The Menopause
Authors
INTRODUCTION
The climacteric or perimenopausal period normally begins as early as 40 years of age with commencement of the regression of ovarian function. Depletion of primordial ovarian follicles results in diminution of estradiol levels leading to intermittent menstrual irregularities, vasomotor symptoms, and genital atrophy. As a result of the decrease in estradiol negative feedback and diminished levels of inhibin, there is increased secretion of folliclestimulating hormone (FSH). The elevated FSH levels accelerate follicular maturation and trigger early ovulation. Mean follicular phase and menstrual cycle length may be reduced before the menopause. At first, the luteal phase is of normal duration, but luteal dysfunction eventually may occur because of a fall in progesterone levels. Many anovulatory cycles may occur as well.4,5
The postmenopausal ovary secretes androgens but virtually no estrogen.6,7 Although the ovary may still contain some oocytes, the follicles are largely incapable of responding to gonadotropins and of synthesizing estradiol. Removal of postmenopausal ovaries often fails to change the levels of total circulating estrogen.7 The estrogen produced after the menopause is primarily from the peripheral conversion of adrenal androgens and occurs in the liver, kidney, brain, adrenal, and peripheral adipose tissue.8 Only small quantities of estrone and estradiol are secreted by the ovary.6,7,9,10 Mean serum levels of estrone after the menopause approximate 35 pg/ml.7,11,12,13 Almost all the estradiol that is produced comes from the peripheral conversion of estrone,14 causing the mean estradiol level to fall from 120 to 18 pg/ml (Table 1).15
TABLE 1. Typical Ranges of Circulating Hormonal Concentrations in Untreated Menopausal Women
Hormones | Concentrations |
Estradiol | <10–40 pg/ml |
Estrone | <10–50 pg/ml |
FSH | 30–240 mIU/ml |
LH | 30–220 mIU/ml |
Androstenedione | 600–1200 pg/ml |
Testosterone | 150–350 pg/ml |
Prolactin | 5–20 ng/ml |
FSH, follicle-stimulating hormone; LH, luteinizing hormone.
Because of the changes in estrogen production, the ratio of estradiol to estrone changes after the menopause, with the estrone level exceeding that of estradiol.9 The absolute levels of estrogen are influenced by weight, sex, and age. Obese women have a higher concentration of free estradiol because of decreased sex hormone-binding globulin and an increased rate of aromatization.6,16 Stress raises the estrogen level by increasing adrenal secretion, whereas liver disease and congestive heart disease raise serum estrogen by decreasing the metabolic clearance of androstenedione.
Gonadotropin levels greater than 30 mIU/ml are typically diagnostic of menopause, with the ratio of FSH to luteinizing hormone (LH) being greater than 1.17 After oophorectomy in a woman of reproductive age, there is a variable rise in gonadotropins. It may take more than a month for final menopausal levels to be reached.18 Eventually, there is a 10- to 20-fold rise in FSH, with a threefold increase in LH. In physiologic menopause, it may take 1 to 3 years for these levels to be attained.11 In castrated and menopausal women, however, gonadotropin levels rise quickly in the absence of ovarian estrogen secretion. As in other physiologic conditions, in the postmenopausal woman, the secretion of gonadotropins is pulsatile, with FSH pulses being more pronounced and occurring at 60- to 90-minute intervals.19 Some data suggest that gonadotropin levels may decrease somewhat in the very elderly.
Androgens continue to be produced by the ovarian stromal and hilus cells in response to the increased levels of circulating LH. There is a 25% increase in testosterone secretion by the postmenopausal ovary; however, circulating levels of testosterone decrease to slightly less, approximately 250 pg/ml, than those of premenopausal women.11,13,20,21 This reduction has been attributed to a significant fall in the conversion of androstenedione to testosterone after the menopause. In premenopausal women, 50% of androstenedione is secreted by the adrenal gland and 50% by the ovary; 14% of androstenedione is converted to testosterone to account for 50% of circulating testosterone. After menopause, only 20% of androstenedione is secreted by the ovary, and the percentage of androstenedione converted to estrone rises from approximately 1.3% to 2.8%. Circulating concentrations of androstenedione are reduced after menopause from 1500 pg/ml to approximately 800 to 900 pg/ml.11,13,20,21 The levels of androstenedione in postmenopausal women are similar to those of young surgically castrated women, but the level of testosterone in intact postmenopausal women is twice that of oophorectomized younger women.20
Although the total levels of androgen drop with menopause, the cumulative effect is an increase in androgenicity because of the significant fall in estrogen and the diminished levels of sex hormone-binding globulin. It is this increase in androgenicity that is the cause of increased facial hair growth and scalp hair loss in some postmenopausal women.
SIGNS AND SYMPTOMS OF MENOPAUSE
The hypoestrogenic state seen at menopause is manifested in many women by signs and symptoms of hormonal deficiency in tissues containing estrogen receptors, including the ovary, endometrium, vaginal epithelium, urethra, hypothalamus, and skin. The most common complaints are vasomotor disturbances characterized by hot flushes, genital atrophy, and psychologic symptoms. The decline in estrogen also causes an increased risk of osteoporosis.
Vasomotor Flushes
Vasomotor instability appears to arise not from a lack of estrogen but rather from its withdrawal. Estrogen-deficient patients with gonadal dysgenesis fail to develop hot flushes unless given estrogen replacement therapy (ERT) that is subsequently withdrawn.22 Castrated women with androgen insensitivity experience vasomotor symptoms after the discontinuation of estrogen. Similarly, premenopausal women treated with the antiestrogen clomiphene and postpartum women with very low estrogen levels often complain of hot flushes.
Hot flushes or flashes are experienced by 75% to 85% of all women undergoing natural menopause or who have undergone bilateral oophorectomies.23,24,25,26 The sudden drop in estrogen seen in oophorectomized women apparently makes them more prone to vasomotor instability. Hot flushes may begin in the perimenopausal period months or years before menopause, even in the presence of regular menstrual cycles.24 These women can be successfully treated with low-dose estrogen. More than four of five women experience hot flushes for more than 1 year, and 45% of women continue to have hot flushes for 5 to 10 years.25,26,27 Although one study showed a relationship between circulating estrogen and the occurrence of hot flushes,28 most investigators have not found such a correlation.29,30
The duration of the flush varies from a few seconds to minutes and rarely may last up to an hour. The flushes may be infrequent or may recur as often as every 30 minutes. Flushes appear to be more severe at times of stress and more frequent and severe at night, when they are called night sweats. Simultaneous electroencephalographic recordings show that women awaken before the detection of the physiologic changes seen with each flush.31 Night sweats can lead to significant sleep deprivation. Menopausal women not on replacement hormones have decreased rapid eye movement sleep and increased sleep latency compared with those on estrogen.
There is a subjective awareness of an impending hot flush, with an aura that may be perceived as a headache accompanied by heart palpitations occurring up to 4 minutes before the actual flush. The subjective sensation of the flush is followed by a change in skin conductance. There is then a rise in finger temperature that reflects cutaneous vasodilation (Fig. 1).32,33,34 The pulse rate increases an average of nine beats per minute, and a rapid rise is seen in blood flow to the hand before the flush35 (Table 2).
TABLE 2. Documented Physiologic Changes Known to Accompany Hot Flashes
Decrease in skin resistance, increased conductance
Rise in finger temperature
Fall in core body temperature
Increase in pulse rate
Increase in blood flow to hand
Vasodilation along cervical sympathetic pathway
Hormonal changes: increase in LH, ACTH, cortisol, dehydroepiandrosterone, androstenedione
Interruption of REM sleep
ACTH, corticotropin; LH, luteinizing hormone; REM, rapid eye movement.
|
The actual hot flush is subjectively characterized by a sensation of warmth and heat that starts in the chest and spreads upward over the neck and head. This sensation is accompanied by regional vasodilation, which causes flushing of the neck and face and produces body heat loss. The core temperature falls an average of 0.2°C, resulting in perspiration and chills.36 Other vasomotor symptoms may occur concurrently, including nausea, dizziness, headache, palpitations, and diaphoresis.
Endocrine studies have shown that hot flushes occur in menopausal women together with pulses of LH (Fig. 2). Although not every LH pulse is accompanied by a hot flush, virtually every hot flush occurs simultaneously with the onset of a pulse of LH.37 Circulating estrone and estradiol levels do not vary before or after the flush; however, the adrenal steroids cortisol, dehydroepiandrosterone, and androstenedione increase significantly at the time of the flush. Corticotropin (ACTH) and cortisone also increase in a pulsatile fashion with the temperature changes.38
|
The pathophysiology of the hot flush is not fully understood.39 The withdrawal of estrogen seems to alter the hypothalamic thermoregulatory system such that the “set point” lowers, the patient vasodilates to meet this temperature setting, and changes in neural activity alter hormonal secretions. Although LH pulses occur concurrently with flushes,37,38,40 LH does not initiate the hot flush, because patients with pituitary insufficiency and those with hypophysectomies can still have hot flushes.41,42 Injections of gonadotropins do not induce flushes, and administration of a gonadotropin-releasing hormone (GnRH) agonist inhibit pulsatile LH release and precipitate hot flushes.43,44 The hot flush has been associated with GnRH release, because the GnRH neurons are located near the preoptic nucleus of the hypothalamus, the nucleus responsible for temperature regulation. However, GnRH is not the initiating factor, because women with GnRH deficiency can still have hot flushes.
An alteration in the autonomic nervous system has been implicated because neuronal processes from the anterior hypothalamus innervate the superior cervical ganglion, accounting for the distribution of the flush, which spreads along the cervical sympathetic pathway. Norepinephrine, an α-adrenergic agent, releases GnRH and affects thermoregulatory function.45 The role of catecholamines is further supported by the fact that clonidine, an α2-adrenergic agonist, decreases the frequency and intensity of hot flushes, whereas yohimbine, an α2-adrenergic antagonist, provokes hot flushes.46,47 Attempts to measure levels of epinephrine and norepinephrine have produced conflicting results.37,48,49 Central adrenergic activation could cause the release of vasoactive substances such as prostaglandin or histamine. Catecholamines and prostaglandin E have been linked to the release of GnRH50,51 and to temperature regulation.52 These data led to the hypothesis that estrogen deficiency in the central nervous system induces changes in catecholamines and prostaglandins that affect neurons in the locus ceruleus, causing the regional vasodilation associated with the hot flush.22
It has also been suggested that a decrease in gonadal steroids may cause a fall in endogenous opioid activity within the hypothalamus, inducing the symptoms of menopause, which are similar to those of opiate withdrawal.53 This theory is based on several findings. Ovariectomy in the monkey causes a significant decrease in hypothalamic β-endorphin levels.54 Estradiol and progesterone increase β-endorphin secretion.55 Naloxone stimulates the release of LH in certain situations, suggesting inhibition of gonadotropin secretion by opioids.55 When morphine-dependent rats are given clonidine in doses of 10 to 50 μg, there is a modest increase in tail skin temperature, which is blocked if naloxone is also given.45
ERT has been shown clinically to improve vasomotor symptoms and totally eradicates them in most women.56,57 If a patient is unable to take estrogen, progestins have been shown to be effective in reducing hot flushes. Oral medroxyprogesterone acetate (MPA) (20 to 40 mg/day),58 depo-MPA (150 mg given intramuscularly every 3 months),59 or megestrol acetate (40 to 80 mg/day) decreases patient distress. Other agents suggested for the treatment of vasomotor instability include clonidine, naloxone, methyldopa, and a mixture of phenobarbital, ergotamine, and belladonna (Bellergal). The most carefully studied of these other agents is clonidine.46 Large doses of clonidine of up to 400 μg daily reduce the number of objectively recorded hot flushes; however, side effects have caused 40% of women to discontinue using clonidine in controlled studies.60 Moreover, at maximal tolerated dosages, the mean rate of hot flush occurrence decreases by less than one half.
Urogenital Changes
The decline in estrogen in the menopausal woman leads to a number of anatomic changes in the genitourinary tract and elsewhere (Table 3). The uterus becomes smaller and firmer, with a decrease in its total weight from 120 g to less than 50 g. There is also a decrease in myometrial thickness and vascularity. Most commonly, the endometrium becomes atrophic, the so-called senile endometrium; 5% of postmenopausal women develop a weakly proliferative endometrium, and a smaller percentage develop cystic hyperplasia or adenomatous hyperplasia, with even fewer developing neoplasia.
TABLE 3. Anatomic Changes of Menopause
Smaller uterus
Smaller cervix
Adolescent cervix: corpus ratio
Inner migration of squamocolumnar junction of cervix
Contraction of cervical glands
Smaller labia
Decreased Bartholin gland secretion
Smaller clitoris
Thinning of hair on mons pubis and labial folds
Shorter, more narrow vagina
Left shift in maturation index
Flaccid breasts
Shortened urethra
Thinning of skin
Loss of bone density
Increased facial hair
Thinning of scalp hair
Change in fat to muscle ratio
The cervix also decreases in size, although to a lesser degree than the corpus, resulting in a ratio similar to that seen in adolescence. There is an inner migration of the squamocolumnar junction, making the diagnosis of cervical cancer more difficult. The cervical glands contract, resulting in a decrease in cervical mucus.
