosis of abruption and noted that only 25% had retroplacental or retromembranous clots.117 Ultrasonography did not appear to have a large impact on management in his patients. Huang and colleagues noted that 46.8% of patients who had a clinical and sonographic diagnosis of abruption were found to have an abruption.118 Jaffe and associates discovered that of abruptions confirmed both clinically and pathologically, ultrasound identified them in only 50% of cases.113 A recent 2002 study examined the clinical usefulness of sonography in diagnosing placental abruption.119 These authors found the sensitivity, specificity, positive predictive value, and negative predictive value of sonography to be 24%, 96%, 88%, and 53%, respectively.119
Because of the advances in ultrasound resolution, imaging, and interpretation, we recently set out to prospectively determine the diagnostic accuracy of targeted sonography in detecting abruptio placentae in patients with vaginal bleeding. The ultrasound examination targeted for the following seven sonographic features of abruption: (1) preplacental collection under the chorionic plate (between placenta and amniotic fluid) (Fig. 5); (2) "jello-like" movement of the chorionic plate with fetal activity; (3) retroplacental collection (between placenta and myometrium) (Fig. 6); (4) marginal collection (at the placental margin) (Fig. 7); (5) subchorionic membranous collection (between the membranes and uterine wall) (Fig. 8); (6) increased placental thickness or echogenicities (defined as greater than 4–5 cm perpendicular to the plane of the placenta throughout pregnancy (Figs. 9 and 10); and (7) intra-amniotic hematoma (collection within the amniotic fluid) (Fig. 11).
|

|

|

|

|

|

|

We found that in 73 patients presenting with vaginal bleeding, the sensitivity, specificity, positive predictive value, and negative predictive value of targeted ultrasound in detecting abruptio placentae (confirmed macroscopically) were 80%, 92%, 95%, and 69%, respectively. Our sensitivity is higher than what has been previously reported. We also set out to determine if the sonographic diagnostic accuracy of abruption was compromised in patients with PROM.120 We found the sensitivity of ultrasound to detect placental abruption to be higher in PROM patients versus those with intact membranes (94% vs. 71%), and surmised these findings may have been influenced by the difference in gestational ages at the time of ultrasound examination in these two populations (27 weeks in PROM patients vs. 33 weeks in patients with intact membranes).
Some of the difficulty in sonographically diagnosing abruptions is attributable to the sonographic changes that occur with time. Nyberg and colleagues reviewed 75 cases of placental abruption detected on ultrasonography retrospectively.121 The locations noted were subchorionic in 81%, retroplacental in 16%, and preplacental in 4%. They noted that the echogenicity of the clot changed with time. A newly formed or acute hemorrhage is hyperechoic or equal in appearance to the placenta. Over 1 week, the hematoma becomes hypoechogenic with respect to the placenta and then sonolucent within 2 weeks.121 Abruptions also can be confused with or mistaken for other lesions on ultrasound, such as succenturiate lobe, uterine myoma, chorioangioma, and coexisting molar pregnancy.121 Repeating the ultrasonography over time may be helpful in reaching a diagnosis.
Other facts to keep in mind to further improve the diagnostic accuracy of detecting abruptions on ultrasound include the following: (1) even in the presence of placenta previa, placental separation should be rule out when it is suspected; and (2) a true marginal blood collection emanating from a low-lying placenta may falsely give the impression of a previa if the collection is located just above the internal cervical os. In such cases, a “fundal” placental location can be a clue that an abruption (rather than placenta previa) may be present.
The size and location of the abruption identified by sonography may be important prognostically. Retroplacental collections have a worse prognosis for fetal survival than subchorionic abruptions. In addition, large retroplacental hemorrhages (more than 60 mL, or greater than 50% of placental involvement) have been associated with a fetal mortality rate of 50% or greater, whereas similar-size subchorionic hemorrhages have a 10% fetal mortality rate.122 Ball and colleagues found that the presence of a sonographically detected subchorionic hemorrhage increased the risk for miscarriage, stillbirth, and preterm labor, with a large hemorrhage having a worse prognosis than a small one.123
Although not all patients with abruption have positive evidence on ultrasonography, those who do should undergo close surveillance. We prospectively correlated positive and negative sonographic signs of abruption with perinatal outcomes in 91 patients presenting with vaginal bleeding. We found that those with positive sonographic signs of abruption were more likely to have fetuses with lower gestational age and birth weight at delivery, higher rates of preterm births, lower 1-minute and 5-minute Apgar scores, and higher rates of cesarean deliveries.124 Glantz also found positive sonographic findings of placental abruption to be univariately associated with two-fold to three-fold greater subsequent preterm delivery, low birth weight, and neonatal intensive care unit admission.119
In summary, ultrasonography is used effectively to localize the placenta and determine if a placenta previa is present. With advances in ultrasound technology and recognition of fine detail, the diagnosis of placental abruption by targeted ultrasonography should not be a diagnosis of exclusion. In our experience, the direct recognition of sonographic signs of abruption has high sensitivity and positive predictive value.
Real-time scanning also may be used both to identify abruption and to monitor hemodynamically stable patients with a suspected abruption in early pregnancy. In such cases, serial evaluations are useful in monitoring abruption size and fetal growth. In approximately 60% of patients with chronic abruption (delay of at least 7 days after the initial hemorrhage before delivery occurs), an entity called chronic abruption–oligohydramnios sequence may be seen.125 This involves initial documentation of normal amniotic fluid volume with eventual development of oligohydramnios without ruptured membranes. This is important clinically because in those patients with chronic abruption–oligohydramnios sequence at less than 20 weeks, there is an earlier gestational age at delivery, greater chance for chorioamnionitis, and higher perinatal mortality. The pathophysiologic origin of the oligohydramnios is unclear but may result from the rupture of membranes; another less likely possibility is placental insufficiency and decreased fetal renal perfusion.
Magnetic resonance imaging also has been suggested as a tool to successfully diagnose placental abruptions; however, disadvantages of this modality include cost, lack of portability, and examination time.126
MATERNAL COMPLICATIONS
The following are the principal maternal complications associated with premature separation of the placenta: (1) hemorrhagic shock resulting from acute whole blood loss and resultant contraction of the intravascular compartment; (2) generalized coagulopathy occurring because of active consumption of clotting factors within the vascular tree and consequent secondary fibrinolysis; (3) ischemic necrosis of distant organs. The organs most frequently involved are the kidneys and the anterior pituitary gland. Acute renal failure is a serious complication and may lead to maternal death; and (4) preterm PROM resulting from decidual hemorrhage.
A recent study examining maternal outcome after abruptio placentae found that women presenting with a stillborn infant on admission were more likely to require transfusions and have complications, such as DIC and acute renal failure, than women presenting with a live fetus.127
Hemorrhagic Shock
Hemorrhagic shock is caused by an absolute reduction in peripheral circulating blood volume along with subsequent tissue hypoperfusion. It has been stated that the shock that occurs in patients with abruptio placentae frequently is out of proportion to the observed blood loss and is a result of profound hypovolemia.
The end point of persistent hypotension is asphyxia of both the fetus and mother; therefore, the immediate treatment is replacement of the intravascular volume deficit as rapidly as possible and restoring effective perfusion. Crystalloid fluids should be infused until proper crossmatched blood is available. Crystalloid therapy initially should involve volumes two- to three-times in excess of the actual hemorrhage, because shock often is associated with major fluid shifts from the intravascular to the extravascular compartments. The highest maternal morbidity and mortality rates occur with severe cases of abruptio placentae. Although some patients may die from pituitary or renal damage, most die from hemorrhagic shock or overvigorous fluid replacement.
General Coagulopathy
Since the turn of the century, clinicians and investigators have observed the presence of a bleeding diathesis accompanying some cases of premature separation of the placenta. DeLee and Dieckmann reported incoagulable blood in some of their patients, and in 1936, Dieckmann reported low levels of fibrinogen in patients with severe abruptio placentae.11, 15 Clinically, this complication presents as generalized bleeding from mucous membranes, intravenous sites, or subcutaneous tissues; as profuse uterine hemorrhage; or as uncontrolled bleeding at the time of surgery.
