Authors
INTRODUCTION
Surgical sterilization continues to be the most frequently used method of contraception among men and women in the United States. Approximately 1 million procedures are performed yearly.1,2 Nearly 40% of married couples have chosen this method of contraception.3 By 1990, more than 8 million tubal sterilizations had been performed.4 With such large numbers of women seeking this form of contraception, it is estimated that approximately 6% will seek information regarding reversal of tubal sterilization,4 and approximately 5000 women actually will have the reversal procedure performed each year.5 In general, patients who reevaluate their decision for sterilization and again desire to reproduce underwent sterilization at a younger age (30 years or younger), had the procedure after a miscarriage, have fewer children, or have a change in marital status.4,6,7
CANDIDATES FOR REVERSAL OF TUBAL STERILIZATION
Before 1978, reversal of sterilization had only one option: surgical tubal anastomosis. However, with the advent of and improvement in conception through in vitro fertilization (IVF), patients now have a choice regarding how they will attempt conception. Factors that must be considered include patient age, method of sterilization, financial resources, and patient preference.
Age is an important consideration in calculating the prognosis of the chance of conception. Pregnancy rates with IVF markedly decrease after age 39 years (12% versus 21% for those 39 and younger per cycle).8 Interestingly, Trimbos-Kemper9 showed a 45% intra-uterine pregnancy rate in 78 women between 40 and 45 years of age after reversal of tubal sterilization in the mean time interval of 5.5 months from surgery. This finding supports the recommendation of surgery over IVF in this patient population.
Another factor that should be taken into account when counseling patients for reversal of tubal sterilization is the method of sterilization that was employed. Reversal of tubal sterilization tends to be more successful if the sterilization was performed using the Pomeroy or Falope ring techniques rather than other more tissue-destructive procedures such as coagulation or the Uchida technique.10 Through life table methods, Rock and colleagues11 estimated a cumulative probability of pregnancy after reversal of Falope ring sterilization of 28.4%, 48.8%, 69.3%, and 87.2% at 6, 12, 24, and 36 months after the reversal surgery, respectively. This finding compares with 22.7%, 37.8%, 52.4%, and 57.9% cumulative probability of pregnancy after 6, 12, 24, and 36 months after reversal of monopolar cautery sterilization, respectively (Table 1).11 Patients whose final tubal length is less than 4 cm and who have marked luminal discrepancy tend to have lower success rates. Sterilization procedures that involve the use of clips, rings, or Pomeroy midsegment resection allow for longer, less damaged tubal segments than do coagulation techniques.
Table 1. Cumulative probability of pregnancy after tubal reanastomosis*
Method of Sterilization | Time After Procedure (mo) | |||
6 | 12 | 24 | 36 | |
Falope ring | 28.4 | 48.8 | 69.3 | 87.7 |
Monopolar cautery | 22.7 | 37.8 | 52.4 | 57.9 |
* Patients who had sterilization performed with Falope ring had a higher pregnancy rate than those who had monopolar electrocautery.
Patient age and existing anatomy are important determinants of success after reversal of tubal sterilization, but financial considerations may govern the patient's decision between IVF and surgical reversal of tubal ligation. Although improvements have occurred in insurance coverage for assisted reproduction, most assisted reproductive procedures remain non-reimbursed. For some patients, the alternative of tubal reversal, with its one-time fee, may be preferred over the high cost incurred through multiple IVF attempts. Conversely, some patients may prefer the nonoperative approach of IVF over surgical reversal. IVF is performed under sedation rather than with general anesthesia.
PREOPERATIVE EVALUATION
Pregnancy requires three basic criteria: sperm, oocyte, and the ability of gametes to meet. Obviously, patients desiring pregnancy after sterilization lack the last element. However, it cannot be assumed that all other factors necessary for pregnancy exist simply because one is lacking. Therefore, patients undergoing tubal sterilization reversal procedures should have a basic infertility evaluation. This preoperative evaluation can include a variety of tests.
Sperm availability can be evaluated with basic semen analysis testing. Functional assays for sperm quality can include the sperm penetration assay or the hemizona-binding assay12, 13 if the basic semen analysis finding is abnormal.