The postmenopausal vulva loses subcutaneous fat and elastic tissue, which results in a more narrow introitus. The labia majora flatten and wrinkle and shrink more than the labia minora, creating relative proportions similar to those of the prepubertal state. The clitoris decreases in size. The Bartholin glands produce less secretion, causing vaginal dryness and pruritus, and the hair on the mons pubis and labial folds becomes thinner and more coarse. Although the vulva has estrogen receptors, no change is observed after ERT. It is unknown whether estrogen, if instituted at the time of menopause, can prevent these changes.
Postmenopausally, the vagina becomes shorter and more narrow because of an increase in submucosal connective tissue. The rugae become less prominent. The fall in estrogen causes the maturation index to shift to the left, with a predominance of parabasal and intermediate cells. Eventually, the smear contains only small parabasal cells. Scant vaginal secretion and thin vaginal epithelium result in dryness and friability. The glycogen content of the vaginal epithelium decreases, as does the acidity of the secretions. Consequently, there is inhibition of lactobacilli with increased growth of other flora, increasing the susceptibility to irritation, trauma, and infection.
The glandular tissue of the breast atrophies, and Cooper's ligaments become less elastic, leading to flaccid breasts consisting primarily of fatty tissue. The nipples become smaller and may lose their erectile properties. The alveoli disappear, and the ducts decrease in size. In 10% of women, the breasts enlarge during the climacteric period, probably because of early unopposed estrogen and increased pituitary stimulation. They may remain enlarged and tender for some years after menopause.
The urethra and the base of the bladder are derived from müllerian tissue and are estrogen sensitive. Epithelial changes in the lining of the urethra and trigone of the bladder after the menopause are similar to those of the vagina and may result in atrophic cystitis, atrophic urethritis, urethral caruncles, urethral shortening, and stress incontinence. The urethral syndrome that results from the loss of bladder sphincter tone is characterized by recurrent bacterial urethritis with dysuria, frequency, urgency, nocturia, and postvoid dribbling. Estrogen replacement is helpful in treating all these symptoms. Between 10% and 15% of postmenopausal women older than 60 experience recurrent urinary tract infections. In a study of 93 women with this condition, a significant reduction in incidence occurred with the use of vaginal estriol cream.61 Pelvic relaxation, including cystocele, rectocele, or uterine prolapse, may develop in part because of the atrophic changes of the vagina and surrounding musculature. Estrogen receptors are not found in the area of the pelvic floor, which is composed of striated muscle; therefore, estrogen replacement is of no benefit for these conditions.
Hypoestrogenism accelerates aging of the skin. Estrogen can reverse some of these changes and has been shown to cause thickening of the epidermis.62 Estrogen receptors are present in the skin, and estrogen may be involved in collagen metabolism. After menopause, the epidermis thins, there is loss of epidermal ridges, the dermal papillae become less prominent, and the collagen and elastic tissue are reduced in the dermis. Other skin changes, including redistribution of fat deposits, loss of muscle tone, and loss of elastic tissue, are not thought to result from estrogen deprivation. There also are fewer hair follicles on the scalp and extremities and decreased production from sebaceous glands. All these changes lead to thin, dry skin with the development of creases and lines, frequent itching, and a tendency toward balding. Because of the state of relative hyperandrogenism occurring with menopause, increased facial hair and loss of scalp hair are common.
Bone Changes and Osteoporosis
Postmenopausal osteoporosis was first described in 1940.63 It is characterized by a progressive loss of bone mass without any change in the chemical composition of bone. The bone loss results in changes in the microscopic architecture of the bone that lead to an increase in fracture rate. Risk factors for osteoporosis include low bone mass at the onset of menopause, slender build, white or Asian race, premature ovarian failure, surgical menopause, a positive family history for osteoporosis, glucocorticoid therapy, and nulliparity (Table 4). Avoidable factors that predispose to osteoporosis include lack of physical exercise, insufficient calcium intake, cigarette smoking, excessive caffeine or alcohol intake, and estrogen deficiency. Premenopausal women with hyperprolactinemia or hypoestrogenic forms of amenorrhea are at increased risk of excessive bone loss because of the associated estrogen deficiency.64 Anorexia nervosa is associated with significant osteoporosis in young women.65 Factors that seem to be protective against osteoporosis include obesity, multiparity, muscular habitus, black race, and possibly the use of oral contraceptive agents for more than 1 year.
TABLE 4. Common Risk and Protective Factors for Osteoporosis
Unavoidable Risk Factors | Avoidable Risk Factors | Protective Factors |
Genetic predisposition | Lack of physical exercise | Obesity |
Low bone mass | Insufficient calcium intake | Multiparity |
Slender build | Smoking | Muscular habitus |
White or Asian race | Excessive alcohol intake | Black race |
Premature ovarian failure | Excessive caffeine intake | Prolonged oral contraceptive use |
Surgical menopause | Estrogen deficiency | Hormone replacement therapy |
Glucocorticoid therapy | Anorexia nervosa |
|
Nulliparity | Excessive exercise |
|
| Excessive thyroid re placement |
|
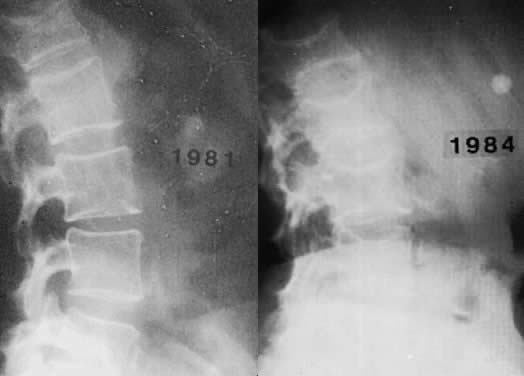
Osteoporosis is an insidious disease and often goes undetected until a painful compression fracture occurs. Only in hypoestrogenic female athletes and dancers may stress fractures be the first sign. Back pain is frequently the first complaint associated with osteoporosis; at first presentation, radiologic changes are usually not evident. A minimum of 25% to 30% of bone mineral content must be lost for osteoporosis to be diagnosed by routine radiographs (Fig. 3). Sudden severe pain may indicate vertebral collapse. The principal complications of osteoporosis include distal forearm fractures, vertebral compression fractures, and hip fractures. Distal forearm fractures (i.e. Colles' fractures) are the first to increase, with a 10-fold rise occurring in Caucasian women as they age from 35 to 60.
|
Spinal compression fractures, the most frequently occurring of the osteoporotic fractures, may cause pain, loss of height, and postural deformities. Such fractures are 10 times more common in white women than in men, occurring in 25% of Caucasian women over the age of 60. The average postmenopausal woman shrinks approximately 6.35 cm. Some loss of height is secondary to narrowing of the disc space. Small vertebral fractures are responsible for anterior collapse of the vertebral bodies, leading to dorsal kyphosis (i.e. dowager's hump).
Osteoporotic fractures of the femur occur later in life, usually at age 70 to 75. The incidence of hip fractures increases from 0.3 per 1000 to 20 per 1000 from age 45 to 85, with 20% to 25% of all women sustaining such a fracture by age 90. In 80% of the cases, osteoporosis is the cause. Fifteen percent of these women die within a 3-month period because of complications of the fracture, including pulmonary edema, myocardial infarction, and pulmonary embolism.66 Another 25% of these women suffer significant morbidity. Taking into account the significant morbidity, the direct and indirect costs of osteoporosis were estimated for 1995 to have been 13.8 billion dollars in the United States.67
Cortical bone predominates in the shaft of long bones, whereas trabecular bone is found primarily in the vertebrae, pelvis, and other flat bones, as well as the ends of long bones. Trabecular bone is more sensitive to factors that affect remodeling because it is metabolically more active than cortical bone. Vertebral fractures, Colles' fractures of the distal arm, and increased loss of teeth are seen with postmenopausal osteoporosis because the vertebral body, ultradistal radius, and mandible contain large amounts of trabecular bone. Trabecular bone loss begins at age 30 to 35, with a linear decrease of 1.2% per year. Although one series reported a similar rate of loss in postmenopausal and premenopausal women,68 most studies have shown a significant increase in bone loss after menopause. One study reported a 12% loss of density in the lumbar vertebrae 2 years after surgical oophorectomy.69 This accelerated phase of bone loss appeared to result from an increased rate of bone resorption relative to bone formation.70,71 This phase is more easily discernible in oophorectomized women, who have an abrupt loss of estrogen, than in women undergoing physiologic menopause, who have a gradual decline in estrogen levels.
The loss of bone mass correlates with the duration of estrogen deficiency. When women of a mean age of 50 who had been castrated 20 years before were compared with women of a mean age of 70 who had undergone menopause 20 years earlier, the bone mass was similar in both groups, with a 15% to 28% loss of radial bone.72 The actual estrogen levels, the metabolic clearance rates, and the rates of conversion of androgen to estrogen appear to be of no value in predicting which women will have a more rapid rate of bone loss.
Cortical bone loss begins at approximately age 40, at which time there is a slow rate of loss of 0.3% to 0.5% per year until menopause, when the rate increases to 2% to 3% per year. This rate continues for 8 to 10 years, at which point the slow loss rate is resumed.73,74,75 Consequently, there is a much greater loss of trabecular than cortical bone.
The belief that estrogen deficiency plays a major role in bone loss is strongly supported by the high incidence of osteoporosis seen in untreated oophorectomized women and women with gonadal dysgenesis. The rapid bone loss seen in untreated women is prevented with the use of estrogen replacement.76 Increased urinary excretion of calcium and hydroxyproline is associated with estrogen deficiency, presumably because of an increase in bone resorption (Table 5).77 ERT reduces the rate of excretion of these substances to the range observed in premenopausal women.
TABLE 5. Effects of Estrogen Decline on Bone Metabolism
Acceleration of bone loss
Decreased secretion of parathyroid hormone
Increased secretion of calcitonin
Decreased production of 1,25-dihydroxycholecalciferol
Decreased calcium absorption
Increased urinary excretion of calcium and hydroxyproline
Parathyroid hormone (PTH) causes an increase in serum calcium by increasing bone resorption, increasing tubal reabsorption of calcium in the kidney, and producing the enzyme 1α-hydroxylase, which is needed to make the active form of vitamin D necessary for calcium absorption from the gut. Premenopausally, estrogen is thought to block the action of PTH on bone resorption, possibly by increasing calcitonin levels. After menopause, estrogen levels fall. It is believed that the actions of PTH are then less inhibited, leading to an acceleration of bone loss. There is decreased secretion of PTH, increased secretion of calcitonin, and impaired 1α-hydroxylase activity, causing a decrease in the production of 1,25(OH)2 vitamin D and diminished calcium absorption from the gastrointestinal tract.
Estrogen receptors have been identified in osteoblastic cells in tissue culture.78,79 Although added estrogen increases secretion of alkaline phosphatase and α1-procollagen by such cells in vitro, it is not clear whether this is the mechanism by which estrogen affects bone loss. This is especially true in view of the diverse effects of estrogens on metabolic factors that can affect bone. Progesterone receptors are present in bone as well.80
Only 20% of castrated women and 30% of women undergoing natural menopause lose sufficient bone mass to result in pathologic fractures. It is difficult to predict which women are at risk for osteoporosis. A variety of radiologic methods have been used to assess bone mineralization, including radiogrammetry, linear photon absorptiometry, dual photon absorptiometry, dual energy x-ray absorptiometry, computed tomography, quantitative computed tomography, neutron activation analysis, and ultrasound. These tests are costly and sometimes inaccurate in the presence of arthritis, scoliosis, and compression fractures. The dual energy x-ray absorptiometer claims accuracy of 3% to 6% and precision of 0.5% to 1.2% while having the advantage of very low radiation exposure (1 to 3 mrem). The instrument can evaluate lumbar spine, hip, and wrist, as well as total body fat and calcium content. The World Health Organization has proposed guidelines for the diagnosis of osteoporosis when using bone mineral density testing (Table 6). Less expensive screening devices are being investigated.
TABLE 6. World Health Organization Criteria for Diagnosis of Osteoporosis
Category | T Score* |
Normal | Above -1.0 STD |
Osteopenia | -1.0 to -2.5 STD |
Osteoporosis | Below -2.5 STD |
*The T score represents the number of standard deviations (STD) from the peak, young, healthy bone mineral density of the reference group.