Various investigators have attempted to elucidate the cause of this abnormal bleeding. In 1886, Wooldridge first reported intravascular clotting after injection of tissue extract.128 In 1917, Obata noted defective coagulation and findings similar to eclampsia in mice injected with a placental extract.129 The investigations of Page and coworkers confirmed that DIC is the cause of the hypofibrinogenemia that is seen in abruptio placentae.130 Hypofibrinogenemia was produced by injecting animals with decidual and placental extracts, which are rich in thromboplastin. The inciting event leading to DIC with placental abruption is thought to be entry of thromboplastins from the placental injury site into the circulation. The thromboplastins cause widespread intravascular activation of the clotting cascade. The concept of DIC also has been referred to as consumption coagulopathy, defibrination syndrome, and acquired hypofibrinogenemia. As the name implies, widespread activation of the coagulation system within the vascular tree produces a consequent depletion of various clotting elements and a resultant hemorrhagic state. The extensive conversion of fibrinogen to fibrin results in a decrease in the concentration of fibrinogen. Secondary fibrinolysis leads to the formation of fibrin degradation products (FDP), which, by their anticoagulant effect, further compromise the hemostatic system. Levels of prothrombin, factor V, factor VIII, and platelets also are decreased. Normal hemostasis depends on a critical balance between coagulation and fibrinolytic systems to maintain the vascular fluid state while allowing clot formation locally at injury sites. In abruptio placentae, disruption of this balance can occur. DIC is seen in 10% of cases of abruption and is seen mostly in severe cases of abruption associated with fetal death or massive hemorrhage.106
The following hypotheses have been advanced to account for the lowered plasma fibrinogen levels in premature separation of the placenta: (1) increased utilization of fibrinogen by thrombin results in conversion to fibrin, which is deposited throughout the microvasculature. This concept is the most widely cited; (2) continual fibrin deposition in the retroplacental clot has been suggested. However, Pritchard and Brekken found that conversion of fibrinogen to fibrin at the placental site did not play a major role in the etiology of severe hypofibrinogenemia;131 and (3) destruction of fibrin and fibrinogen by primary fibrinolysis appears to play a significant role. The increase in fibrinolytic activity is thought to be secondary to DIC and may reduce fibrin deposits in the microcirculation.
In addition to its association with severe placental abruption, acquired hypofibrinogenemia also has been reported in cases of amniotic fluid embolism, long-standing fetal death in utero, septic abortion, eclampsia, and delayed postpartum hemorrhage.
The phenomenon of consumption coagulopathy leads to patient injury because of two problems: the bleeding diathesis caused by diminished coagulation factors and elevated FDP, and the localized tissue necrosis in target organs because of fibrin deposition in small blood vessels. As a protective mechanism, the fibrinolytic system is activated secondarily, and dissolution of the fibrin clots by plasmin may protect the local tissue from anoxia. This delicate balance between fibrin deposition and degradation is present in the body at these times. If this secondary fibrinolysis and fibrinogenolysis become excessive, the decreased coagulation factors resulting from consumption are augmented by destruction of the same factors by plasmin, and the hemorrhagic situation is made worse. The degradation products of fibrin and fibrinogen also interfere with fibrinogen conversion to fibrin. Fibrinolytic problems in abruptio placentae are mostly secondary, with progressive activation of the system occurring only after an initial phase of intravascular coagulation.
The complications of hypofibrinogenemia have been detected in one third to one half of patients having signs and symptoms of severe placental separation. Most patients with abruptio placentae have the milder form and exhibit no clinical difficulties with the clotting mechanism. Placental separation precedes the depression of the fibrinogen levels, and the depletion process progresses as long as the pathologic condition persists and the uterus remains unevacuated. Commonly used coagulation tests, such as PT and partial thromboplastin time, are insensitive indicators of DIC; more than 50% of clotting factors must be consumed before these test results become abnormal.132 Fibrinogen levels are sensitive indicators of DIC on serial testing. A fibrinogen concentration of less than 200 mg/dL in a pregnant patient is abnormal. Clinical evidence of bleeding may appear when the value is less than 100 mg/dL. The platelet count decreases in concert with fibrinogen levels, but in most cases, there is a greater decrease in the fibrinogen level than in the platelet count.132 The most sensitive laboratory test for diagnosis of coagulopathy related to abruption may be the determination of fibrin–fibrinogen degradation products by a variety of techniques, including D-dimer assays.133
Ischemic Necrosis of Distant Organs
Ischemic damage to the kidneys is a well-documented complication of severe abruptio placentae and takes the form of acute tubular necrosis, bilateral cortical necrosis, or both. The pathologic changes are explained on the basis of inadequate blood supply and hypoxia from hemorrhagic hypovolemia or obstruction secondary to focal fibrin deposits in the precapillary arterioles from DIC. Other suggested mechanisms are vasospasm of the supplying arteries caused by humoral (serotonin release) or reflex (uterorenal) factors.
Acute renal cortical destruction histologically reveals ischemic coagulation necrosis of all elements in the cortex, with extensive thrombosis in the interlobular arteries and occasional involvement of the glomerular afferent arterioles and capillaries. This probably represents a direct effect of DIC.
Acute tubular necrosis, the most common cause of anuria in obstetric accidents, generally is a result of hemorrhagic shock with resultant anoxic insult to the tubular structures of the renal medulla. Lower nephron injury secondary to hemoglobinemia from erythrocyte hemolysis must be kept in mind in patients with abruptio placentae, especially when multiple blood transfusions have been administered.
When extreme oliguria or anuria develops, it is impossible to initially distinguish between acute tubular necrosis and acute cortical necrosis. Acute renal failure with lower nephron damage usually occurs later in the abruption process and is reversible after a period of time. In contrast, the pattern of acute cortical necrosis shows involvement early in the abruption process; if the condition is untreated by dialysis, the clinical course progresses to death from uremia in 7 to 12 days. The urine that is obtainable invariably gives positive test results for albumin, and multiple formed elements are seen on microscopic examination.
The key to prevention of renal ischemic damage is vigorous blood and fluid therapy to combat hypovolemic shock. In addition to pathologic involvement in the kidneys, necrotic lesions also may be found in the liver, adrenal glands, and pituitary gland. Anterior pituitary necrosis with delayed onset of the signs and symptoms of hypopituitarism originally was discussed by Sheehan in 1937.134
Preterm Premature Rupture of the Membranes
The precise mechanism by which placental abruption leads to preterm PROM has not been delineated. However, a recent study examined the effects of thrombin (produced by vascular damage associated with decidual hemorrhage and/or inflammation) on expression of proteolytic enzymes (matrix metalloproteinase-1).135 They found that aberrant thrombin output from an acute or chronic placental abruption could promote breakdown of fetal membranes via increased enzyme activity. Increased matrix metalloproteinase activity in the amniochorion before term is thought to compromise fetal membrane integrity and therefore lead to preterm PROM.135
FETAL AND NEONATAL COMPLICATIONS
There are many possible fetal and neonatal complications from abruptio placentae. The perinatal morbidity and mortality rate associated with abruption is as high as 20% to 40%,83 accounting for 15% of all perinatal deaths.30 However, the overall perinatal mortality rate from placental abruption may be decreasing secondary to improvements in obstetric and neonatal care. The three major causes of perinatal death are fetal anoxia, exsanguination (because, in rare cases, rupture of fetal placental vessels can occur), and, especially, prematurity.26, 136 Almost 20% of abruptions are manifest between 28 and 32 weeks, whereas another 20% of cases present before 28 weeks.106 A recent study found the occurrence of placental abruption to be higher in preterm pregnancies, complicating as much as 5.1% of preterm deliveries.137 Ananth and colleagues recently showed an associated perinatal mortality rate of 119 per 1000 births with abruption (compared with perinatal mortality rate of 8.2/1000 in the reference United States population).6 The high mortality with abruption was found to be caused, in part, by its strong association with preterm delivery; 55% of the excess perinatal deaths linked with an abruption delivery were because of early gestational age alone.6 In this study, placental abruption was recorded in 46,731 pregnancies. Of these, 51% ended before 37 completed weeks (compared with 10.1% of all other births).6
In a recent study (n = 53,371) using data from Mount Sinai Hospital (New York), the degree of placental separation had a profound effect on stillbirth (relative risk: 31.5 for 75% placental separation), although this was evident only among women with 50% or more placental separation138 ( Fig. 12). For preterm delivery, however, this risk was substantially increased, even for mild forms of placental separation (relative risk: 5.5 for 25% placental separation)138 (Fig. 13).