Egg availability can be assessed by basal body temperature (BBT) records, luteinizing hormone testing, endometrial biopsy, or serum progesterone values.14, 15, 16, 17 BBT charting is inexpensive, easy, and suggests impending ovulation if the temperature tracing is biphasic.14 Luteinizing hormone testing can be performed using urine or serum. This method provides a reasonably accurate assessment of ovulatory cycles and is most easily done with the use of hormone colorimetric urine testing kits;15 however, this method is considerably more expensive than BBT charting. Histologic evidence can be used to document ovulation by performing a late-luteal-phase endometrial biopsy. If this method is used, the biopsy should be performed 1–2 days before the onset of menses. Serum progesterone testing also can be used to verify that ovulation has occurred. In general, if the serum progesterone level in the midluteal phase is greater than 3 ng/dl,16 ovulation has taken place, and a functional corpus luteum is present. However, serum progesterone level alone is not adequate evidence of the quality of the corpus luteus.17
Finally, before surgery is scheduled for reversal of tubal sterilization, hysterosalpingography (HSG) and laparoscopy should be performed to assess the likelihood of a successful procedure. HSG will allow the surgeon to assess the proximal fallopian tube segment. Cornual obstruction can result in considerably more difficult surgery. Laparoscopy allows the surgeon to visualize the length of the distal segments as well as the status of the fimbria. In general, the greatest success in achieving pregnancy after reversal of tubal sterilization procedures is experienced with isthmic-isthmic anastomosis, followed in decreasing order by cornual-isthmic, isthmic-ampullary, and ampullary-ampullary anastomoses (Table 2).18
Table 2. Pregnancy rates for tubal reanastomosis at various sites
Type of Anastomosis | Intrauterine Pregnancies (%) |
Isthmic-isthmic | 75 |
Cornual-isthmic | 70 |
Isthmic-ampullary | 64 |
Ampullary-ampullary | 57 |
If egg or sperm availability is questionable, or if tubal segments or fimbria are in poor condition, the couple should be evaluated further or offered the alternative of IVF. It is important to keep the best interest of the patient in mind, and recommendations should be based on the most practical, efficacious, and cost-effective method of conception for the couple.
SURGICAL TECHNIQUE
Reversal of tubal sterilization can be performed by reanastomosis of the two obstructed segments. Tubal reanastomosis is classified according to the anatomic location of tubal damage and surgical site: cornual-isthmic, isthmic-isthmic, isthmic-ampullary, ampullary-ampullary, and ampullary-infundibular.
Gynecologists who are interested in performing reversals of tubal sterilization must emphasize microsurgical principles. This approach involves adopting a philosophy of minimizing tissue trauma during surgery and keeping current regarding knowledge of new instruments, materials, and techniques. The gynecologist also must be able to provide adequate exposure of the pelvis, magnification of tissue, and irrigation of tissue; perform appropriate hemostasis; use microsurgical instruments and fine nonreactive sutures; and avoid permanent stents or other foreign bodies.
Exposure of Surgical Fields
A Pfannenstiel skin incision is recommended for this type of surgery unless a previous midline incision has been performed. The size of the incision is determined during the survey laparoscopy and depends on the mobility of the uterus and adnexa as well as the weight of the patient. In most patients, it is possible to elevate the adnexa or even exteriorize the uterus and tubes, as suggested by Silva and associates,19 through a small (5–6 cm) mini-laparotomy incision. In most instances a retractor is not needed, because the uterus and moist packs around it separate the skin surfaces.
Magnification
We prefer to use a microscope for reversal of tubal sterilization, with magnification varying between 4× and 10×. Loupes can be used, but any head motion causes defocusing and makes the procedure much more cumbersome. Most microsurgeons agree that the use of the microscope in these procedures yields higher pregnancy rates than the use of surgical loupes.20, 21, 22
Irrigation
Constant irrigation keeps the tissue moist, thus avoiding dryness and potential trauma with future adhesion formation; it also aids in the identification of small bleeders for cauterization. We use heparinized lactated Ringer's solution in 30-ml syringes with a 25-gauge needle catheter. This method allows for a pinpoint directed flow of solution, which aids in identifying bleeding areas.