The diagnosis of osteoporosis is one of exclusion. The radiologic changes are late manifestations. There are usually only minimal alterations in laboratory values. Serum calcium levels are typically normal; phosphorus concentrations may be slightly low, normal, or slightly elevated; serum PTH and alkaline phosphatase levels are normal; and urinary excretion of calcium and hydroxyproline is usually increased. The ratio of urinary calcium to creatinine is elevated.81
Drugs for osteoporosis can be divided into two categories: prevention and treatment (Table 7). Estrogen, saloxifene, and alendronate have been approved by the U.S. Food and Drug Administration (FDA) for prevention and treatment. The relation between lack of estrogen and osteoporosis was described 50 years ago by Albright.63 ERT has been found to increase calcium absorption and decrease bone resorption.82
TABLE 7. FDA Approved Therapy for Osteoporosis
Indication | Therapy |
Prevention and treatment | Raloxifene |
Treatment only | Calcitonin |
Prevention and treatment | Hormone replacement therapy |
Prevention and treatment | Alendronate |
Estrogen does not appear to stimulate osteoblastic formation of new bone directly but may have a positive effect through insulin-like growth factor, transforming growth factor, and prostaglandins.83,84,85 Estrogen prevents bone mineral loss if begun within 2 months of surgical castration of premenopausal women or before physiologic menopause.76,86 If therapy is delayed 3 to 6 years after castration, there is still a response to estrogen therapy with an increase in bone density, which seems to be maintained for at least a 5-year period (Fig. 4).86 If estrogen therapy is stopped, bone loss resumes, with bone mineral content rapidly declining to the low levels of nontreated women. It may be necessary to continue ERT indefinitely to maintain the benefit. However, women who do not start ERT until age 60 may fare almost as well as the women who initiate ERT at menopause, provided they continue it long term.87,88 Estrogen replacement also decreases the incidence of fractures of the radius and hip.89,90,91 In one study, women taking exogenous estrogen had less than one half of the fractures of the placebo group, with the most apparent decline seen after 5 or more years of therapy.90 Estrogen use was found to protect against hip fractures in the subsequent 2 years in women younger than 65 and in those 65 to 74 years old.92 Various doses of the different estrogen preparations have been shown to be protective of bone mineral density (Table 8). Many of the bone density studies have been controlled, randomized trials. Fracture data, however, have been drawn primarily from observational studies.
TABLE 8. Doses of Estrogen Preparations that Prevent Bone Loss
Estrogen | Dose |
Conjugated estrogens | 0.3 mg |
Oral estradiol-17β | 0.5 mg |
Transdermal estradiol-17β | 0.025 mg |
Esterified estrogens | 0.3 mg |
|
The bisphosphonate alendronate has been approved by the FDA at a dose of 5 mg/day for prevention and 10 mg/day for treatment. An increase of approximately 9% at the spine and 7% at the hip was reported in the treatment group over a period of 3 years.93 Fracture data indicate an approximately 50% reduction in fractures of the spine and hip.94 Very few side effects are reported with this medication; however, an uncommon but serious risk of esophageal or gastric ulceration with potential hemorrhage has been reported. It is thought that strict adherence to dosing guidelines can reduce the incidence of this side effect. Patients must be willing and able to take the medication first thing in the morning on an empty stomach with a full glass of water. They need to remain upright sitting or standing and not consume any other food or beverage for a full 30 minutes. Patients with preexisting esophageal problems or significant hiatal hernias may not be good candidates for this medication. Other bisphosphonates are under investigation. As a class, they have very low absorption rates—hence the specific dosing instructions. In general, they have a very short serum half-life and a very long half-life (years) of adsorption to hydroxyapatite in the bone. Long-term effects on bone metabolism remain to be determined.
Nasal spray calcitonin has been approved by the FDA for the treatment of osteoporosis. It is recommended as a treatment option for the woman with osteoporosis who is more than 5 years past menopause and not using ERT. Estrogen has been shown to stimulate the release of calcitonin,95 and women with postmenopausal osteoporosis have been found to have diminished calcitonin levels.96 With use of a calcium clamp, calcitonin release was found to be blunted in women with osteoporosis compared with age-matched women without osteoporosis.97 Other techniques, however, have shown that calcium sometimes stimulates calcitonin release in patients with osteoporosis.98 Osteoporosis may or may not be associated with an alteration in calcitonin. Nevertheless, calcitonin has been shown to be effective in a dose-related fashion in suppressing bone loss.99,100 When calcitonin was given with calcium, a slight gain in bone mass was observed over 2 years, and the fracture rate was reduced by two thirds.101 Exercise may release calcitonin, explaining the positive effect of exercise on bone. Calcitonin acts to inhibit bone resorption by reducing the activity and the number of osteoclasts.102 Calcitonin results in increased levels of circulating β-endorphins, which may explain the analgesic effect reported by patients with osteoporosis treated with calcitonin. Calcitonin may decrease the bone pain associated with osteoporosis. Dosing for the nasal spray calcitonin is 200 units or one spray per nostril per day. The patient should alternate nostrils each day. An earlier version of calcitonin can be administered subcutaneously in doses ranging from 50 units every other day to 100 units daily.
Antibodies to calcitonin may develop and impede its usefulness. Several studies suggest that calcitonin may lose effectiveness after a period of time. Investigation is under way to determine if intermittent administration of the drug eliminates the development of resistance. Human calcitonin is less immunogenic than the salmon calcitonin. Anti-salmon calcitonin antibodies do not bind to human calcitonin in vitro. Patients with Paget's disease who have developed a resistance to salmon calcitonin respond favorably to treatment with human calcitonin,103 and this may prove to be a promising therapy for osteoporosis.
Raloxifene was approved by the FDA for the prevention and treatment of osteoporosis. Raloxifene is a benzothiophene and belongs to a class of drugs designated as selective estrogen receptor modulators (SERMs). Two other drugs in this category are clomiphene and tamoxifen, both triphenylethelenes. These drugs have estrogen agonist effects at some end-organ sites and estrogen antagonist effects at other sites and were previously known as mixed estrogen agonist-antagonists. Tamoxifen, for example, has antiestrogenic effects at the breast and reduces breast cancer recurrence for at least 5 years of treatment. It has mildly estrogenic effects on bone, lipids, and the uterus. It is not recommended for use for longer than 5 years because any protective effect on the recurrence rate for breast therapy appears lost after this time.104 Decreased bone loss has been observed in postmenopausal women using tamoxifen as treatment for breast cancer.105 There have also been reports of an increased incidence of cancer of the uterus in women using this drug.106,107
Raloxifene has a slightly different profile. It has mildly estrogenic effects on the bone and lipid profile with no observable effect on the breast or uterus. Unlike oral estrogens, raloxifene does not increase triglycerides. It also has no apparent benefit on the symptoms of hot flushes and vaginal dryness and may increase these symptoms in some women. In a 2-year trial, raloxifene produced a 1% to 2% increase in bone mineral density at the spine and hip compared with baseline and a 2.0% to 2.4% increase compared with the placebo group.108 Side effects include a 6% incidence of leg cramps and a threefold increase in venous thromboembolic events (VTEs), an increase similar to that reported with ERT. A history of VTEs is a contraindication to using raloxifene.
Sodium fluoride has been used for many years in the treatment of osteoporosis. The drug has many proponents and opponents. It appears to increase bone density substantially;109 however, it has lost favor since the publication of data indicating marked improvement in bone density with no improvement in fracture rate110 in women being treated with fluoride. A high frequency of side effects can be encountered with use of fluoride, including gastrointestinal problems, anemia, and joint and tendon inflammation. A slow-release fluoride formulation under investigation may provide better fracture protection with fewer side effects, but at present it is advisable to limit the use of fluoride to research settings until better data are available.
Most postmenopausal and castrated women are in negative calcium balance because of insufficient calcium intake. Those not on estrogen require approximately 1.5 g per day to remain in balance, whereas those on estrogen require 1 g per day.111 However, calcium supplementation alone does not seem effective in preventing osteoporosis. When high-dose calcium was given to menopausal women, it was no more effective in preventing trabecular bone loss than the average daily intake of 500 to 600 mg of calcium. Calcium does, however, seem to suppress cortical bone loss112,113,114 and reduce the risk of developing osteoporosis-related fractures.115 Although calcium supplementation does not appear to arrest trabecular bone loss in the early postmenopausal phase, it may have a more positive effect in the elderly. Women with a mean age of 84 who were given calcium and vitamin D supplements were found to have 43% fewer hip fractures.116 Other studies have reported a beneficial effect of calcium on bone loss in the older postmenopausal woman.117,118 Reports have indicated that there may be more vitamin D deficiency among the elderly than was suspected. Replacing vitamin D and calcium in the elderly can have significant benefits.116,117,118
Because there is no cure for osteoporosis, prevention of accelerated bone loss is of the greatest value. Adequate dietary intake of calcium and sufficient exercise should be encouraged throughout life. Avoidable risk factors for osteoporosis should be addressed (Table 4), and ERT therapy should be considered for those women who are eligible and deemed to be at risk for osteoporosis.
Cardiovascular and Lipid Changes
The hypoestrogenic state that occurs after menopause may be a significant factor in the development of ischemic heart disease. Premenopausal females are relatively protected against atherosclerosis and coronary heart disease compared with males the same age. Women rarely suffer heart attacks until after the menopause, when the risk of cardiovascular disease approximates that of men by age 65.119 This sex difference seems to be apparent only in affluent populations. Some investigators feel the decrease in the male to female ratio of death rates results solely from a decrease in male mortality with age. This hypothesis is supported by a study that showed a linear increase in the incidence of coronary heart disease in women between the ages of 30 and 90, with no apparent change in rate at menopause.120 However, an increase in the incidence of heart disease has been reported after castration in young women,121,122,123 with autopsy studies showing the presence of more coronary disease than in age-matched controls.124 A large, prospective study found bilateral oophorectomy but not natural menopause to increase the risk of coronary heart disease.125 This increase seemed to be prevented by ERT. In contrast, other studies have found no difference in the incidence of coronary disease in women with and without oophorectomy.126 Women with premature ovarian failure have also been shown to have an increased incidence of coronary heart disease 10 to 20 years after the cessation of menstruation, with significantly higher cholesterol and triglyceride levels than age-matched women who underwent physiologic menopause.127
Smokers have an earlier natural menopause by 1 to 2 years. When the risk factors of smoking and age were considered, the increased risk seemed to affect only women castrated and those not on ERT.128 Although hypertension is a significant factor in premature development of coronary disease, it presumably plays no role in normal women because no change in diastolic or systolic blood pressure is found with menopause.129
Cholesterol levels increase with age in men and women. Values greater than 250 ng/ml correlate with an increased risk of heart disease. However, after age 50, this association is not as strong. Serum cholesterol levels rise after natural or surgical menopause to values seen in men. It is unknown whether this change results from estrogen depletion. When castrated women were treated with 50 μg of ethinyl estradiol or 1.25 mg of conjugated estrogens daily, no change was seen in their cholesterol levels,130 but when 2.5 mg of conjugated estrogen was administered, cholesterol levels fell.131
Individuals with high low-density lipoprotein (LDL) cholesterol and low high-density lipoprotein (HDL) cholesterol are at increased risk for coronary heart disease. Elevated levels of HDL are found in people who exercise and those at low risk for atherosclerotic heart disease. At the time of menopause, there is a shift in the lipid pattern to one more similar to the pattern found in men, with increases in phospholipids, α-lipoproteins, and triglycerides.132 Menopause seems to have only a slight effect on HDL cholesterol levels. Although estrogen replacement cannot totally reverse this pattern, it does decrease LDL cholesterol concentrations, and raise HDL cholesterol concentrations.133 Natural estrogen increases the HDL2 and HDL3 fractions.134
The beneficial effect of oral estrogen administration on the lipid profile has been attributed to its first passage through the liver, and it is thought to be more beneficial in this regard than percutaneous application. However, percutaneous administration has been shown to produce similar changes of a lower magnitude, but a longer time is required to see this beneficial effect.135
Estrogen use in postmenopausal women has been reported to protect against coronary heart disease.91,136 When mortality rates from ischemic heart disease in postmenopausal women on estrogen were compared with those in living and deceased women not on estrogen, estrogen and excessive alcohol use were shown to decrease the chance of dying, whereas diabetes, hypertension, and smoking increased the risk of dying. Even women who smoked and took estrogen had decreased mortality.137 When mortality rates from all causes were evaluated in age-adjusted women, those on ERT had significantly lower rates than nonusers.138
There are studies that refute the reported beneficial effects of estrogen on coronary heart disease.139,140,141 In one study of incident acute myocardial infarctions occurring in a large managed care program, there was no statistically significant reduction in relative risk of myocardial infarction among current users of ERT.141 No definitive conclusions can be made regarding the beneficial or detrimental effects of estrogen on coronary disease. The preponderance of data, however, suggests that estrogen administration to postmenopausal women may reduce the incidence of death from cardiovascular disease by as much as one half; however, most of these reports were observational studies and not randomized or double-blind trials. The best data probably will come from the very large Women's Health Initiative Trial sponsored by the National Institutes of Health. Results may not be available until 2005 or later.
Data on the use of estrogen for secondary prevention of coronary heart disease (CHD) in women were published in 1998.142 This prospective randomized trial of 2,763 women with documented CHD followed the subjects an average of 4.1 years. The women were randomly assigned to a continuous regimen of 0.625 mg conjugated equine estrogens and 2.5 mg medroxyprogesterone acetate administered daily or placebo. At the end of four years there were no significant differences between the two groups with regard to the occurrence of angioplasty, coronary bypass procedures, myocardial infarction, or CHD death. The group on HRT had more surgical gallbladder disease and thromboembolic events. Prior observational studies had reported a significant benefit with HRT in the setting of secondary prevention of CHD. The results of this study underscore the importance of well-designed clinical trials in confirming or disputing the results of observational studies. The Women's Health Initiative will provide more data on this subject.