|
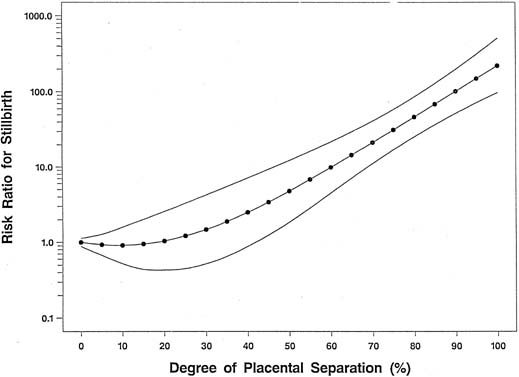
|
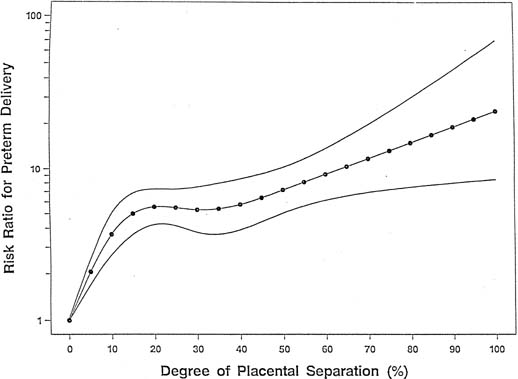
Another major possible complication of abruptio placentae is intrauterine growth restriction, emphasizing that abruption in most cases is the final event of a long-standing pathologic process. Hibbard and Jeffcoate found 81% of infants born at less than 36 weeks weighed less than the mean birth weight for gestational age.139 Our group recently set out to evaluate whether the association between low birthweight and placental abruption is mediated through preterm birth or restricted fetal growth.140 Among abruption cases, 60.3% were low birthweight in comparison with 11.2% of controls (OR, 13.7; 95% CI 7.4–25.2). Furthermore, placental abruption had a significantly increased association with preterm birth in both small for gestational age (OR, 17.4; 95% CI 4.6–64.9) and appropriately grown fetuses (OR, 15.8; 95% CI 8.4–29.8). Therefore, we found that the association between placental abruption and low birthweight is chiefly mediated through preterm birth.140
The likelihood of a normal neonatal outcome decreases with the severity of abruption. Poor outcome may be caused by the fact that perinatal hypoxic–ischemic injury starts in utero, caused by an interruption in placental blood flow and gas exchange, often extending into the recovery period after resuscitation. In a recent study comparing patients having placental abruption with or without antepartum hemorrhage, the patients without antepartum hemorrhage had higher rates of stillbirth and perinatal mortality, along with poorer 1-minute and 5-minute Apgar scores.141 The authors surmised that vaginal bleeding may predict the possibility of abruptio placentae and prompt early intervention. Therefore, in those patients without bleeding, later detection may occur, with a larger area of placental separation and more fetal distress.141 An increased risk for cerebral palsy has been reported with moderate to severe abruptions.142 Increased risks for perinatal asphyxia,143 intraventricular hemorrhage,142 and periventricular leukomalacia and extensive periventricular hemorrhage144 also can be seen with placental abruption. However, these also may be related to premature delivery secondary to the abruption itself. In addition, with abruption there is a three-fold increase in the rate of major malformations, mostly involving the central nervous system.132
MANAGEMENT
A plan of management for patients with placental abruption must take into account the condition of both mother and fetus. Presented here is a discussion of the initial evaluation and stabilization of patients, evaluation of the maternal hemostatic mechanisms, formulation of a satisfactory therapeutic plan, and postpartum care.
INITIAL EVALUATION AND STABILIZATION
General Guidelines
Patients presenting with antepartum bleeding should be immediately admitted to the labor and delivery suite. Maternal vital signs should be assessed and taken initially, and electronic fetal heart rate and uterine activity monitoring should be instituted. Remember that a normal blood pressure may be misleading in hypertensive patients, because a true underlying hypertensive state may not be evident until restoration of intravascular volume is performed. While a history is obtained and a physical examination is performed, a large-bore intravenous catheter is inserted, and a second line also may be considered if heavy bleeding is present. This allows replacement of fluid and blood products as needed. Blood should be drawn for hemoglobin, hematocrit, PT, fibrinogen, fibrin split products, electrolytes, and renal function studies. A specimen should be sent for type and crossmatch, and several units of blood must be made available. After a brief initial evaluation, a careful speculum examination should be performed to ensure that the bleeding is coming from the uterine cavity rather than the perineum, vagina, or cervix.
Because placental abruption often is accompanied by concealed hemorrhage, blood loss may be severely underestimated. Acute volume loss initially may cause vasoconstriction, resulting in normal or elevated blood pressure. Hemoglobin concentrations also may fail to reflect accurately acute blood loss. When blood loss seems significant or concealed abruption is suspected, central arterial (Swan-Ganz catheter) or central venous pressure invasive hemodynamic monitoring may be helpful. Insertion of a Foley catheter provides additional information about the patient's volume status and permits accurate evaluation of urine output. Associated medical and obstetric diseases such as preeclampsia and diabetes mellitus also should be identified. Gestational age and fetal status must be rapidly and accurately assessed. The responsible members of the anesthesia and pediatric departments should be informed of the patient's status.
Determination of fetal status involves the use of both heart rate monitoring and ultrasonography. Real-time ultrasonography always should be available on the labor floor. Ultrasonography is most helpful as an aid in the differential diagnosis of antepartum bleeding, and it may directly identify one or more of the abruption signs. If the placenta is found to be fundal in location, the diagnosis of placenta previa is virtually ruled out. Transvaginal ultrasonography may be helpful in assessment of questionable placenta previa near the os. If the placenta is not covering the os, the clinician should check for the insertion site of the placental cord. Vasa previa also is a cause of bleeding that can be diagnosed by ultrasonography. Ultrasound also can determine the gestational age and estimated fetal weight. Finding an abruption prospectively on ultrasound has been found to correlate with perinatal outcomes such as lower gestational age and birth weight at delivery, higher rate of preterm births, lower 1-minute and 5-minute Apgar scores, and higher rate of cesarean deliveries.124 Therefore, when ultrasound identifies a placental abruption, close surveillance of both mother and fetus is indicated. Serial ultrasonographic examinations have been used in patients with mild, stable abruptions to measure the volume of the retroplacental clot and correlate this information with antepartum heart rate testing and maternal symptoms. Three fetuses were monitored in this manner for several weeks. Fetal distress was observed in only one instance, when the retroplacental clot volume exceeded 480 mL.145
Continuous fetal monitoring, as already mentioned, should be implemented as soon as possible because fetal distress may develop in as many as 60% of patients presenting with a live fetus.30 In an extensive abruption, fetal distress, if not fetal death, will likely be present, as evidenced by persistent late decelerations or bradycardia. With excessive uterine contractions, the monitor may show frequent repetitive late decelerations. In a patient with severe abruption, a tracing that shows a fetal bradycardia similar in rate to the maternal heart rate should have the fetal rhythm confirmed by ultrasonography. The fetal heart rate electrode affixed to the fetal scalp can, in cases of fetal death, detect maternal electrical cardiac impulses and lead to the misdiagnosis of fetal distress. This also has been reported by others in the case of fetal bradycardia and normal fetal heart rate patterns.146, 147, 148 The fetal heart rate can be normal initially, but this finding is not reassuring. The process of placental abruption can be dynamic and progress without warning, leading quickly to fetal distress or even death. In cases of maternal trauma and suspected abruption, patients may need to be monitored for an extended time, perhaps at least 12–24 hours. Kettel and colleagues describe a case in which fetal bradycardia 12 hours after trauma was the first significant sign of abruption.149 Other reports recommend that patients with minor or insignificant injuries be monitored for at least several hours.150
Uterine activity in placental abruption may show a distinctive pattern on the tocographic monitor. The resting tone may exceed 25 mmHg, compared with 5–12 mmHg during normal labor.151 The frequency of contractions may be as high as five or more over 10 minutes, with a mean of 5.6 per 10 minutes.152
The role of Doppler studies in cases of active abruption has not been clearly determined. Doppler flow studies performed in one case of abruption showed elevated systolic–diastolic ratios for the umbilical artery and the uterine vessels.153 This report also noted a dicrotic notch in the umbilical artery waveform. These changes may reflect increased vascular resistance secondary to the actual retroplacental clot or perhaps prostaglandin released during the abruption, which may be associated with fetal death in some cases.153 Hoskins and associates found elevated systolic–diastolic ratios of the umbilical artery in cocaine-abusing patients with abruption.154 Others have found an increased risk for placental abruption if abnormal umbilical artery flow velocity waveforms are seen in patients with third-trimester bleeding.155 Conversely, a prospective study on the use of umbilical artery Doppler studies in placental abruption found that they were not useful or reliable in predicting fetal outcome.156 A recent study of 97 cases of placental abruption that underwent Doppler ultrasonographic studies found they were not effective in the prenatal prediction of abruption and were generally normal.157
As noted previously, laboratory data are less specific in differentiating abruptio placentae from placenta previa. Anemia may be demonstrated in either group of patients. Approximately 50% of patients with placental abruption, however, have laboratory evidence of a coagulopathy as indicated by thrombocytopenia, a prolonged PT, hypofibrinogenemia, and elevated fibrin split products. Most clinicians use a fibrinogen value of 150 mg/dL as the critical volume below which DIC should be expected. In abruptio placentae, sudden fluctuations in the fibrinogen concentration may occur as a result of destruction from DIC and rapid regeneration by the liver. Therefore, the coagulation profile should be repeated every 2–4 hours.