Hemostasis
The use of a bipolar coagulator is essential to minimize tissue trauma and avoid the use of numerous sutures. The use of microforceps with bipolar coagulation capabilities is recommended. Unipolar microelectrodes also are helpful for hemostasis, and they can be used for any necessary excision of tissue, such as adhesions.
Microsurgical Instruments
In addition to bipolar forceps, other key instruments include tissue microforceps with and without teeth, a microneedle electrode, iris scissors, and fine microsurgical scissors. The use of glass, quartz, or plastic rods is helpful for tissue retraction when adhesions are present. Quartz rods are recommended as backstops for adhesiolysis when a CO2 laser is used, because they are not as fragile as glass.
Suture Materials and Needles
The use of absorbable 8-0 and 9-0 polyglactin (Vicryl) or polydioxanone (PDS) sutures are recommended because they provoke less tissue reaction and possible fibrosis than do nylon or catgut. The needle most often used is a taper-cut, 3/8 inch circle with an overall length of 3–5 mm.
Technique of Reanastomosis
A pediatric Foley catheter is placed in the uterine cavity before a Pfannenstiel incision is made. This catheter is connected to intravenous tubing and a 20-ml syringe containing diluted indigo carmine dye. This equipment greatly facilitates the surgery because chromopertubation can be performed by the surgeon as needed during the procedure. This procedure allows the surgeon to assess tubal segment patency before reanastomosis, leakage of the reanastomosis site, and final tubal patency.
With the patient in the dorsal supine position, a Pfannenstiel incision large enough to allow adequate exposure of the uterus and tubes is made. A retractor is placed, and the bowel is packed with several moist laparotomy sponges. Care must be taken not to include distal tubal segments during the initial bowel packing. The uterus and adnexa are elevated by placing moistened laparotomy sponges in the cul-de-sac and fixed by placing another sponge anteriorly in the vesicouterine pouch. Sponges may be placed within a washed surgical glove to avoid drying during long surgical procedures. The goal is to elevate the adnexal structures so that the fallopian tubes have adequate exposure with minimal mobility and are as close to the plane of the abdominal surface as possible.
ISTHMIC-ISTHMIC REANASTOMOSIS
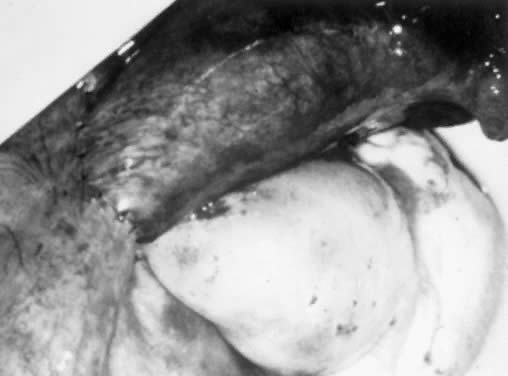
The first step in tubal reanastomosis is preparation of the two segments of fallopian tubes. After the area of occlusion, whether a ring, clip, or cauterized area, is excised with straight, fine, iris-type scissors, both ends of the adjoining tube are cut transversely to allow patency. This procedure usually involves removal of approximately 0.5 cm from the obstructed ends of the tube, or as much tubal tissue as necessary until adequate patency is observed. Hemostasis is achieved with a bipolar coagulator or microelectrode or, if necessary, a 6-0 Vicryl suture for the mesosalpinx. Patency of the proximal end of the tube is evaluated using the previously placed intrauterine pediatric catheter. Similarly, the adjoining distal segment of the tube is prepared, and patency is checked. The use of a lacrimal probe that is fed gently through the fimbrial end or, alternatively, an 18-gauge angiocatheter, can help to delineate the area of occlusion for more accurate excision of tissue. It also can be used for distal irrigation to confirm patency. If patency of both segments is not adequate, or if the tissue does not appear viable (e.g. it is white or fibrotic), it may be necessary to excise another 0.5–1 cm segment of tube until this tissue appears pink and bleeds easily, and the surgeon is comfortable with the quality of the tissue and the patency. Irrigation can help to identify small bleeders, which are then controlled using cautery. A 2-0 nylon splint is then fed into the proximal and distal segments of the fallopian tube.