Estrogen also has an effect on liver function. The effects are influenced by the dose, the route of administration, and the type of estrogen used. The usual estrogen replacement dose, 0.625 mg of conjugated equine estrogen daily, is about one fifth as potent as one dose commonly used in low-dose oral contraceptives, 30 μg of ethinyl estradiol. The synthetic estrogens used in oral contraceptives, unlike the natural estrogens used for estrogen replacement, significantly increase globulins produced in the liver, including renin substrate (angiotensinogen), causing elevated blood pressure in some women.143 Natural estrogens also stimulate hepatic synthesis of renin substrate but to a much lesser extent. Blood pressure is unaffected by postmenopausal ERT,144,145 except for the 5% to 8% of such women who develop an idiosyncratic elevation.146 Several observational and prospective reports have indicated an increased risk of VTEs with use of ERT.147,148,149,150,151,152 The increase in relative risk was 2.0 to 3.6. The absolute risk is small because of the overall low incidence of these events (less than 1 in 10,000). However, because of the potential serious and life-threatening sequelae of VTEs caution should be exercised in assessing the risk to benefit ratio in individuals deemed to be at increased risk of VTEs.
Several small studies of different progestins suggest that the synthetic progestins commonly used together with estrogen for replacement therapy have an adverse effect on lipoprotein metabolism, causing a substantial increase in LDL cholesterol and a significant decrease in HDL cholesterol.153 In contrast, data from the prospective Postmenopausal Estrogen-Progestin Intervention Trial showed that micronized progesterone did not adversely affect the beneficial effects on lipids of conjugated equine estrogens.151 The effects of progestins on lipoproteins are greater with the 19-nortestosterone derivatives and appear to be dose dependent.154 During the phase of the treatment cycle when estrogen and progestin are given together, it appears that the beneficial effects of estrogen on lipoprotein cholesterol levels are negated at least in part.155,156,157 These findings have led to the common recommendation that progestogens, if prescribed, should be given in the lowest possible dose needed to achieve the desired histologic changes in the endometrium and should not be given to women who have undergone hysterectomy. The clinical significance of the effect of progestins on the lipid profile is not known. Early research on cardiovascular health and HRT focused on the beneficial effect of HRT on the lipid profile.
Estrogen interacts with the cardiovascular system in many ways. Documented effects of estrogen include a decrease in fibrinogen, lipoprotein a, plasminogen activator inhibitor, fasting glucose, collagen formation, and neointimal proliferation.158,159,160,151 Estrogen appears to enhance vasodilation and collateral vessel formation161 The effects of estrogens on lipids may be of little added benefit to their apparently beneficial cardiovascular effects. Several groups have attempted to estimate the effects of estrogen alone and estrogen given with a progestin to postmenopausal women for HRT.162,163 More studies are needed to define the benefits of estrogens on cardiovascular disease and to determine the optimal way in which estrogens and progestins should be administered.
Psychologic and Other Symptoms
Complaints of fatigue, nervousness, headache, insomnia, depression, irritability, joint and muscle pain, forgetfulness, inability to concentrate, dizziness, palpitations, and formication are also indicative of the menopausal syndrome. Many of these symptoms can be attributed to the sleep deprivation that results from frequent night sweats and may be avoided by taking estrogen. Postmenopausal women treated with estrogen replacement in one study had an improvement in their hot flush frequency and severity, insomnia, urinary frequency, vaginal dryness, frequency of headaches, mood, and memory. Treatment in postmenopausal women without flushes and night sweats improves only their vaginal atrophy, memory, and mood.164 In this same study, estrogen was not found to improve arthralgia, backache, or vaginal discomfort and had no effect on skin condition, coital satisfaction, or frequency of orgasm. It is unclear whether fatigue, irritability, anxiety, nervousness, and depression are caused by estrogen deficiency or another alteration at the central nervous system level. It has been suggested that estrogen is an inhibitor of monoamine oxidase, an enzyme whose levels are elevated in some depressed women.165
A decrease in the intensity and duration of the sexual response and a decline in libido is seen in some women after menopause. Most menopausal women remain sexually active, and estrogen replacement with the use of a vaginal lubricant has been helpful in relieving the dyspareunia associated with vaginal atrophy. One major reason for decreased sexual activity among older women is lack of an able partner.
HORMONE REPLACEMENT THERAPY
The decision to place a woman on hormone replacement must be made on an individual basis, weighing all risks and benefits. The patient must be willing to take hormonal replacement with the understanding that the regimen may change as more studies assessing the risks and benefits and the best mode of administration are published.
Complications of Estrogen Therapy
Exogenous estrogens, even in physiologic quantities, may lead to any of the several problems enumerated in the following sections.
ENDOMETRIAL CANCER.
The primary risk of ERT is the development of adenocarcinoma of the endometrium if estrogen is given without the addition of a progestin. Estrogen is a definitive risk factor in the development of this malignancy, with a 4- to 12-fold increased incidence reported in long-term users.166,167,168,169 The epidemiologic studies have multiple methodologic deficiencies and differences to account for the variation in the reported relative risk. The incidence of endometrial cancer appears related to the dose and the duration of estrogen use, with the added risk becoming negligible within 6 months of discontinuation of therapy. The prospective PEPI trial confirms earlier reports.170
There is a consistent progression seen in the endometrium from hyperplasia, to hyperplasia with atypia, and to adenocarcinoma with the use of continuous unopposed estrogen. Twenty-three percent of women on continuous estrogen develop cystic or adenomatous hyperplasia. Ten percent of women with adenomatous hyperplasia eventually develop frank carcinoma. The carcinoma associated with estrogen use is low grade, well differentiated,171 and usually cured by simple hysterectomy. The mortality rate of women with estrogen-associated endometrial carcinoma is less than that of nonusers; estrogen users developing this carcinoma have a 10-year survival rate of 90%, compared with 50% for the control group.172
Several studies reported that estrogen-induced hyperplasia and carcinoma of the endometrium can be prevented by the addition of a progestin.173,174,175 However, one study indicated twice the rate of hyperplasia in women using cyclic estrogen and progestin an average of 4 years compared with nonusers.176 Progestins block estrogen receptor synthesis,177 induce estradiol dehydrogenase (the enzyme that converts estradiol to estrone),178 and increase the rate of sulfation of estrogen in the endometrium.179 These actions limit the effect estrogen has on the endometrium, thereby preventing endometrial proliferation. Norethindrone (350 μg) or norgestrel (150 μg) can decrease receptor DNA activity in women on 0.625 mg of conjugated estrogen to the level normally seen in the secretory phase of the menstrual cycle. Although dosages of MPA less than 10 mg have not been proved to eliminate the risk of endometrial carcinoma, they decrease the receptor activity and may be protective if given for more than 12 days. Some data suggest that duration of therapy may be more important than dose with regard to hyperplasia;180 however, results of long-term use of low-dose progestins have not been reported, and one very large short-term study involving 1385 women on four different regimens of estrogen and MPA found hyperplasia only in the two groups using the lowest amount of MPA.181 The maximal effects of progestins are not seen until after 6 days of continuous therapy, and hyperplasia is usually inhibited when these agents are given for 12 or more days.182
BREAST CANCER.
In the United States, 1 of every 8 women develops breast cancer. It is the most prevalent malignancy of women (32%) and the second leading cause of death attributed to cancer (18%), with 10 times the number of deaths compared with endometrial cancer. Lung cancer surpassed breast cancer as the leading cause of cancer death for women in 1987. However, far more women get breast cancer than lung cancer. Whether estrogen is an etiologic agent is unknown. Because breast cancer is 182 times more common in women than men, occurs after puberty, often contains estrogen and progesterone receptors, responds to endocrine ablation therapy, and is found in decreased numbers of women castrated before age 35, there is a strong implication that estrogen has a role in the development of this disease or serves as an important cofactor. The risk factors associated with breast cancer all involve prolonged exposure to unopposed estrogen and include low parity, birth of first child after age 30, obesity, anovulation, infertility, early menarche, and late menopause. Animal data suggest that breast cancer can be induced with high-dose estrogen.
Because of the importance of the breast cancer issue and the lack of consistent findings among the many published studies,183,184,185,186,187,188,189,190,191,192,193 several investigators have performed meta-analyses. Two investigators claim that there is no significant increase in the risk of breast cancer associated with the use of hormone replacement therapy (HRT),194,195 and four suggest an increased risk associated with extended use.196,197,198,199 Any selection bias in the past against prescribing hormones for women with a family history of breast cancer may have produced an underestimation of the risk of breast cancer. Surveillance bias in women taking estrogen may have led to an overestimation of the risk of breast cancer. A breast examination and mammogram should be done before the institution of hormonal treatment and at appropriate intervals thereafter. Further studies are needed to define the effects of exogenous estrogen and progestin on the breast.
GALLBLADDER DISEASE.
Estrogen replacement, like oral contraceptives, may increase cholelithiasis in susceptible patients by increasing cholesterol saturation of the bile. The risk of gallbladder disease was reported to increase more than 2.5-fold in women on ERT.200,201 Progestational agents alone have also been associated with an elevated risk of gallstones.
OTHER DISEASES.
New-onset asthma and systemic lupus erythematosus have been reported to occur twice as often in ERT users as in nonusers.202,203 The mechanism is not fully understood.
Contraindications to Hormone Replacement Therapy
Contraindications to HRT include uncontrolled hypertension, unexplained vaginal bleeding, impaired liver function, active thromboembolic disease, porphyria, and breast cancer (Table 9). Although the data with regard to estrogens and breast cancer have led many clinicians to refuse to prescribe estrogens for women with a history of breast cancer, there are some clinical observations suggesting estrogens may not accelerate breast cancer. First, there is no difference in survival when pregnant women with breast cancer are matched to nonpregnant women by age and stage of disease; moreover, termination of pregnancy is not associated with improved survival.204 Second, although pregnant women have a 2.5-fold greater risk of metastases, the reason is diagnosis at a later stage because of the breast changes associated with pregnancy.205 Third, a pregnancy after diagnosis and appropriate therapy for breast cancer has no negative impact on prognosis.206 Fourth, there is no evidence that use of oral contraceptives, containing much larger doses of estrogen than prescribed for postmenopausal women, increases the overall risk of developing breast cancer.207,208,209 Fifth, some small studies have reported that estrogens so not increase the recurrence rate in women with breast cancer.210,211,212 In perhaps the best of these, a case-control study from Australia,212 the risk of recurrence was not increased among 90 estrogen users compared with two matched controls for each user (relative risk, 0.40; 95% confidence interval, 0.17–0.93); among users, there were no deaths, and only 7% developed a recurrence compared with 17% of the nonusers. Not all reports are in agreement on these issues. For example, a report from M. D. Anderson Cancer Center concludes that a concurrent or recent pregnancy adversely affects survival rates in women with breast cancer.213 Some investigators have argued that tamoxifen is a better choice than estrogen for women with a history of breast cancer.214 Tamoxifen does have a positive effect on bone density, lipid concentrations, and the occurrence of myocardial infarctions,215,216,217,218 but the effects do not appear as great as those reported with estrogen.
TABLE 9. Contraindications to Estrogen Therapy
Strong | Relative |
Unexplained vaginal bleeding | Hypertriglyceridemia |
Uncontrolled hypertension | Leiomyomas |
Impaired liver function | Endometriosis |
Active thromboembolic disorders | Gallbladder disease |
Porphyria | Pancreatitis |
Breast cancer | Migraine headaches |
| Strong family history of breast cancer |
| Endometrial cancer |
Taken together, these data suggest there may be times when it is acceptable to give exogenous estrogens to women with a history of breast cancer who want very much to take estrogen. There seems to be little point in withholding estrogen from women with widely disseminated breast cancer who desire estrogen because their quality of life is miserable with menopausal symptoms. Patients with a low risk of recurrence, including those more than 5 years from a diagnosis without evidence of disease, those with ductal carcinoma in situ, those without any positive axillary nodes, those with tumor size less than 1 cm, those who are estrogen receptor negative, and those with well-differentiated (nuclear grade 1) tumors, would appear to be especially good candidates for consideration for estrogen. However, women electing estrogen therapy must be aware of the potential risks; for most women, it is probably prudent to treat menopausal symptoms with agents other than estrogen until the risks are known.
Relative contraindications include gallbladder disease, pancreatitis, leiomyomas, endometriosis, migraine headaches, seizures, hypertriglyceridemia, endometrial cancer, history of thromboembolic disease, and a strong family history of breast cancer. Consensus is developing that it is probably safe to prescribe HRT for a woman with an early-stage, low-grade endometrial cancer who has had a hysterectomy. In most instances, the level of estrogen used in HRT is not sufficient to stimulate endometriosis and leiomyomas. The decision to give HRT to women who fall into any of these categories must be based on the severity of the symptoms and the circumstances. The patient should be well informed of the potential adverse effects of the treatment and must clearly believe that the benefits to her are worth the risks. There is no contraindication to the use of HRT in women with a history of cervical or ovarian cancer.