A red top tube taped to the wall at the bedside (“poor man's test”) can provide invaluable information on the patient's coagulation status before receiving the laboratory results. A clot should form within 6–8 minutes. If it does not, or if it forms and lyses within 30 minutes to 2 hours, a significant coagulopathy probably is present. Steps to correct this coagulopathy may be initiated before the full panel of laboratory studies has been completed.
Fluid replacement is guided by two major goals: re-establishment of hemodynamic stability and correction of the coagulopathy. Fresh whole blood is the ideal substance for replacement because it provides red blood cells, platelets, and clotting factors. However, fresh whole blood is difficult to obtain in most centers and probably does not offer major advantages except for the decreased transmission of disease. A patient carefully managed with component therapy will do well in most cases. Despite routine screening of all donors, the risks of blood product replacement should not be taken lightly, because a risk of posttransfusion hepatitis exists. With DIC, fibrinogen is the coagulation factor that most often requires replacement. A fibrinogen level less than 100 mg/dL may indicate the need for replacement with fresh-frozen plasma. One unit of fresh-frozen plasma can be expected to raise the plasma fibrinogen level by about 25 mg/dL. The effect of cryoprecipitate is less predictable. Four or five units can be administered, with the need for further therapy dictated by laboratory testing.
Platelet transfusion rarely is necessary but may be used if operative delivery is planned in a patient whose platelet count has decreased to less than 50,000/mm3,158 or if spontaneous bleeding is occurring and the platelet count is less than 25,000/mm3.158 Each bag of platelet concentrate administered increases the count by 7,000–10,000/mm3.158 Serial measurements of electrolytes, especially potassium, should be closely monitored in patients undergoing massive transfusion.
Urine output should be maintained at no less than 30 mL/h and hematocrit should be maintained at 30%. Because heparin or fibrinolytic inhibitors may lead to more severe hemorrhage, they should not be used in patients with DIC.
Therapeutic Plan
In contrast to the more conservative trend that characterizes the management of placenta previa, management of abruptio placentae has for the most part become more aggressive. In the past, studies have noted the numerous deaths among viable fetuses alive at the time of admission and have urged more liberal use of cesarean section for the delivery of patients with placental abruption.159 However, some patients may be candidates for closely monitored ambulatory obstetrical management. This includes patients who are in stable condition with a small resolving abruption, no increased uterine activity, and reassuring results of fetal surveillance.160
In general, the longer the interval between diagnosis and delivery, the greater the risk for maternal complications and the poorer the outlook for fetal or neonatal salvage. If DIC occurs, its onset usually takes place within 8 hours of placental abruption. Pritchard and Brekken report that all patients in whom potentially serious hypofibrinogenemia develops, have it develop within this time period.131
The timing and method of delivery depend on maternal and fetal condition, gestational age, and cervical status. The premature fetus with a mild abruption and minimal bleeding may be managed expectantly with close observation, because this often is a self-limiting event.161 Tocolysis may be considered and has been used with caution in certain cases. It may be beneficial in the scenario of a stable mother and fetus without distress or complications, with positive sonographic signs of abruptio placentae, and who has only mild bleeding that is associated with uterine contractions. There is evidence that such pregnancies may be successfully prolonged (which would allow corticosteroid administration for fetal lung maturity enhancement) without increased jeopardy to the mother or fetus.117, 162 Magnesium sulfate is the tocolytic agent of choice because betamimetic agents can have adverse hemodynamic effects on a bleeding patient by accentuating further signs of hypovolemia (hypotension and tachycardia). In the premature fetus with persistent, heavy vaginal bleeding, however, use of tocolytics would be contraindicated, and expeditious delivery is recommended. In general, any attempt at tocolysis should be weighed against the severity of abruption and likelihood of neonatal survival and morbidity.
An important aspect of the treatment is continuous, careful monitoring of mother and fetus for any signs or symptoms of deterioration. If the abruption is adversely affecting maternal or fetal condition, delivery should be performed. In cases of premature placental separation, cesarean delivery should be performed liberally for maternal or fetal reasons.
The route of delivery for patients with placental abruption and a viable fetus generally should be by rapid cesarean delivery unless vaginal delivery can be expected promptly. Many patients with placental abruption already have contractions; therefore, cesarean delivery may not be necessary. Abruption may even cause a rapid and tumultuous labor. A recent study suggests that in the absence of life-threatening hemorrhage, approximately 50% of patients with placental abruption, but a normal fetal heart rate tracing, could have a vaginal delivery.158 In such cases, neonatal outcomes comparable with those obtained in infants born by cesarean delivery were reported. There is no specific time limit imposed on a trial of vaginal delivery as long as intensive maternal and fetal surveillance show no significant progression in abruption severity and labor is progressing satisfactorily. Oxytocin may be used to augment uterine contractions. Its use has been questioned and challenged in that it might enhance the escape of thromboplastin into the maternal circulation and therefore initiate or augment consumptive coagulopathy. However, there is no evidence to support this hypothesis.20 Remember, however, that the fetal condition may rapidly deteriorate. Patients may present with a live fetus, only to have that fetus die undelivered while awaiting vaginal delivery. In a recent study it was found that in cases of placental abruption, for those fetuses alive on admission, cesarean delivery was associated with a significant reduction (odds ratio: 0.10; 95% confidence interval: 0.05–0.20) in neonatal mortality.127 With an immature fetus or after intrauterine fetal death, attempts at vaginal delivery using oxytocin should be implemented if needed. However, a deteriorating clinical situation with increasing blood loss or a worsening coagulopathy may dictate operative intervention for maternal indications.
Management is most difficult and controversial in patients who have placental abruption and are admitted with clinical DIC. If bleeding is excessive, the condition must be promptly treated after evaluation of the previously mentioned hemostatic parameters. The most effective and definitive treatment is correction of the underlying process (i.e., the release of tissue thromboplastin into the circulation by the damaged placenta) by delivery of the placenta and fetus. If vaginal delivery is accomplished quickly without trauma, prompt restoration of the hemostatic mechanism usually results. Even in the most severe cases, clinically evident coagulopathy usually resolves by 12 hours after delivery. There is a decrease in the fibrin deposition products that interfere with thrombin action and platelet function and an increase in fibrinogen, factor V, and factor VIII. The platelet count returns to normal at a slower rate. This delay is caused by the time required for maturation and release of new platelets from the bone marrow. The expected order of normalization of the coagulation tests is PT followed by fibrinogen, FDP, and platelets. A clinical trial has found that the use of activated protein C intravenously in cases of placental abruption complicated by DIC resulted in rapid improvement of the DIC picture within 1 to 2 days. No adverse events related to the use of activated protein C were observed.163 Further study, however, is needed to elucidate its value in DIC.