Before the actual reanastomosis is performed, the mesosalpingeal defect is approximated with sutures of 6-0 material such as Vicryl or PDS and placed correctly to align both lumens. Two stay sutures are placed at the junction between the mesosalpinx and the 6-o'clock portion of the tubes that are about to be approximated. The sutures are held with a small hemostat and tied after the first muscular suture at the 6-o'clock position is placed. The purpose of these stay sutures is to decrease tension on the reanastomotic site. Additional sutures incorporating only the muscular layer follow at the 3-, 9-, and 12-o'clock positions. PDS or Vicryl material is used (Fig. 1). The use of a microscope facilitates accurate placement of the sutures. The serosal layer is approximated in a circumferential manner, using as many interrupted 8-0 or 9-0 sutures as needed (see Fig. 1). In the past, the splint was removed through the cervix several days after the procedure. The need for this procedure can be avoided by gently removing the splint with atraumatic forceps before placing the 12-o'clock suture. The same procedure is repeated on the opposite tube.
{kind=link}
ISTHMIC-AMPULLARY REANASTOMOSIS
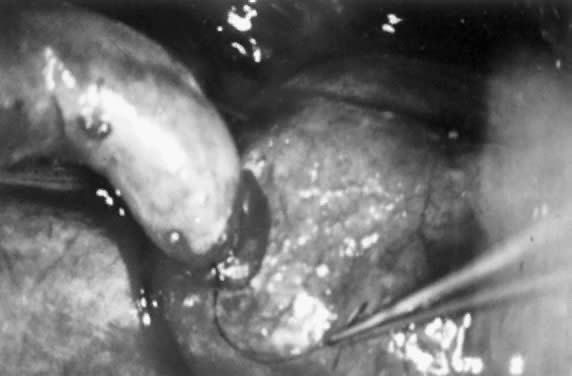
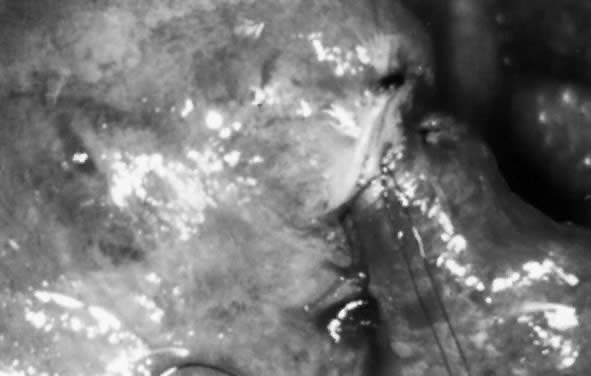
Because the ampulla is greater in diameter than the isthmus, it is important to prepare the lumens carefully to avoid significant luminal disparity. This preparation can be done in two ways. One option is to enlarge the isthmic diameter by cutting a slit anteriorly, on the antimesenteric side, to create a fish-mouth opening. Alternatively, the ampullary stump can be cut so that the diameter approximates that of the isthmic side (Figs. 2 and 3). This procedure is done by stretching the stump end with a lacrimal probe and taking small-diameter cuts until patency is reached (Figs. 4 and 5). A two-layer reanastomosis is performed in a similar fashion to that at the isthmic-isthmic site (Fig. 6).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
AMPULLARY-AMPULLARY REANASTOMOSIS
The primary difficulty with ampullary-ampullary reanastomosis is that the muscularis is thin, and the mucosal folds tend to prolapse. It may be necessary to push the mucosal folds gently inward instead of resecting them. A two-layer reanastomosis is then performed. Because the diameter is large compared with that of the much smaller isthmus, it often is necessary to place more sutures than usual to approximate the lumens.