Preparations of Estrogen and Progestin
There are several classes of estrogens. Naturally occurring estrogens, including estradiol, estrone, and conjugated estrogens (composed of many estrogens, including estrone sulfate, equilin, and equilenin), are the estrogens generally given for replacement therapy. Synthetic estrogens, including ethinyl estradiol, mestranol, and quinestrol, and the nonsteroidal estrogens, including diethylstilbestrol and chlorotrianisene, typically are not used for ERT.
Estrogen can be administered through a variety of routes, including oral, intramuscular, topical, subcutaneous, nasal, and vaginal. Not all forms are available in the United States. Nasal sprays allow direct rapid absorption. Intramuscular injection is convenient, requiring infrequent administration, but immediate reversal is impossible, and tolerance may develop. Moreover, very high circulating levels of estrogen may be achieved soon after administration. Subcutaneous pellets also give sustained release, but immediate reversal may not be possible because retrieval of the pellet is difficult. Estrogen creams are used extensively in France but require a wide area of application. Transdermal patches allow direct absorption, but the effect is not sustained; therefore, the patch must be worn continually and reapplied at appropriate intervals. The most frequent complication of transdermal delivery is skin irritation. Vaginal suppositories and creams permit direct absorption but are unacceptable to many women. A low-dose vaginal ring that delivers 7.5 μgm estradiol per day over a 90-day period provides a local effect without raising serum estradiol levels above the menopausal range.219 The oral route is most convenient but is the only mode of delivery that significantly affects the liver.
The most commonly prescribed estrogen is oral conjugated equine estrogen. A daily dose of 0.625 mg is effective in eliminating complaints in most postmenopausal women (Table 10). Equivalent oral alternatives include piperazine estrone sulfate at a dose of 0.625 to 1.25 mg, which has less of an effect on renin substrate and may therefore be preferable in women with hypertension, and micronized estradiol-17β at a dose of 1 mg. The equivalent transdermal estradiol-17β dose is 0.05 mg to 0.1 mg. Higher dosages may be necessary when first starting replacement therapy in women with severe symptoms. Moreover, the dosage of any estrogen preparation must be individualized.
TABLE 10. Approximately Equivalent Estrogen Dosages
Administration Method | Dosages* |
Oral | 0.625 mg conjugated equine estrogen |
| 0.625–1.25 mg piperazine estrone sulfate |
| 1 mg micronized estradiol-17β |
Transdermal | 0.05–0.1 mg estradiol-17β |
*Daily.
Estrogen administration is associated with a number of side effects that may affect compliance. Initially, most women experience some breast tenderness. If breast discomfort persists, the dosage of estrogen should be reduced. Some women require much higher doses for alleviation of their symptoms; young, surgically oophorectomized women often need twice as much estrogen as those who underwent physiologic menopause. Other side effects include nausea, vomiting, weight gain up to 5 lb, fluid retention, and heartburn. Fluid retention and weight gain often may be abolished by restricting salt intake.
The most frequent complaint with hormonal replacement is uterine bleeding. The frequency of irregular bleeding is related to the estrogen dose, with 1.25 mg of conjugated estrogen associated with a 2% to 12% incidence and 0.625 mg associated with a 1.4% incidence.220 When progesterone is added to the regimen, the incidence of irregular bleeding diminishes markedly.
Progestin is usually administered only orally. The most commonly prescribed progestin in the United States is MPA at a dose of 10 mg. This dose is not well tolerated in as many as 25% of women. Common complaints include bloating, depression, premenstrual tension-like symptoms, acne, and breast tenderness. Beginning with a dose of 5 mg and increasing the dose to 10 mg in those women without complaints reduces the number of women discontinuing therapy. It may even be necessary to decrease the dose to 2.5 mg in some women. Norgestrel (150 to 500 μg) and norethindrone acetate (1 to 5 mg) are frequently used in Europe. These 19-norsteroids lower the ratio of high-density to low-density lipoproteins more than MPA and therefore are not commonly used in the United States.221 However, the effect on lipoproteins may not be significant with the use of lower doses,222 and the effect of HRT on the lipid profile may not be the only mechanism whereby HRT reduces the incidence of cardiovascular disease. Other progestins may also be used. Micronized progesterone is well absorbed,223 has little or no effect on the lipid profile,224,151 and has been approved for use in the United States. Progesterone in vaginal gel form is also available. Other progestins, such as norgestimate, gestodene, and transdermal levonorgestrel and norethindrone acetate are being investigated.
Treatment Regimens
Many regimens are being used, none of which is physiologic. Estrogen is usually given with a progestin to women with a uterus to prevent endometrial hyperplasia. Estrogen is given alone to women without a uterus to avoid the deleterious effect of progestin on lipoproteins.138
One of the most widely prescribed regimens in the United States for women with a uterus is the use of an estrogen for the first 25 days each month with the addition of MPA (5 to 10 mg) for days 13 to 25. Women who are symptomatic during the drug-free days can be given estrogen continuously, with MPA administered for the first 13 days of each month.
In Europe, most women are given continuous estrogen therapy with 12 to 14 days of progestin. This regimen has gained popularity in the United States, because bleeding is no more frequent than with the intermittent cyclic regimens and because this regimen is easier for the patient to remember. Women with fibrocystic condition of the breast may benefit from cyclic regimens with days off estrogen therapy. Continuous daily administration of a combination of an estrogen and a progestin has become more popular.225,226 Unfortunately, irregular breakthrough bleeding occurs frequently in the first 6 to 9 months of therapy.227 Moreover, the ratios of estrogen to progestin are empiric. Occasional reports of cancer of the uterus occurring with this regimen have appeared.228,229,230 Another suggested regimen provides estrogen and progestin Monday through Friday of each week, with no hormonal replacement given on the weekends. Quarterly use of progestin has also been reported. Although women preferred the quarterly progestin to monthly progestin, they did have longer, heavier menses, with almost twice the incidence of hyperplasia of the endometrium after 1 year (1.5% versus 0.9%).231 However, the incidence in both groups is very low.
How long therapy of postmenopausal and oophorectomized women should continue is unknown. Relief of mild menopausal symptoms may be achieved by short-term therapy tapering to none. Prophylaxis against cardiovascular disease in the setting of a strong family history of cardiovascular disease may result in indefinite use of HRT. The same is true for protection against osteoporosis.
Evaluation of Patients on Hormonal Therapy
Before institution of HRT, a complete history and physical examination should be completed (Table 11). Pertinent tests include a stool guaiac, a Pap smear, baseline mammogram, a sequential multiple analyzer (SMA) assay, and fasting cholesterol, triglycerides, and glucose concentrations. Liver function tests are required in women with a history of liver disease. Pretreatment endometrial biopsies are not necessary for all women. Biopsies should be performed in women with irregular bleeding and in those at increased risk for endometrial carcinoma. Women at increased risk include those with a positive family history for endometrial or breast carcinoma, obesity, alcoholism, hepatic disease, and a long history of amenorrhea or oligomenorrhea during their reproductive years. Some recommend pretreatment biopsies in women who still withdraw to a short course of MPA,174 although the value of this has not been confirmed.
TABLE 11. Initial Workup Before Initiating Estrogen Replacement Therapy
History and physical examination
Stool guaiac
Pap smear
Mammogram
SMA
Fasting cholesterol
Triglycerides
Glucose
Liver function tests (with past history of liver disease)
Endometrial biopsy (in high-risk groups)
SMA, sequential multiple analyzer assay.
After replacement therapy is initiated, patients should be evaluated in 4 to 6 weeks to adjust the dosage if necessary and to evaluate side effects or complications. If severe headaches, visual changes, chest pain, or symptoms of thrombophlebitis develop, estrogen should be discontinued immediately. If hypertension develops with the onset of therapy and cannot be controlled, then therapy should be stopped. Blood pressure usually returns to normal in those women. It has been suggested that biopsies be performed in women receiving cyclic progestin only if bleeding occurs before day 11 of progestin therapy,232 but these data require substantiation. A biopsy should be performed immediately in any woman who develops abnormal bleeding. Women on unopposed estrogen should have an annual endometrial biopsy even in the absence of any bleeding. Breast and pelvic examination, blood pressure monitoring, and a stool guaiac test should be repeated at least yearly. Periodic mammograms should also be performed, with the frequency dictated by age and the presence of risk factors. Pap smears should be obtained every 1 to 3 years, depending on history and risk factors. Although the roles of exogenous estrogen and progesterone therapy in cardiovascular disease and breast cancer have not been clearly defined, the use of this hormonal combination has been found to be cost effective and also has been shown to increase life expectancy by 1 month relative to no treatment.233 Other mathematical models predict -0.5 to + 2.2 years change in life expectancy, depending on individual baseline risk factors.162 Attempts to create mathematical models are hampered by the lack of randomized double-blind studies regarding cardiovascular disease and breast cancer, the lack of definitive data regarding the impact of progestins on cardiovascular risks and breast cancer risks, and the issue of selection bias in the existing studies.234 Despite these limitations, a very elaborate mathematical analysis using a Markov state transition model concluded that “the only women not expected to gain from this treatment are those who are both at greatest risk for breast cancer and at least risk for coronary heart disease.”235
Alternatives to Hormone Replacement Therapy
Menopause is a normal and natural event in the female life span. Although HRT may provide benefits for many women, not all women want or need to use HRT. The life expectancy of women already exceeds that of men, and many elderly women enjoy an excellent quality of life without HRT. All women should be counseled regarding the healthy lifestyle that they themselves can adopt: low-fat, lowcholesterol diet; adequate calcium and vitamin D; exercise; and avoidance of smoking, excessive alcohol, and obesity. A decision to use or not to use HRT is not irrevocable; it can be changed as new information becomes available. Patient and physician can reassess the current research and future health goals at each annual examination.