If a cesarean delivery is to be performed, the patient should be receiving fluids, oxygen, and replacement products. Coagulation factors should be given during the surgery. If given before surgery, they may provide little improvement at the time of surgery as a result of the ongoing DIC. Surgery should be performed quickly but in a meticulous manner. The surgeon should avoid unnecessary trauma to the tissues and should ligate or cauterize all bleeding points, even small bleeders that otherwise might be overlooked. The abdominal incision should be drained by a closed system. If vaginal delivery is expected, which in some cases, depending on maternal and fetal status, may be the preferred route, the obstetrician should attempt an amniotomy as soon as possible, because it may benefit labor and also allows the placement of internal monitoring if desired. If the fetus is immature, it may be best to leave the membranes intact. The intact sac may be a better dilatory wedge than a small fetal part that can be poorly applied to the cervix.21 After delivery, uterine blood loss can be decreased by quick infusion of oxytocin and appropriate uterine massage. The episiotomy, if needed, should be repaired meticulously and the cervix and vagina carefully examined for lacerations.
In a patient with extensive uterine involvement and uncontrollable blood loss, a hysterectomy may be indicated. A bruised Couvelaire uterus is by itself not a reason for hysterectomy. In this situation, there often is fear of uterine hemorrhage secondary to atony; however, this usually is not the rule. In most cases, the uterus will still be able to contract sufficiently, even in response to oxytocin, to prevent postpartum hemorrhage.
Placental abruption is one of the more common causes of antepartum sensitization of an Rh-negative gravida. Therefore, if delivery is not imminent, we believe that Rh immune globulin should be offered to all eligible women. Prevention of potential sensitization appears to outweigh the risks involved.164 The proper amount of Rh immunoglobulin to be administered is dependent on the extent of the fetomaternal bleed as assessed by the Kleihauer-Betke or equivalent assay.
Postpartum Care
After delivery, a patient's hemodynamic status should be carefully monitored. Judicious use of transfusion or diuretics may be required, based on central hemodynamic monitoring indices, hemoglobin concentration, and urine output. As stated previously, coagulation defects generally correct rapidly, although fresh-frozen plasma or platelet transfusions occasionally are necessary to hasten the process. Suboptimal clotting may be present at the time of delivery, and wounds must be carefully inspected for evidence of hematoma formation. Early ambulation should be practiced: McKay has drawn attention to the phenomenon of rebound hypercoagulability in patients recovering from DIC.165 Pulmonary status must be carefully monitored, especially if the patient has had rapid induction of general anesthesia and is at risk for aspiration pneumonia. Patients may have acute renal failure as a result of hypovolemia and vasospasm. Fortunately, this condition generally is reversible with proper management.
CONCLUSIONS
Because preeclampsia, small for gestational age, and placental abruption share several similarities (as evidenced by uterine and umbilical Doppler studies, placental histology, and biochemical factors), we have introduced the term "ischemic placental disease," under which we include these 3 clinical conditions. It may be that these conditions may be different clinical manifestations of a common etiology (defective/inadequate placentation). Importantly, ischemic placental disease at preterm gestations may be etiologically different from those that occur at term gestations. Preterm placental abruption may have the same pathophysiology as that of ischemic placental disease.
Abruptio placentae must be included among the most dangerous of obstetrical complications, with hazardous implications for mother and infant. For both, the total morbidity and mortality are determined by the severity of the separation, prematurity of the fetus, amount of blood lost, and degree of difficulty in the delivery process. Anoxic damage and prematurity have accounted for increased fetal loss in the past. With improvements in obstetrical and neonatal care, overall perinatal mortality may be declining. Maternal mortality is influenced mostly by the severity of ensuing shock and the presence of significant hypertension. Maternal complications have decreased because of improved techniques of blood storage and administration, as well as central hemodynamic monitoring. Vigorous therapeutic regimens instituted when coagulation defects are identified also account for improved maternal salvage.
Despite many advances in the field of obstetrics, however, placental abruption is associated with significant maternal morbidity and perinatal morbidity and mortality. With its varied causes and dynamic pathophysiologic processes, placental abruption challenges even experienced obstetricians.
REFERENCES
Iffy L, Kaminetsky HA: Principles and Practice of Obstetrics & Perinatology. 1086-1089, New York, John Wiley & Sons, 1981 |
|
Sher G: A rational basis for the management of abruptio placentae. J Reprod Med 21:123, 1978 |
|
Ananth CV, Savitz DA, Bowes WA Jr et al: Influence of hypertensive disorders and cigarette smoking on placental abruption and uterine bleeding during pregnancy. Br J Obstet Gynaecol 104:103, 1997 |
|
Sholl J: Abruptio placentae: Clinical management in non-acute cases. Am J Obstet Gynecol 156:40, 1987 |
|
Saftlas AF, Olson DR, Atrash HK et al: National trends in the incidence of abruptio placentae, 1979–1987. Obstet Gynecol 78:1081, 1991 |
|
Ananth CV, Wilcox AJ: Placental abruption and perinatal mortality in the United States. Am J Epidemiol 153:332, 2001 |
|
Freud S: Veber Coca. Centralbl f d ges Therap. 2:289, 1884 |
|
Freud S: On coca In: Byck R (ed): Cocaine Papers. pp 49-73, New York, Stonehill Publishing, 1974 |
|
Ananth CV, Peltier MR, Chavez MR et al: Recurrence of ischemic placental disease. Obstet Gynecol. 2007 Jul;110(1):128-33. |
|
Rigby E: An Essay on the Uterine Hemorrhage Which Precedes the Delivery of the Full-Grown Fetus. London, 1776 |
|
DeLee JB: A case of fetal hemorrhagic diatheses with premature detachment of the placenta. Am J Obstet Gynecol 44:785, 1901 |
|
Couvelaire A: Deux novelles observations d'apopoloxie uteroplacentaire. Ann Gynecol Obstet 9:486, 1912 |
|
Williams JW: Further observations concerning premature separation of the normally implanted placenta. J Obstet Gynaecol Br Emp 32:259, 1925 |
|
Wilson P: Uteroplacental apoplexy in accidental hemorrhage. Surg Gynecol Obstet 34:57, 1922 |
|
Dieckmann WJ: Blood chemistry and renal function in abruptio placentae. Am J Obstet Gynecol 31:734, 1936 |
|
Pritchard JA: Treatment of defibrination syndromes of pregnancy In: Ratnoff OD (ed): Treatment of Hemorrhage Disorders. p 175, New York, Harper & Row, 1968 |
|
Ananth CV, Smulian JC et al, Demissie K: Placental abruption among singleton and twin Births in the United States: risk factor profiles. Am J Epidemiol 153:771, 2002 |
|
Rasmussen S, Irgens LM, Bergsjo P et al: The occurrence of placental abruption in Norway 1967-1991. Acta Obstet Gynecol Scand. 1996 Mar;75(3):222-8. |
|
Ananth CV, Oyelese Y, Yeo L et al: Placental abruption in the United States, 1979 through 2001: temporal trends andpotential determinants. Am J Obstet Gynecol. 2005 Jan;192(1):191-8. |
|
Cunningham FG, MacDonald PC: Williams Obstetrics. pp 746-755, 20th edn. New York, Appleton & Lange, 1997 |
|
Pritchard JA, MacDonald PC: Williams Obstetrics, pp 702-703. New York, Appleton-Century-Crofts, 1989 |
|
Rana A, Sawhney H, Gopalan S et al: Abruptio placentae and chorioamnionitis-microbiological and histologic correlation. Acta Obstet Gynecol Scand 78: 363, 1999 |
|
Handwerker SM, Selick AM: Placental abruption after insertion of catheter tip intrauterine pressure transducers: A report of four cases. J Reprod Med 40:845, 1995 |
|
Eriksen G, Wohlert M, Ersbak V et al: Placental abruption: A case-control investigation. Br J Obstet Gynaecol 98:448, 1991 |
|
Meyer MB, Jonas BS, Tonascia JA: Perinatal events associated with maternal smoking during pregnancy. Am J Epidemiol 103:464, 1976 |
|
Naeye RL, Harkness WL, Utts J: Abruptio placentae and perinatal death: A prospective study. Am J Obstet Gynecol 128:740, 1977 |
|
Williams MA, Lieberman E, Mittendorf R et al: Risk factors for abruptio placentae. Am J Epidemiol 134:965, 1991 |
|
Hibbard BM, Hibbard ED: Aetiological factors in abruptio placentae. Part I: Epidemiology BMJ 2:1430, 1963 |
|
Paterson MEL: The aetiology and outcome of abruptio placentae. Acta Obstet Gynecol Scand 58:31, 1979 |
|
Gabbe SG, Niebyl JR, Simpson JL: Obstetrics: Normal and Problem Pregnancies. pp 505-532, 3rd edn. New York, Churchill Livingstone, 1996 |
|
Ananth CV, Wilcox AJ, Savitz DA et al: Effect of maternal age and parity on the risk of uteroplacental bleeding disorders in pregnancy. Obstet Gynecol 88:511, 1996 |
|
Pritchard JA: Genesis of severe placental abruption. Am J Obstet Gynecol 108:24, 1970 |
|
Williams JW: Premature separation of the normally implanted placentae. Surg Gynecol Obstet 21:541, 1951 |
|
McKelvey JL: Vascular lesions in the decidua basalis. Am J Obstet Gynecol 38:815, 1939 |
|
Hertig AT: Symposium on obstetrics. Clinics 4:585, 1945 |
|
Yla-Outinen SA, Palander M, Heinoken PK: Abruptio placentae: Risk factors and outcome of the newborn. Eur J Obstet Gynecol Reprod Biol 25:23, 1987 |
|
Williams MA, Mittendorf R, Monson RR: Chronic hypertension, cigarette smoking, and abruptio placentae. Epidemiology 2:450, 1991 |
|
Brink AL, Odendaal HJ: Risk factors for abruptio placentae. South Afr Med J 72:250, 1987 |
|
Ananth CV, Peltier MR, Kinzler WL et al: Chronic hypertension and risk of placental abruption: is the association modified by ischemic placental disease? Am J Obstet Gynecol. 2007 Sep;197(3):273.e1-7. |
|
Ananth CV, Vintzileos AM: Medically indicated preterm birth: recognizing the importance of the problem. Clin Perinatol. 2008 Mar;35(1):53-67 |
|
Reis PM, Sander CM, Pearlman MD: Abruptio placentae after auto accidents. J Reprod Med 45: 6, 2000 |
|
Benedetti TJ: Antepartum hemorrhage In: Gabbe SG, Niebyl JR, Simpson JL (eds): Obstetrics: Normal and Problem Pregnancies. pp 490-495. New York, Churchill Livingstone, 1986 |
|
Bunai Y, Nagai A, Nakamura I et al: Fetal death from abruptio placentae associated with incorrect use of a seatbelt. Am J Forensic Med Pathol 21: 207, 2000 |
|
Higgins SD, Garite TJ: Late abruptio placentae in trauma patients: Implications for monitoring. Obstet Gynecol 63:105, 1984 |
|
Dahmus MA, Sibai BM: Blunt abdominal trauma: Are there any predictive factors for abruptio placentae or maternal-fetal distress. ? Am J Obstet Gynecol 169:1054, 1993 |
|
Shah S, Miller PR, Meredith JW et al: Elevated admission white blood cell count in pregnant trauma patients: an indicator of ongoing placental abruption. Am Surg 68:644, 2002 |
|
Ananth CV, Smulian JC, Vintzileos AM: Incidence of placental abruption in relation to cigarette smoking and hypertensive disorders during pregnancy: A meta-analysis of observational studies. Obstet Gynecol 93:622, 1999 |
|
Spira A, Philippe E, Spira N et al: Smoking during pregnancy and placental pathology. Biomedicine 27:266, 1977 |
|
Christianson RE: Gross differences observed in the placentas of smokers and nonsmokers. Am J Epidemiol 110:78, 1979 |
|
Suzuki K, Minei LJ, Johnson EE: Effect of nicotine upon uterine blood flow in the pregnant rhesus monkey. Am J Obstet Gynecol 136:1009, 1980 |
|
Acker D, Sachs BP, Tracey KJ et al: Abruptio placentae associated with cocaine use. Am J Obstet Gynecol 146:220, 1983 |
|
Townsend RR, Laing FC, Brooke RJ: Placental abruption associated with cocaine abuse. AJR Am J Roentgenol 150:1339, 1988 |
|
Bingol N, Fuchs M, Diaz V et al: Teratogenicity of cocaine in humans. J Pediatr 110:93, 1987 |
|
Hulse GK, Milne E, English DR et al: Assessing the relationship between maternal cocaine use and abruptio placentae. Addiction 92:1547, 1997 |
|
Handler A, Kistin B, Davis F et al: Cocaine use during pregnancy: Perinatal outcomes. Am J Epidemiol 133:818, 1991 |
|
Washton AM, Gold MS, Pottash AC: Intranasal cocaine addiction. Lancet ii 1374, 1983 |
|
Siegel RK: Cocaine smoking. J Psychoactive Drugs 14:271, 1982 |
|
Siegel RK: Cocaine smoking. N Engl J Med 300:373, 1979 |
|
Jekel JF, All DF, Podlewski H et al: Epidemic free-base cocaine abuse: Case study from the Bahamas. Lancet i 459, 1986 |
|
Wesson DR, Smith DE: Cocaine: Treatment perspectives. Natl Inst Drug Abuse Res Monogr Ser 61:193, 1985 |
|
Ritchie JM, Green M: Last anesthesia. In: Gilman AG, Goodman LS, Gilman A (eds): The Pharmacological Basis of Therapeutics. pp 300-320, 6th ed.. New York, Macmillan, 1980 |
|
Sherman WT, Gautierei RF: Effect of certain drugs on perfused human placenta: X norepinephrine release by bradykinin. J Pharm Sci 61:878, 1972 |
|
Chasnoff IJ, Burns WJ, Schnoll SH et al: Cocaine use in pregnancy. N Engl J Med 313:666, 1985 |
|
Ness PM, Budzymski AZ, Olexa SA et al: Congenital hypofibrinogenemia and recurrent placental abruption. Obstet Gynecol 61:519, 1983 |
|
Edwards RZ, Rijhsinghani A: Dysfibrinogenemia and placental abruption. Obstet Gynecol 95:1043, 2000 |
|
Steegers-Theunissen RP, Boers GH, Blom HJ et al: Hyperhomocysteinaemia and recurrent spontaneous abortion or abruptio placentae. Lancet 339:1122, 1992 |
|
Van den Berg M, Franken DG, Boers GHJ et al: Combined vitamin B6 plus folic acid therapy in young patients with arteriosclerosis and hyperhomocysteinaemia. J Vasc Surg 20:933, 1994 |
|
Gebhardt GS, Scholtz CL, Hillermann R et al: Combined heterozygosity for methylenetetrahydrofolate reductase (MTHFR) mutations C677T and A1298C is associated with abruptio placentae but not with intrauterine growth restriction. Eur J Obstet Gynecol Reprod Biol 97:174, 2001 |
|
Goddijn-Wessel TAW, Wouters MGAJ, Molen EF et al: Hyperhomocysteinaemia: A risk factor for placental abruption or infarction. Eur J Obstet Gynecol Reprod Biol 66:23, 1996 |