REFERENCES
Amundsen DW, Diers CT: The age of menopause in medieval Europe. Hum Biol 45: 605, 1973 |
|
McKinlay S, Jeffreys M, Thompson B: An investigation of the age of menopause. J Biosoc Sci 4: 161, 1972 |
|
Rebar RW, Erickson GF, Yen SSC: Idiopathic premature ovarian failure: Clinical and endocrine characteristics. Fertil Steril 37: 35, 1982 |
|
Sherman BW, Korenman SG: Hormonal characteristics of the human menstrual cycle throughout reproductive life. J Clin Invest 55: 699, 1975 |
|
Sherman BW, West JH, Korenman SG: The menopausal transition: Analysis of LH, FSH, estradiol and progesterone concentrations during menstrual cycles of older women. J Clin Endocrinol Metab 42: 629, 1976 |
|
Grodin JM, Siiteri PK, MacDonald PC: Source of estrogen production in postmenopausal women. J Clin Endocrinol Metab 36: 207, 1973 |
|
Judd HL, Judd GE, Lucas WE et al: Endocrine function of the postmenopausal ovary concentrations of androgens and estrogens in ovarian and peripheral vein blood. J Clin Endocrinol Metab 39: 1020, 1974 |
|
Longcope C, Pratt JH, Schneider SH, Fineberg SE: Aromatization of androgen by muscle and adipose tissue in vivo. J Clin Endocrinol Metab 46: 164, 1978 |
|
Chang RJ, Judd HL: The ovary after menopause. Clin Obstet Gynecol 24: 181, 1981 |
|
Judd HL, Lucas WE, Yen SSC: Serum 17β-estradiol and estrone levels in postmenopausal women with and without endometrial cancer. J Clin Endocrinol Metab 43: 272, 1976 |
|
Vermeulen A: The hormonal activity of the postmenopausal ovary. J Clin Endocrinol Metab 42: 247, 1976 |
|
Longcope C, Kato T, Horton R: Conversion of blood androgens to estrogens in normal adult men and women. J Clin Invest 48: 2191, 1969 |
|
Greenblatt RB, Colle ML, Mahesh VB: Ovarian and adrenal steroid production in the postmenopausal woman. Obstet Gynecol 47: 383, 1976 |
|
Judd HL, Shamonki IM, Frumar AM, LaGassa LD: Origin of serum estradiol in postmenopausal women. Obstet Gynecol 59: 680, 1982 |
|
Judd HL: Hormonal dynamics associated with the menopause. Clin Obstet Gynecol 19: 775, 1976 |
|
Nisker JA, Hammond GL, Davidson GL et al: Sex hormone binding globulin capacity and the percentage of free estradiol in postmenopausal women with and without endometrial carcinoma. Am J Obstet Gynecol 138: 637, 1980 |
|
Scaglin HM, Medina AL, Pinto-Ferreira AG et al: Pituitary LH and FSH secretion and responsiveness in women of old age. Acta Endocrinol 81: 673, 1976 |
|
Morine SE, Jaffe RB, Midgley AR Jr: Regulation of human gonadotropins. XIII. Changes in serum gonadotropins in menstruating women in response to oophorectomy. J Clin Endocrinol Metab 34: 420, 1972 |
|
Yen SSC, Tsai CC, Naftolin F et al: Pulsatile patterns of gonadotropin release in subjects with and without ovarian function. J Clin Endocrinol Metab 34: 671, 1972 |
|
Judd HE, Lucas WI, Yen SSC: Effect of oophorectomy on circulating testosterone and androstenedione levels in patients with endometrial cancer. Am J Obstet Gynecol 118: 793, 1974 |
|
Abraham GE: Ovarian and adrenal contribution to peripheral androgens during the menstrual cycle. J Clin Endocrinol Metab 39: 340, 1974 |
|
Yen SSC: The biology of menopause. J Reprod Med 18: 287, 1977 |
|
Anderson E, Hamburger S, Liu JH, Rebar RW: Characteristics of menopausal women seeking assistance. Am J Obstet Gynecol 156: 428, 1987 |
|
Chakravarti S, Collins WP, Thom MH, Studd JWV: Relation between plasma hormone profiles: Symptoms and response to estrogen treatment in women approaching the menopause. Br Med J 1: 983, 1970 |
|
Jaszmann LJB, Van Lith ND, Zaat JLA: The perimenopausal symptoms. Med Gynaecol Sociol 4: 268, 1969 |
|
Thompson B, Hart SA, Dumo D: Menopausal age and symptomatology in general practice. J Biosoc Sci 5: 71, 1973 |
|
McKinlay S, Jeffreys M: The menopausal syndrome. Br J Prev Soc Med 25: 108, 1974 |
|
Erlik Y, Meldrum DR, Judd HL: Estrogen levels in postmenopausal women with hot flushes. Obstet Gynecol 59: 403, 1982 |
|
Stone SL, Mickal A, Rye PH: Postmenopausal symptomatology, maturation index and plasma estrogen levels. Obstet Gynecol 45: 625, 1975 |
|
Hutton JD, Jacobs HS, Murray MAF, James UHT: Relation between plasma oestrone and oestradiol and climacteric symptoms. Lancet 1: 678, 1978 |
|
Erlik LY, Tataryn IV, Meldrum DR et al: Association of waking episodes with menopausal hot flushes. JAMA 245: 2405, 1979 |
|
Tataryn IV, Lomax P, Meldrum DR et al: Objective techniques for the assessment of postmenopausal hot flashes. Obstet Gynecol 57: 340, 1981 |
|
Meldrum DR, Shamonki IM, Frumar AM et al: Elevation in skin temperature of the finger as an objective index of postmenopausal hot flashes: Standardization of the technique. Am J Obstet Gynecol 135: 713, 1979 |
|
Yen SSC, Jaffe RB: Reproductive Endocrinology, Physiology, Pathophysiology and Clinical Management, p 393. Philadelphia: WB Saunders, 1991 |
|
Ginsburg J, Swinhoe J, O'Reilly B: Cardiovascular responses during the menopausal hot flush. Br J Obstet Gynaecol 88: 925, 1981 |
|
Tataryn IV, Lomax P, Bajorek JA et al: Postmenopausal hot flushes: A disorder of thermoregulation. Maturitas 2: 101, 1980 |
|
Casper RF, Yen SSC, Wilkes MM: Menopausal flushes: A neuroendocrine link with pulsatile luteinizing hormone secretion. Science 205: 823, 1979 |
|
Meldrum DR, Tataryn IV, Frumar AM et al: Gonadotropins, estrogen, and adrenal steroids during the menopausal hot flush. J Clin Endocrinol Metab 50: 685, 1980 |
|
Kronenberg F: Hot flushes. In Lobo RA (ed): Treatment of the Postmenopausal Woman, Basic and Clinical Aspects, p 97. New York: Raven Press, 1994 |
|
Tataryn IV, Meldrum DR, Lu KH et al: LH, FSH and skin temperature during the menopausal hot flash. J Clin Endocrinol Metab 49: 152, 1979 |
|
Meldrum DR, Erlik Y, Lu JK, Judd HL: Objectively recorded hot flashes in patients with pituitary insufficiency. J Clin Endocrinol Metab 52: 681, 1981 |
|
Mulley G, Mitchell JRA, Tattersall RB: Hot flashes after hypophysectomy. Br Med J 2: 1062, 1977 |
|
Casper RF, Yen SSC: Menopausal flushes: Effect of pituitary gonadotropin desensitization by a potent luteinizing hormone-releasing factor agonist. J Clin Endocrinol Metab 53: 1056, 1981 |
|
DeFazio J, Meldrum DR, Laufer L et al: Induction of hot flashes in premenopausal women treated with a long acting GnRH agonist. J Clin Endocrinol Metab 56: 445, 1983 |
|
Simpkins JW, Katovich MJ: An animal model for pharmacologic evaluation of the menopausal hot flush. In Notelovitz M, Van Keep P (eds): The Climacteric in Perspective, p 213. Boston: MTP Press, 1986 |
|
Clayden JR, Ball JW, Pollard P: Menopausal flushing double-blind trial of a nonhormonal medication. Br Med J 1: 409, 1974 |
|
Freedman RR, Woodward S, Sabharwal SC: α2 -Adrenergic mechanism in menopausal hot flushes. Obstet Gynecol 76: 573, 1990 |
|
Kronenberg F, Cote LJ, Linkie DM et al: Menopausal hot flashes: Thermoregulatory, cardiovascular and circulating catecholamine and LH changes. Maturitas 6: 31, 1984 |
|
Mashchak CA, Kletzky OA, Artal R, Mishell DR Jr: The relation of physiological changes to subjective symptoms in postmenopausal women with and without hot flushes. Maturitas 6: 301, 1984 |
|
Kalra S, McCann SM: Effects of drugs modifying catecholamine synthesis on LH release induced by preoptic stimulation in the rat. Endocrinology 93: 356, 1973 |
|
Ojeda SR, Jameson HE, McCannon I: Hypothalamic areas involved in prostaglandin (PG) induced gonadotropin release. I. Effects of PGE2 and PGF2α implants on luteinizing hormone release. Endocrinology 100: 1585, 1977 |
|
Veale WL, Cooper KE: Comparison of sites of action of prostaglandin E and leukocyte pyrogen in brain. In Lomax P, Schonbaum E, Jacob J (eds): Temperature Regulation and Drug Action, p 218. New York: S Karger, 1975 |
|
Spitzer IB, Rebar RW: Physiology and measurement of hot flushes. Am J Obstet Gynecol 156: 1284, 1987 |
|
Wehrenberg WB, Wardlaw SL, Frantz AC et al: β-Endorphin in hypophyseal portal blood: Variations throughout the menstrual cycle. Endocrinology 111: 879, 1982 |
|
Wardlaw SL, Wehrenberg WB, Fenn M et al: Effects of β-endorphin in hypophyseal portal blood. J Clin Endocrinol Metab 55: 877, 1982 |
|
Coope J: Double-blind crossover study of estrogen replacement therapy. In Campbell S (ed): The Management of the Menopause and Postmenopausal Years, p 159. Baltimore: University Park Press, 1976 |
|
Campbell S, Whitehead M: Oestrogen therapy and the menopausal syndrome. Clin Obstet Gynecol 4: 31, 1977 |
|
Schiff I, Tulchinsky D, Cramer D, Ryan KJ: Oral medroxyprogesterone treatment of postmenopausal symptoms. JAMA 244: 1443, 1980 |
|
Lobo RA, McCormick W, Singer F et al: Depomedroxy-progesterone acetate compared with conjugated estrogens for the treatment of postmenopausal women. Obstet Gynecol 63: 1, 1984 |
|
Laufer LR, Erlik Y, Meldrum DR et al: Effect of clonidine on hot flashes in postmenopausal women. Obstet Gynecol 60: 583, 1982 |
|
Raz P, Stamm WE: A controlled trial of intravaginal estriol in postmenopausal women with recurrent urinary tract infections. N Engl J Med 329: 753, 1993 |
|
Punnonen R: Effects of castration and peroral estrogen therapy on the skin. Acta Obstet Gynecol Scand Suppl 21: 3, 1972 |
|
Albright F, Bloomberg F, Smith DH: Postmenopausal osteoporosis. Trans Assoc Am Physicians 55: 298, 1940 |
|
Herzog DB, Copeland PM: Eating disorders. N Engl J Med 313: 295, 1985 |
|
Bachrach LK, Katzman DK, Litt IF et al: Recovery from osteopenia in adolescent girls with anorexia nervosa. J Clin Endocrinol Metab 72: 602– 606, 1991 |
|
Heaney RP: Estrogens in postmenopausal osteoporosis. Clin Obstet Gynecol 19: 791, 1976 |
|
Ray NF, Chan JK, Thamer M, Melton LJ III Medical expenditures for the treatment of osteoporotic fractures in the United States in 1995. Report from the National Osteoporosis Foundation. J Bone Min Res 12: 24, 1997 |
|
Riggs BL, Wahner HW, Melton LJ III et al: Rates of bone loss in the axial and appendicular skeleton of women: Evidence of substantial vertebral bone loss prior to menopause. J Clin Invest 77: 1487, 1986 |
|
Genant HK, Cann CE, Ettinger B, Gordon GS: Quantitative computed tomography of vertebral spongiosa: A sensitive method for detecting early bone loss after oophorectomy. Ann Intern Med 97: 699, 1982 |
|
Eriksen EF, Mosekilde L, Melsen F: Trabecular bone resorption depth decreases with age: Differences between normal male and females. Bone 6: 141, 1985 |
|
Heaney RP, Recker RR, Saville PD: Menopausal changes in bone remodeling. J Lab Clin Med 92: 964, 1978 |
|
Richelson LS, Wahner HW, Melton LJ et al: Relative contributions of aging and estrogen deficiency to postmenopausal bone loss. N Engl J Med 311: 1273, 1984 |
|
Mazess RB: On aging bone loss. Clin Orthop 165: 239, 1982 |
|
Smith DM, Khairi MRA, Johnson CC Jr: The loss of bone mineral with aging and its relationship to risk of fracture. J Clin Invest 56: 311, 1975 |
|
Lindsay R, Hart DM, Forrest C, Baird C: Prevention of spinal osteoporosis in oophorectomized women. Lancet 2: 1151, 1980 |
|
Aitken JM, Hart DM, Lindsay R: Estrogen replacement therapy for prevention of osteoporosis after oophorectomy. Br Med J 2: 515, 1973 |
|
Nordin BEC: Clinical significance and pathogenesis of osteoporosis. Br Med J 1: 571, 1971 |
|
Eriksen EF, Colvard DS, Berg NJ et al: Evidence of estrogen receptors in normal human osteoblast-like cells. Science 241: 84, 1988 |
|
Komm BS, Teipening CM, Benz DJ et al: Estrogen binding, receptor mRNA, and biologic response in osteoblast-like osteosarcoma cells. Science 241: 81, 1988 |
|
Slootweg MC, Ederveen AGH, Schot LPC et al: Oestrogen and progestogen synergistically stimulate human and rat osteoblast proliferation. J Endocrinol 133: R5, 1992 |
|
Nordin BEC, Gallagher JC, Aaron JE et al: Postmenopausal osteopenia and osteoporosis. Estrogens in the postmenopause. Front Horm Res 3: 131, 1975 |
|
Gallagher JC, Riggs BL, Deluca HF: Effects of estrogen, calcium absorption, and serum vitamin D metabolites in postmenopausal osteoporosis. J Clin Endocrinol Metab 51: 1359, 1980 |
|
Romagnoli E, Minisola S, Carnevale V et al: Effect of estrogen deficiency on IGF-1 plasma level: Relationship with bone mineral density in perimenopausal women. Calcif Tissue Int 53: 1, 1993 |
|
Bain SD, Bailey MC, Celino DL et al: High-dose estrogen inhibits bone resorption and stimulates bone formation in the ovariectomized mouse. J Bone Miner Res 8: 435, 1993 |
|
Golde B: New clues into the etiology of osteoporosis: The effects of prostaglandins (E2 and E3) on bone. Med Hypotheses 38: 125, 1992 |
|
Lindsay R, Hart DM. Aitken JM et al: Long-term prevention of postmenopausal osteoporosis by oestrogen. Lancet 1: 1038, 1976 |
|
Ettinger B, Grady D: Maximizing the benefit of estrogen therapy for prevention of osteoporosis. Menopause 1: 19– 34, 1994 |
|
Schneider DL, Barrett-Connor EL, Morton DJ et al: Timing of postmenopausal estrogen for optimal bone mineral density. JAMA 277: 543– 547, 1997 |
|
Paganini-Hill A, Ross RIC, Gerkins VR et al: Menopausal estrogen therapy and hip fractures. Ann Intern Med 95: 28, 1981 |
|
Weiss NS, Ure CL, Ballarch JH et al: Decreased risk of fractures of the hip and lower forearms with postmenopausal use of estrogen. N Engl J Med 303: 1195, 1980 |
|
Hammond CB, Jelovsek FR, Lee KL et al: Effects of long-term estrogen replacement therapy. I. Metabolic effects. Am J Obstet Gynecol 133: 525, 1979 |
|
Kiel DP, Felson DT, Anderson JJ et al: Hip fracture and the use of estrogens in postmenopausal women. N Engl J Med 317: 1169, 1987 |
|
Liberman UA, Weiss SR, Broll J et al: Effect of oral alendronate on bone mineral density and the incidence of fracture in postmenopausal osteoporosis. N Engl J Med 333: 1437– 1443, 1995 |
|
Black DM, Cummings SR, Karpf DB et al: Randomized trial of effect of alendronate on risk of fracture in women with existing vertebral fractures. Lancet 348: 1535– 1541, 1996 |
|
Greenberg C, Kukreja SC, Bowser EN et al: Effects of estradiol and progesterone on calcitonin secretion. Endocrinology 118: 2594, 1986 |
|
Taggart HM, Chestnut CH, Irey J: Deficient calcitonin response to calcium stimulation in postmenopausal osteoporosis. Lancet 1: 475, 1982 |
|
Torring O, Bucht E, Sjoberg HE: Plasma calcitonin response to a calcium clamp: Influence of sex and age. Horm Metab Res 17: 536, 1985 |
|
Tiegs RD, Body JJ, Wahner HW et al: Calcitonin secretion in postmenopausal osteoporosis. N Engl J Med 312: 1097, 1985 |
|
Gennari C, Chierichetti SM, Bagazzi S et al: Comparative effects on bone mineral content of calcium and calcium plus salmon calcitonin given in two different regimens in postmenopausal osteoporosis. Curr Ther Res 38: 455, 1985 |
|
Mazzuoli GF, Passeri M, Gennari C et al: Effects of salmon calcitonin in postmenopausal osteoporosis: A controlled double-blind clinical study. Calcif Tissue Int 38: 3, 1986 |
|
Overgaard K, Hansen MA, Jensen SB, Christiansen C: Effect of calcitonin given intranasally on bone mass and fracture rates in established osteoporosis: A dose-response study. Br Med J 305: 556, 1992 |
|
Austin LA, Health H III Calcitonin: Physiology and pathophysiology. N Engl J Med J 304: 269, 1981 |
|
Human calcitonin for Paget's disease. Med Lett Drugs Ther 29:47, 1987 |
|
Fisher B, Dignan J, Bryant J et al: Five versus more than five years of Tamoxifen therapy for breast cancer patients with negative lymph nodes and estrogen-positive tumors. J Natl Cancer Inst 88: 1529– 1542, 1996 |
|
Love RR, Mazess RB, Barden HS et al: Effects of tamoxifen on bone mineral density in postmenopausal women with breast cancer. N Engl J Med 326: 852, 1992 |
|
Fisher B, Costantino J, Redmond C et al: Endometrial cancer in tamoxifen-treated breast cancer patients: Findings from the National Surgical Adjuvant Breast and Bowel Project (NSABP) B-14. J Natl Cancer Inst 86: 527, 1994 |
|
Fornander T, Cedermark B, Mattsson A et al: Adjuvant tamoxifen in early breast cancer: Occurrence of new primary cancers. Lancet 1: 117, 1989 |
|
Delmas PD, Bjarnason NH, Mitlak BH et al: Effects of raloxifene on bone mineral density, serum cholesterol concentrations, and uterine endometrium in postmenopausal women. N Engl J Med 337: 1641– 1647, 1997 |
|
Dambacher MA, Ittner J, Ruegsegger P: Long-term fluoride therapy of postmenopausal osteoporosis. Bone 7: 199, 1986 |
|
Riggs BL, Hodgson SF, O'Fallon WM et al: Effect of fluoride treatment on the fracture rate in postmenopausal women with osteoporosis. N Engl J Med 322: 802, 1990 |
|
Heaney RP, Recker RR, Saville PD: Menopausal changes in calcium balance performance. J Lab Clin Med 92: 953, 1978 |
|
Recker RR, Saville PD, Heaney RP: Effect of estrogens and calcium carbonate in bone loss in postmenopausal women. Ann Intern Med 87: 649, 1977 |
|
Riis B, Thomsen K, Christiansen C: Does calcium supplementation prevent postmenopausal bone loss? A double-blind, controlled clinical study. N Engl J Med 316: 173, 1987 |
|
Albanese AA: Calcium nutrition in the elderly: Maintaining bone health to minimize fracture risk. Postgrad Med 63: 167, 1978 |
|
Riggs BL, Seeman E, Hodgson SF et al: Effect of the fluoride/calcium regimen on vertebral fracture occurrence in postmenopausal osteoporosis: Comparison with conventional therapy. N Engl J Med 306: 446, 1982 |
|
Chapuy ML, Arlot ME, Duboeuf F et al: Vitamin D3 and calcium to prevent hip fractures in elderly women. N Engl J Med 327: 1637, 1992 |
|
Reid IR, Ames RW, Evans MC et al: Effect of calcium supplementation on bone loss in postmenopausal women. N Engl J Med 328: 460, 1993 |
|
Dawson-Hughes B, Dall IGE, Krall EA et al: A controlled trial of the effect of calcium supplementation on bone density in postmenopausal women. N Engl J Med 323: 878, 1990 |
|
Kannel WB, Hyortland MC, McNamara PM, Gordon T: Menopause and coronary heart disease: The Framingham Study. Ann Intern Med 85: 447, 1976 |
|
Furman RH: Coronary heart disease and the menopause. In Ryan KJ, Gibson DC (eds): Menopause and Aging: Summary Report and Selected Papers from a Research Conference on Menopause and Aging, p 39. Washington, DC: United States Government Printing Office, 1973 |
|
Oliver MF: The menopause and coronary heart disease. In Campbell S (ed): The Management of the Menopause and Postmenopausal Years. Baltimore: University Park Press, 1976 |
|
Oliver MF, Boyd GS: Effect of bilateral ovariectomy on coronary artery disease and serum lipid levels. Lancet 2: 690, 1959 |
|
Parris HM, Carr CA, Hall DG, King TM: Time interval from castration in premenopausal women to development of excessive coronary atherosclerosis. Am J Obstet Gynecol 99: 155, 1967 |
|
Wuest J, Dry JT, Edwards JE: The degree of coronary atherosclerosis in bilaterally oophorectomized women. Circulation 7: 801, 1953 |
|
Colditz GA, Willett WC, Stampfer MJ et al: Menopause and the risk of coronary heart disease in women. N Engl J Med 316: 1105, 1987 |
|
Ritterbrand AB, Jaffe LA, Densen PM et al: Gonadal function and development of coronary artery disease. Circulation 26: 668, 1962 |
|
Sznajderman M, Oliver MF: Spontaneous premature menopause, ischemic heart disease and serum lipids. Lancet 1: 962, 1963 |
|
Willett W, Stampfer MJ, Bain C et al: Cigarette smoking, relative weight and menopause. Am J Epidemiol 117: 651, 1983 |
|
Hamilton M, Pickering GW, Robert JAF, Sowry GSC: The etiology of essential hypertension. I. The arterial pressure in the general population. Clin Sci 13: 11, 1954 |
|
Bolton CH: The effects of ethinyl estradiol and conjugated equine estrogen on plasma lipids in oophorectomized women. Arranged by the Institute of Obstetrics and Gynecology, University of Lancaster. The Management of the Menopause and Postmenopausal Years, p 185. Lancaster, UK: MTP Press, 1976 |
|
Pyorala T: The effect of synthetic and natural estrogens on glucose tolerance, plasma insulin and lipid metabolism in postmenopausal women. Arranged by the Institute of Obstetrics and Gynecology, University of Lancaster. The Management of the Menopause and Postmenopausal Years, p 195. Lancaster, UK: MTP Press, 1976 |
|
Furman RH: Are gonadal hormones of significance in the development of ischemic heart disease? Ann N Y Acad Sci 149: 822, 1968 |
|
Wahl P, Walden C, Knopp R et al: Effect of estrogen/progestin potency on lipid/lipoprotein cholesterol. N Engl J Med 308: 862, 1983 |
|
Blumenfeld Z, Aviram M, Brook GJ, Brandis JM: Changes in lipoprotein in subfractions following oophorectomy and estrogen replacement in perimenopausal women. Maturitas 5: 77, 1983 |
|
Jensen J, Riis B, Strom V et al: Long term effects of percutaneous estrogens and oral progesterone on serum lipoproteins in postmenopausal women. Am J Obstet Gynecol 156: 66, 1987 |
|
Stampfer MJ, Willett WC, Colditz GA et al: A prospective study of postmenopausal estrogen replacement therapy and coronary heart disease. N Engl J Med 313: 1044, 1985 |
|
Ross RK, Mack TM, Paganini-Hill A et al: Menopausal oestrogen therapy and protection from death from ischemic heart disease. Lancet 1: 858, 1981 |
|
Bush TL, Cowan LD, Barnett-Conner E et al: Estrogen use and all-cause mortality. Preliminary results from the Lipid Research Clinical Program Follow-up Study. JAMA 249: 903, 1983 |
|
Wilson PWF, Garrisen RJ, Castelli UP: Postmenopausal estrogen use, cigarette smoking and cardiovascular morbidity in women over 50: The Framingham Study. N Engl J Med 313: 1038, 1985 |
|
Gordon T, Kannel WB, Hyortland MC, McNamara PM: Menopause and coronary heart disease. Ann Intern Med 89: 157, 1978 |
|
Sidney S, Petitti DB, Quesenberry CP Jr: Myocardial infarction and the use of estrogen and estrogen-progestogen in postmenopausal women. Ann Intern Med 127: 501– 508, 1997 |
|
Hulley S, Grady G, Bush T et al: Randomized trial of estrogen plus progestin for secondary prevention of coronary heart disease in postmenopausal women. JAMA 280: 605, 1998 |
|
Mashchak CA, Lobo RA, Duzono-Takano R et al: Comparison of pharmacodynamic properties of various estrogen formulations. Am J Obstet Gynecol 144: 511, 1982 |
|
Pfeffer RI, Kurosaki TT, Charlton SK: Estrogen use and BP in later life. Am J Epidemiol Med 110: 469, 1979 |
|
Pfeffer RI: Estrogen use, hypertension and stroke in postmenopausal women. J Chronic Dis 31: 389, 1978 |
|
Mashchak CA, Lobo RA: Estrogen replacement therapy and hypertension. J Reprod Med 30: 805, 1985 |
|
Daly E, Vessey MP, Hawkings MM et al: Risk of venous thromboembolism in users of hormone replacement therapy. Lancet 348: 977– 980, 1996 |
|
Jick H, Derby LE, Myers MW et al: Risk of hospital admission for idiopathic venous thromboembolism among users of postmenopausal oestrogens. Lancet 348: 981– 983, 1996 |
|
Grodstein F, Stampfer MJ, Goldhaber SZ et al: Prospective study of exogenous hormones and risk of pulmonary embolism in women. Lancet 348: 983– 987, 1996 |
|
Gutthann S, Rodriguez L, Castellsague J, Ollart A: Hormone replacement therapy and risk of venous thromboembolism: population based case-control study. BMJ 314: 796– 800, 1997 |
|
The Writing Group for the PEPI Trial: Effects of estrogen or estrogen/progestin regimens on heart disease risk factors in postmenopausal women: the Postmenopausal Estrogen/Progestin Interventions (PEPI) Trial. JAMA 273:199–208, 1995 |
|
Grady D, Hulley SB, Furberg C: Venous thromboembolic events associated with hormone replacement therapy [Letter to the editor]. JAMA 278: 477, 1997 |
|
Silvertolpe G, Gustafson A, Samsioe G, Svanborg A: Lipid metabolic studies in oophorectomized women. Effects of three different progestogens. Acta Obstet Gynecol Scand Suppl 88: 89, 1979 |
|
King RJB, Whitehead MI: Assessment of the potency of orally administered progestins in women. Fertil Steril 46: 1062, 1986 |
|
Hirvonen E, Malkonen N, Manninen V: Effects of different progestogens on lipoproteins during postmenopausal replacement therapy. N Engl J Med 304: 560, 1981 |
|
Jensen J, Nilas L, Christiansen C: Cyclic changes in serum cholesterol and lipoproteins following different doses of combined postmenopausal hormone replacement therapy. Br J Obstet Gynaecol 93: 613, 1986 |
|
Ottosson UB, Johansson BG, von Schoultz B: Subfractions of high-density lipoprotein cholesterol during estrogen replacement therapy: A comparison between progestogens and natural progesterone. Am J Obstet Gynecol 151: 746, 1985 |