|
DeVries JI, Dekker GA, Huijgens PC et al: Hyperhomocysteinaemia and protein S deficiency in complicated pregnancies. Br J Obstet Gynecol 104:1248, 1997 |
|
Ray JG, Laskin CA: Folic acid and homocysteine metabolic defects and the risk of placental abruption, preeclampsia and spontaneous pregnancy loss: A systematic review. Placenta 20:519, 1999 |
|
Owen EP, Human L, Carolissen AA et al: Hyperhomocysteinaemia: A risk factor for abruptio placentae. J Inherit Metab Dis 20:359, 1997 |
|
Eskes T: Clotting disorders and placental abruption: homocysteine-a new risk factor. Eur J Obstet Gynecol Reprod Biol 95:206, 2001 |
|
Wiener-Megnagi Z, Ben-Shlomo I, Goldberg Y et al: Resistance to activated protein C and the Leiden mutation: High prevalence in patients with abruptio placentae. Am J Obstet Gynecol 179:1565, 1998 |
|
Kupferminc MJ, Eldor A, Steinman N et al: Increased frequency of genetic thrombophilia in women with complications of pregnancy. N Engl J Med 340:9, 1999 |
|
Prochazka M, Lubusky M, Slavik L et al: Frequency of selected thrombophilias in women with placental abruption. Aust N Z J Obstet Gynaecol. 2007 Aug;47(4):297-301. |
|
Lakasing L, Poston L: Adverse pregnancy outcome in the antiphospholipid syndrome: Focus for future research. Lupus 6:681, 1997 |
|
Kupferminc MJ, Peri H, Zwang E et al: High prevalence of the prothrombin gene mutation in women with intrauterine growth retardation, abruptio placentae and second trimester loss. Acta Obstet Gynecol Scand 79:963, 2000 |
|
Naeye RL, Peters EC: Causes and consequences of premature rupture of fetal membranes. Lancet 1:192, 1980 |
|
Vintzileos AM, Campbell WA, Nochimson DJ et al: Degree of oligohydramnios and pregnancy outcome in patients with premature rupture of membranes. Obstet Gynecol 66:162, 1985 |
|
Gonen R, Hannah ME, Milligan JE: Does prolonged preterm premature rupture of the membranes predispose to abruptio placentae. ? Obstet Gynecol 74:347, 1989 |
|
Major CA, de Veciana M, Lewis DF et al Preterm premature rupture of membranes and abruptio placentae: Is there an association between these pregnancy complications. ? Am J Obstet Gynecol 172:672, 1995 |
|
Saftlas AF, Olson DR, Atrash HK et al: National trends in the incidence of abruptio placentae, 1979-1987. Obstet Gynecol 78:1081, 1991 |
|
Vintzileos AM, Campbell WA, Nochimson DJ et al: Preterm premature rupture of the membranes: A risk factor for the development of abruptio placentae. Am J Obstet Gynecol 156:1235, 1987 |
|
Nelson M, Stempel LE, Zuspan FP: Association of prolonged, preterm premature rupture of the membranes and abruptio placentae. J Reprod Med 31:249, 1986 |
|
Ananth CV, Savitz DA, Williams MA: Placental abruption: A meta-analysis of its incidence, and its association with hypertension and prolonged rupture of membranes. Obstet Gynecol 88:309, 1996 |
|
Ananth CV, Oyelese Y, Srinivas N et al: Preterm premature rupture of membranes, intrauterine infection, andoligohydramnios: risk factors for placental abruption. Obstet Gynecol. 2004 Jul;104(1):71-7. |
|
Hladky K, Yankowitz J, Hansen WF: Placental abruption. Obstet Gynecol Surv 57:299, 2002 |
|
Van Rijn M, Van der Schouw YT, Hagenaars AM et al Adverse obstetric outcome in low and high-risk pregnancies: Predictive value of maternal serum screening. Obstet Gynecol 94:929, 1999 |
|
Bartha JL, Comino-Delgado R, Arce RF: Maternal serum alpha-fetoprotein in placental abruption associated with preterm labor. Int J Gynaecol Obstet 56:231, 1997 |
|
Lydon-Rochelle M, Holt VL, Easterling TR et al: First-birth cesarean and placental abruption or previa at second birth(1). Obstet Gynecol. 2001 May;97(5 Pt 1):765-9. |
|
Getahun D, Oyelese Y, Salihu HM et al: Previous cesarean delivery and risks of placenta previa and placental abruption. Obstet Gynecol. 2006 Apr;107(4):771-8. |
|
Zugaib M, De Barros AC, Bittar RE et al: Abruptio placentae following snake bite. Am J Obstet Gynecol 151:754, 1985 |
|
Taylor RN, Green JR: Abruptio placentae following nipple stimulation. Am J Perinatol 4:94, 1987 |
|
Leung A, Kwok P, Chang A: Association between prostaglandin E2 and placental abruption. Br J Obstet Gynecol 94: 1001,-1987 |
|
Misra DP, Ananth CV: Risk factors for placental abruption in the first and second pregnancies: Heterogeneous etiologies. J Clin Epidemiol 52:453, 1999 |
|
Dommisse J, Tiltman AJ: Placental bed biopsies in placental abruption. Br J Obstet Gynecol 99:651, 1992 |
|
Salafia CM, Lopez-Zeno JA, Sherer DM et al: Histologic evidence of old intrauterine bleeding is more frequent in prematurity. Am J Obstet Gynecol 173:1065, 1995 |
|
Thompson D, Paterson WG, Smart GE et al: The renal lesion of toxemia and abruptio placentae studied by light and electron microscopy. J Obstet Gynaecol Br Commonw 79:311, 1972 |
|
Marilyn DJ, Caris SW, Schwarz SS: Placental abruption in preterm gestation. An association with chorioamnionitis Obstet Gynecol 74:88, 1989 |
|
Darby M, Caritis SN, Shen-Schwartz S: Placental abruption in the preterm gestation: An association with chorioamnionitis. Obstet Gynecol 74:88, 1989 |
|
Nath CA, Ananth CV, Smulian JC et al: Histologic evidence of inflammation and risk of placental abruption. Am J Obstet Gynecol. 2007 Sep;197(3):319.e1-6. |
|
Ramsey EM: Vascular adaptations of the uterus to pregnancy. Ann NY Acad Sci 75:726, 1956 |
|
Ananth CV, Vintzileos AM: Maternal-fetal conditions necessitating a medical intervention resulting in preterm birth. Am J Obstet Gynecol. 2006 Dec;195(6):1557-63. |
|
Ananth CV, Oyelese Y, Prasad V et al: Evidence of placental abruption as a chronic process: associations with vaginalbleeding early in pregnancy and placental lesions. Eur J Obstet Gynecol Reprod Biol. 2006 Sep-Oct;128(1-2):15-21. |
|
Fleming AD: Abruptio placentae. Crit Care Clin 7:865, 1991 |
|
Tikkanen M, Nuutila M, Hiilesmaa V et al: Clinical presentation and risk factors of placental abruption. Acta Obstet Gynecol Scand. 2006;85(6):700-5. |
|
Hurd WW, Miodovnik M, Hertzberg V et al: Selective management of abruptio placentae: A prospective study. Obstet Gynecol 61:467, 1983 |
|
Ito M, Kawasaki K, Matsui V et al: Fetal heart monitoring and ultrasound in the management of placental abruption. Int J Gynaecol Obstet 24:269, 1986 |
|
Usui R, Matsubara S, Ohkuchi A et al: Fetal heart rate pattern reflecting the severity of placental abruption. Arch Gynecol Obstet. 2008 Mar;277(3):249-53. |
|
Emery CL, Morway LF, Chung-Park M et al: The Kleihauer-Betke test: clinical utility, indication, and correlation in patients with placental abruption and cocaine use. Arch Pathol Lab Med 119:1032, 1995 |
|
Williams MA, Hickok DE, Zingheim RW et al: Maternal serum CA 125 levels in the diagnosis of abruptio placentae. Obstet Gynecol 82:808, 1993 |
|
Jaffe MH, Schoen WC, Silver TM et al: Sonography of abruptio placentae. AJR Am J Roentgenol 137:1049, 1981 |
|
Jouppila P, Kirkinen P: Problems associated with the ultrasonic diagnosis of abruptio placentae. Int J Gynaecol Obstet 20:5, 1982 |
|