|
Gerhard M, Ganz P: How do we explain the clinical benefits of estrogen? From bedside to bench. Circulation 92: 5– 8, 1995 |
|
Sullivan JM: Hormone replacement therapy in cardiovascular disease: The human model. Br J Obstet Gynaecol 103 (Suppl 13): 50– 57, 1996 |
|
Koh KK, Mincemoyer R, Bui MN et al: Effects of hormone replacement therapy on fibrinolysis in postmenopausal women. N Engl J Med 336: 683– 690, 1997 |
|
Reis SE, Gloth ST, Blumenthal RS et al: Ethinyl estradiol acutely attenuates abnormal coronary vasomotor responses to acetylcholine in postmenopausal women. Circulation 89: 52– 60, 1994 |
|
Grady D, Rubin SM, Petitti DB et al: Hormone therapy to prevent disease and prolong life in postmenopausal women. Ann Intern Med 117: 1016, 1992 |
|
Henderson BE, Ross RK, Lobo RA et al: Re-evaluating the role of progestogen therapy after the menopause. Fertil Steril 49 (Suppl): 9S, 1988 |
|
Campbell S: Double-blind psychometric studies on the effects of natural estrogens on postmenopausal women. In Campbell S (ed): The Management of the Menopausal and Postmenopausal Years, p 149. Baltimore: University Park Press, 1976 |
|
Klaiber EI, Broverman DM, Vogel W et al: Effects of estrogen therapy on plasma MAO activity and EEG during responses of depressed women. Am J Psychiatry 128: 1492, 1972 |
|
Smith DC, Prentice R, Thompson DJ, Hermann WL: Association of exogenous estrogens and endometrial cancer. N Engl J Med 293: 1164, 1975 |
|
Ziel HK, Finkle WD: Increased risk of endometrial carcinoma among users of conjugated estrogens. N Engl J Med 293: 1167, 1975 |
|
Antures CMG, Stolley PD, Rosenshein NB et al: Endometrial cancer and estrogen use: Repeat of a large case controlled study. N Engl J Med 300: 9, 1979 |
|
Weiss NS, Szekeley D. English D, Schneld A: Endometrial cancer in relation to patterns of menopausal estrogen use. JAMA 242: 261, 1979 |
|
The Writing Group for the PEPI Trial: Effects of hormone replacement therapy on endometrial histology in postmenopausal women. JAMA 275: 370– 375, 1996 |
|
Nyholm HC, Nielsen AI, Norup P: Endometrial cancer in postmenopausal women with and without previous estrogen replacement treatment: Comparison of clinical and histopathological characteristics. Gynecol Oncol 29: 299, 1993 |
|
Collins J, Donner A, Allen LTT et al: Oestrogen use and survival in endometrial cancer. Lancet 2: 961, 1980 |
|
Gambrell DR: The menopause: Benefits and risks of estrogen-progesterone replacement therapy. Fertil Steril 37: 457, 1982 |
|
Gambrell RD, Massey FM, Castaneda TA et al: Use of progesterone challenge test to reduce the risk of endometrial cancer. Obstet Gynecol 55: 732, 1980 |
|
Gambrell RD Jr, Bagnell CA, Greenblatt RB: Role of estrogens and progesterone in the etiology and prevention of endometrial cancer: A review. Am J Obstet Gynecol 146: 696, 1983 |
|
Ettinger B, Selby JV, Citron JT et al: Gynecologic complications of cyclic estrogen progestin therapy. Maturitas 17: 197, 1993 |
|
Tseng L, Gurpide E: Effect of progestins on estradiol receptor level in human endometrioma. J Clin Endocrinol Metab 41: 402, 1975 |
|
Tseng L, Gurpide E: Induction of human estradiol dehydrogenase by progesterone. Endocrinology 97: 828, 1975 |
|
Pack BA, Tovar R, Book E, Brooks SC: The cyclic relationship of estrogen sulfurylation to the nuclear receptor level in human endometrial curetting. J Clin Endocrinol Metab 48: 420, 1979 |
|
Whitehead MI, Townsend PT, Pryse-Davies J et al: Effect of estrogens and progestins on the biochemistry and morphology of the postmenopausal endometrium. N Engl J Med 305: 1599, 1981 |
|
Woodruff JD, Pickar JH et al: Incidence of endometrial hyperplasia in postmenopausal women taking conjugated estrogens (Premarin) with medroxyprogesterone acetate or conjugated estrogens alone. Am J Obstet Gynecol 175 (5 Pt 1):1213, 1994 |
|
Sturdee DW, Wade-Evans T, Paterson EM et al: Relations between bleeding pattern, endometrial histology, and estrogen treatment in menopausal woman. Br Med J 1: 1575, 1978 |
|
Hoover R, Gray LA, Cole P, MacMahon B: Menopausal estrogens and breast cancer. N Engl J Med 295: 401, 1976 |
|
Ross RK, Paganini-Hill A, Gerkins VR et al: A case control study of menopausal estrogen therapy and breast cancer. JAMA 243: 1635, 1980 |
|
Hammond CB, Jelovsek FT, Lee KL et al: Effects of long term estrogen replacement therapy. II. Neoplasia. Am J Obstet Gynecol 133: 537, 1979 |
|
Wynder EL, MacCormack FA, Stellman SD: The epidemiology of breast cancer in 785 United States Caucasian women. Cancer 41: 2341, 1978 |
|
Kaufman DW, Miller DR, Rosenberg L et al: Noncontraceptive estrogen use and the risk of breast cancer. JAMA 252: 63, 1984 |
|
Bergkvist L, Adami HO, Persson I et al: The risk of breast cancer after estrogen and estrogen-progestin replacement. N Engl J Med 321: 293, 1989 |
|
Bergkvist L, Adami HO, Persson I et al: Prognosis after breast cancer diagnosis in women exposed to estrogen and estrogen-progestogen replacement therapy. Am J Epidemiol 130: 221, 1989 |
|
Hulka BS, Chambless LE, Deubner DC, Wilkinson WE: Breast cancer and estrogen replacement therapy. Am J Obstet Gynecol 143: 638, 1982 |
|
Gambrell RD Jr: Breast disease in postmenopausal years. Semin Reprod Endocrinol 1: 27, 1983 |
|
Gambrell RD, Vasquez JM: Estrogen therapy and breast cancer—Is the verdict in? Contemp Obstet Gynecol 19: 38, 1982 |
|
Nachtigall LE, Nachtigall RH, Nachtigall RD, Beckman EM: Estrogen replacement therapy. II. A prospective study in the relationship to carcinoma and cardiovascular and metabolic problems. Obstet Gynecol 54: 74, 1979 |
|
Armstrong BK: Estrogen therapy after menopause—Boon or bane? Med J Aust 148: 213, 1988 |
|
Dupont WE, Page DL: Menopausal estrogen replacement therapy and breast cancer. Arch Intern Med 151: 67, 1991 |
|
Hulka BS: Hormone replacement therapy and the risk of breast cancer. CA Cancer J Clin 40: 289, 1990 |
|
Steinberg KK, Thacker SB, Smith SJ et al: A meta-analysis of the effect of estrogen replacement therapy on the risk of breast cancer. JAMA 265: 1985, 1991 |
|
Sillero-Arenas M, Delgado-Rodriguez M, RodriguesCanteras R et al: Menopausal hormone replacement therapy and breast cancer: A meta-analysis. Obstet Gynecol 79: 286, 1992 |
|
Collaborative Group on Hormonal Factors in Breast Cancer: Breast cancer and hormone replacement therapy: collaborative reanalysis of data from 51 epidemiological studies of 52,705 women with breast cancer and 108,411 women without breast cancer. Lancet 350:1047–1059, 1997 |
|
Boston Collaborative Drug Surveillance Program. Boston University Medical Center: Surgically confirmed gall bladder disease versus thromboembolism and breast tumors in relation to postmenopausal estrogen therapy. N Engl J Med 190:15, 1974 |
|
Grodstein F, Colditz GA, Stampfer MJ: Postmenopausal hormone use and cholecystectomy in a large prospective study. Obstet Gynecol 83: 5, 1994 |
|
The Writing Group for the PEPI Trial: Effects of estrogen or estrogen/progestin regimens on heart disease risk factors in postmenopausal women. JAMA 273:199–208, 1995 |
|
Troisi RJ, Speizer FE, Willett WC et al: The Menopause, postmenopausal estrogen preparations and the risk of adult onset asthma, a prospective cohort study. Am J Respir Crit Care Med 4: 1183– 1188, 1995 |
|
Sanchez-Guerrero JS, Liang NH, Karlson EW et al: Postmenopausal estrogen therapy and the risk for developing systemic lupus erythematosus. Ann Intern Med 122: 430–433 |
|
Zemlickis D, Lishner M, Degendorfer P et al: Maternal and fetal outcome after breast cancer in pregnancy. Am J Obstet Gynecol 166: 781– 787, 1992 |
|
Nugent P, O'Connell: Breast cancer and pregnancy. Arch Surg 120: 1221– 1224, 1985 |
|
Riberio G, Jones DA, Jones M: Carcinoma of the breast associated with pregnancy. Br J Surg 73: 607– 609, 1986 |
|
Schlesielman JJ: Cancer of the breast and reproductive tract in relation to use of oral contraceptives. Contraception 40: 1– 38, 1989 |
|
Romieu I, Berlin JA, Colditz G: Oral contraceptives and breast cancer: Review and meta-analysis. Cancer 66: 2253– 2263, 1990 |
|
Stanford JL, Brinton LA, Hoover RN: Oral contraceptives and breast cancer: Results from an expanded case-control study. Br J Cancer 60: 375– 381, 1989 |
|
Stoll BA, Parbhoo S: Treatment of menopausal symptoms in breast cancer patients. Lancet 1: 1278– 1279, 1988 |
|
Wile AG, Opfell RW, Margileth DA: Hormone replacement therapy in previously treated breast cancer patients. Am J Surg 165: 372– 375, 1993 |
|
Eden JA, Bush T, Nand S, Wren BG: A case-control study of combined continuous estrogen-progestin replacement therapy among women with a personal history of breast cancer. Menopause 2: 67– 72, 1995 |
|
Guinee VF, Olson H, Möller T et al: Effect of pregnancy on prognosis for young women with breast cancer. Lancet 343: 1587– 1589, 1994 |
|
Spicer D, Pick MC, Henderson BE: The question of estrogen replacement therapy in patients with a prior diagnosis of breast cancer. Oncology 4: 49– 54, 1990 |
|
Love RR, Mazess RB, Barden HS et al: Effects of tamoxifen on bone mineral density in postmenopausal women with breast cancer. N Engl J Med 326: 852– 856, 1992 |
|
Love RR, Newcomb PA, Wiebe DA et al: Effects of tamoxifen therapy on lipid and lipoprotein levels in postmenopausal patients with node-negative breast cancer. J Natl Cancer Inst 82: 1327– 1332, 1990 |
|
Dewar JA, Horobin JM, Preece PE et al: Long-term effects of tamoxifen on blood lipid values in breast cancer. Br Med J 305: 225– 226, 1992 |
|
McDonald CC, Stewart HJ: Fatal myocardial infarction in the Scottish adjuvant tamoxifen trial. Br Med J 303: 435– 437, 1991 |
|
Smith P, Heimer G, Kindskog M, Ulmsten V: Oestradiol-releasing vaginal ring for treatment of urogenital atrophy. Maturitas 16: 145– 54, 1993 |
|
Lauritzen CH: The female climacteric syndrome, significance, problems: Treatment. Acta Obstet Gynecol Scand Suppl 51: 47, 1976 |
|
Hammond CB, Ory SJ: Endocrine problems in the menopause. Clin Obstet Gynecol 25: 19, 1982 |
|
Christiansen C, Christiansen MS, Grande P et al: Low risk lipoprotein pattern in postmenopausal women on sequential oestrogen/progestogen treatment. Maturitas 5: 193, 1984 |
|
Maxson WS, Hargrove JT: Bioavailability of oral micronized progesterone. Fertil Steril 44: 622, 1985 |
|
Saarikoski S, Yliskoski M, Penttila I: Sequential use of norethindrone and natural progesterone in premenopausal bleeding disorders. Maturitas 12: 89, 1990 |
|
Weinstein L: Efficacy of a continuous estrogen-progestin regimen in the menopausal patient. Obstet Gynecol 69: 929, 1987 |
|
Prough SG, Aksel S, Wiebe RH, Shepherd J: Continuous estrogen/progestin therapy in menopause. Am J Obstet Gynecol 157: 1449, 1987 |
|
Whitehead MI, Fraser D: Controversies concerning the safety of estrogen replacement therapy. Am J Obstet Gynecol 156: 1313, 1987 |
|
Leather AT, Javvas M, Studd WW: Endometrial histology and bleeding patterns after 8 years of continuous combined estrogen and progestogen therapy in postmenopausal women. Obstet Gynecol 78: 1008, 1991 |
|
Goodman L, Awwad J, Marc K, Schiff I: Continuous combined hormonal replacement therapy and the risk of endometrial cancer—preliminary report. Menopause 1: 57, 1994 |
|
Comerci JT, Fields AL, Rumowica CD et al: Continuous low-dose combined hormone replacement therapy and risk of endometrial cancer. Gynecol Oncol 64: 425– 430, 1997 |
|
Ettinger B, Selby J, Citron JT et al: Cyclic hormone replacement therapy using quarterly progestin. Obstet Gynecol 83: 693, 1994 |
|
Podwick ML, Pryse-Davies J, Whitehead MI: A simple method for determining the optimal dosage of progestin in postmenopausal women receiving estrogens. N Engl J Med 315: 930, 1986 |
|
Weinstein MC, Schiff I: Cost effectiveness of hormonal replacement therapy in menopause. Obstet Gynecol Surv 38: 445, 1983 |
|
Hemminki E, Silvro S: A review of postmenopausal hormone therapy recommendations: Potential for selection bias. Obstet Gynecol 52: 1021, 1993 |
|
Col NF, Eckman MH, Karas RH et al: Patient-specific decisions about hormone replacement therapy in postmenopausal women. JAMA 277: 1140– 1147, 1997 |