Yiu-Chiu V, Chiu L: Sonographic features of placental complication in pregnancy. AJR Am J Roentgenol 138:879, 1982 |
|
Spirit BA, Kagan EH, Rozanski RM: Abruptio placentae: Sonographic and pathologic correlation. Am J Radiol 133:877, 1979 |
|
Sholl J: Abruptio placentae: Clinical management in non-acute cases. Am J Obstet Gynecol 156:40, 1987 |
|
Huang CY, Hwang SS, Chiang JH et al: Abruptio placentae: Analysis of 208 cases. J Formos Med Assoc 86:1215, 1987 |
|
Glantz C, Purnell L: Clinical utility of sonography in the diagnosis and treatment of placental abruption. J Ultrasound Med 21: 837, 2002 |
|
Yeo L, Vintzileos AM, Guzman ER et al: The sonographic diagnostic accuracy of abruptio placenta in patients with premature rupture of the membranes vs. intact membranes [abstract 588] Am J Obstet Gynecol 180:S166, 1999 |
|
Nyberg DA, Cyr DR, Mack LA et al: Sonographic spectrum of placental abruption. AJR Am J Roentgenol 148:161, 1987 |
|
Nyberg DA, Mack LA, Benedetti TJ et al: Placental abruption and placental hemorrhage: Correlation of sonographic findings with fetal outcome. Radiology 358:357, 1987 |
|
Ball RH, Ade CM, Schoenborn JA et al: The clinical significance of ultrasonographically detected subchorionic hemorrhage. Am J Obstet Gynecol 174:996, 1996 |
|
Yeo L, Vintzileos AM, Guzman ER et al: Correlation of sonographic signs of abruptio placenta with perinatal outcome in patients presenting with vaginal bleeding [abstract 587]. Am J Obstet Gynecol 180:S166, 1999 |
|
Elliott JP, Gilpin B, Strong TH et al: Chronic abruption-oligohydramnios sequence. J Reprod Med 43:418, 1998 |
|
Kay HH, Spritzer CE: Preliminary experience with magnetic resonance imaging in patients with third-trimester bleeding. Obstet Gynecol 78:424, 1991 |
|
Witlin AG, Sibai BM: Perinatal and maternal outcome following abruptio placentae. Hypertens Pregnancy 20:195, 2001 |
|
Wooldridge LL: On intravascular clotting. Proc R Soc Lon 40:134, 1886 |
|
Obata I: Eclampsia: An experimental study of sera and placenta extract. Tokyo Igakukai Zasshi 31: 1917 |
|
Page EN, Fulton ID, Glendenning MB: The cause of the blood coagulation defect following abruptio placentae. Am J Obstet Gynecol 61:1116, 1951 |
|
Pritchard JA, Brekken AL: Clinical and laboratory studies on severe abruptio placentae. Am J Obstet Gynecol 97:681, 1967 |
|
Creasy RK, Resnik R: Maternal-Fetal Medicine. pp 621-631, 4th ed.. Philadelphia, WB Saunders, 1999 |
|
Nolan TE, Smith RP, Devoe LD et al: A rapid test for abruptio placentae: Evaluation of a D-dimer latex agglutination slide test. Am J Obstet Gynecol 169:265, 1993 |
|
Sheehan HL: Post-partum necrosis of anterior pituitary. J Pathol Bacteriol 45:189, 1937 |
|
Rosen T, Schatz F, Kuczynski E et al: Thrombin-enhanced matrix metalloproteinase-1 expression: a mechanism leaking placental abruption with premature rupture of the membranes. J Matern Fetal Neonatal Med 11:11, 2002 |
|
Newton ER, Kennedy JL, Farid L: Obstetric diagnosis and perinatal mortality. Am J Perinatol 4:300, 1987 |
|
Sheiner E, Shoham-Vardi I, Hadar A et al: Incidence, obstetric risk factors and pregnancy outcome of preterm placental abruption: a retrospective analysis. J Matern Fetal Neonatal Med 11:34, 2002 |
|
Ananth CV, Berkowitz TS, Savitz DA et al: Placental abruption and adverse perinatal outcomes. JAMA 282:1646, 1999 |
|
Hibbard BM, Jeffcoate TNA: Abruptio placentae. Obstet Gynecol 27:155, 1966 |
|
Nath CA, Ananth CV, DeMarco C et al: Low birthweight in relation to placental abruption and maternal thrombophilia status. Am J Obstet Gynecol. 2008 Mar;198(3):293.e1-5. |
|
Chang YL, Chang SD, Cheng PJ: Perinatal outcome in patients with placental abruption with and without antepartum hemorrhage. Int J Gynaecol Obstet 75:193, 2001 |
|
Spinillo A, Fazzi E, Stronati M et al: Severity of abruptio placentae and neurodevelopmental outcome in low birth weight infants. Early Hum Dev 35:45, 1993 |
|
Rasmussen S, Irgens LM, Bergsjo P et al: The occurrence of placental abruption in Norway 1967–1991. Acta Obstet Gynecol Scand 75:222, 1996 |
|
Gibbs JM, Weindling AM: Neonatal intracranial lesions following placental abruption. Eur J Pediatr 153:195, 1994 |
|
Rivera Alsina ME, Saldana LR, Maklad N et al: The use of ultrasound in the expectant management of abruptio placentae. Am J Obstet Gynecol 146:924, 1983 |
|
Herbert WN, Stuart NN, Butler LS: Electronic fetal heart rate monitoring with intrauterine fetal demise. J Obstet Gynecol Neonatal Nurs 249, 1987 |
|
Maeder HP, Lippert TH: Misinterpretation of heart rate recordings in fetal death. Eur J Obstet Gynecol 6:167, 1972 |
|
Hammacher K: The monitoring of the human fetal heart. Int J Gynaecol Obstet 10:173, 1972 |
|
Kettel LM, Branch DW, Scott JR: Occult placental abruption after maternal trauma. Obstet Gynecol 71:449, 1988 |
|
Rothenberger D, Quattlebaum FW, Perry JF et al: Blunt maternal trauma: A review of 103 cases. J Trauma 18:173, 1978 |
|
Burchell HJ, Odendaal HJ, De Wet JI et al: Uterine contraction patterns in abruptio placentae. South Afr Med J 67:48, 1985 |
|
Heinonen PK, Kajan M, Saarikoski S: Cardiotocographic findings in abruptio placentae. Eur J Obstet Gynecol Biol 23:75, 1986 |
|
Morrow RJ, Ritchie JW: Uteroplacental and umbilical artery blood velocity waveforms in placental abruptio assessed by Doppler ultrasound: Case report. Br J Obstet Gynecol 95:723, 1988 |
|
Hoskins IA, Friedman DM, Frieden FJ et al: Relationship between antepartum cocaine abuse, abnormal umbilical artery Doppler velocimetry, and placental abruption. Obstet Gynecol 78:279, 1991 |
|
Malcus P, Lauriini R, Marsal K: Doppler blood flow changes and placental morphology in pregnancies with third trimester hemorrhage. Acta Obstet Gynecol 71:39, 1992 |
|
Rafla NM: The use of Doppler umbilical artery waveforms in placental abruption: A report of two cases. Eur J Obstet Gynecol Reprod Biol 38:167, 1990 |
|
Toivonen S, Heinonen S, Anttila M et al: Reproductive risk factors, Doppler findings, and outcome of affected births in placental abruption: A population-based analysis. Am J Perinatol 19:451, 2002 |
|
Pritchard JA, MacDonald PC: Williams Obstetrics. pp 495-496, New York, Appleton-Century-Crofts, 1980 |
|
Knab DR: Abruptio placentae: An assessment of the time and method of delivery. Obstet Gynecol 52:625, 1978 |
|
Baron F, Hill WC: Placenta previa, placenta abruptio. Clin Obstet Gynecol 41:527, 1998 |
|
Combs CA, Nyberg DA, Mack LA et al: Expectant management after sonographic diagnosis of placental abruption. Am J Perinatol 9:170, 1992 |
|
Towers CV, Pircon RA, Heppard M: Is tocolysis safe in the management of third-trimester bleeding? Am J Obstet Gynecol 180:1572, 1999 |
|
Kobayashi T, Terao T, Maki M et al: Activated protein C is effective for disseminated intravascular coagulation associated with placental abruption. Thromb Haemost 82:1363, 1999 |
|
Grimes DA, Steele AO, Hatcher RA: Rh immunoglobulin use with placenta previa and abruptio placentae. South Med J 76:743, 1983 |
|
McKay D: Intravascular coagulation: Acute and chronic, disseminated and local. Proc Inst Med Chic 29: 159, 1972 |