CORNUAL-ISTHMIC REANASTOMOSIS
The surgical treatment of cornual occlusion by uterotubal implantation has been replaced by cornual-isthmic reanastomosis because of its superior postreversal pregnancy rates of 46–69%.23, 24, 25, 26, 27, 28 The technique involves preparation of the isthmic portion of the tube similar to that with isthmic-isthmic reanastomosis, with some modification of the cornual side. With a small blade, such as a no. 15 Bard-Parker scalpel, the cornual region is shaved serially. One-millimeter slices are removed until patency is shown (Figs. 7 and 8). Bleeding areas are controlled, preferably by microbipolar cautery, to minimize tissue injury. After the stay sutures of 6-0 Vicryl are placed to align the lumens, a two-layer reanastomosis is performed (Fig. 9). A splint is used, but it is removed at the end of the procedure. A cornual-ampullary reanastomosis is more difficult than a cornual-isthmic procedure because of the large discrepancy in lumen diameter of the ampulla. The best recommendation is to make the ampullary diameter as small as possible, as recommended for the isthmic-ampullary reanastomosis.
{kind=link}
{kind=link}
{kind=link}
POSTOPERATIVE MANAGEMENT
Patients are seen for a routine postoperative check within 3–4 weeks postoperatively. Pregnancy may be attempted after one normal menstrual cycle. Patients are advised to chart their cycles carefully. Ovulation-stimulating agents are recommended if cycles are irregular. If, after 4–6 months of timed intercourse, the patient is not pregnant, a follow-up HSG is performed to document the persistence of tubal patency. We do not recommend routine HSG testing.
RESULTS
Results after tubal reanastomosis are gratifying, with pregnancy rates ranging from 44% to as high as 81%.20,29 In our patients, there have been 15 pregnancies in the last 20 procedures (75%). Of the 5 patients who did not become pregnant, 3 were 40 years or older when the procedure was performed, and 2 had tubal lengths less than 5 cm. In addition to age and tubal length, another variable that can affect pregnancy rate is the anatomic site of reanastomosis. Most authors report the highest pregnancy rate with isthmic-isthmic reanastomosis, followed by cornual-isthmic reanastomosis. The lowest pregnancy rate is achieved with ampullary-ampullary reanastomosis. After reanastomosis, pregnancy usually occurs within the first year of follow-up. Although the abortion rate is not greater than that in women with normal fallopian tubes who conceive, patients are counseled preoperatively about a possible elevated rate of ectopic pregnancy. A higher ectopic pregnancy rate has been described in this population, primarily when high magnification was not used.30
COMPLICATIONS OF TUBAL REANASTOMOSIS
Complications of tubal reanastomosis are similar to those of other pelvic surgery. Infection and bleeding, although rare, are possibilities. Prophylactic antibiotics with a first-generation cephalosporin will provide adequate protection; however, use of these drugs is at the discretion of the surgeon. Bleeding should be minimal because of the nature of the microsurgical technique, which uses cautery delivered with a microneedle tip.
Ectopic pregnancy is a concern after tubal reanastomosis. The results of several surgeons have been compiled by Rock.18 The rate of tubal pregnancy after more than 550 microsurgical tubal reanastomoses ranges from 1–4%. This rate is similar to the prevalence of ectopic pregnancy after IVF and embryo transfer.8
Inability to conceive after tubal reanastomosis can result from partial tubal occlusion or from subtle structural tubal disease such as ciliary dysfunction. The latter is of particular concern if electrocautery was used to perform the sterilization procedure.
RECENT DEVELOPMENTS
Cornual-isthmic obstruction can occur in patients who have not undergone sterilization. In many instances, treatment by reanastomosis has been replaced by retrograde cornual cannulation by fluoroscopic selective catheterization or hysteroscopic retrograde cannulation. The former approach seems reasonable in patients with HSG results that show cornual obstruction in whom laparoscopy is not indicated or desired.31 We feel more comfortable recommending the hysteroscopic approach because most patients undergo diagnostic laparoscopy as part of the infertility evaluation. In addition, any complications from the procedure such as perforation or bleeding can be identified and corrected immediately. With the hysteroscopic approach for tubal cannulation, Novy and associates32 catheterized and established patency in 11 of 12 fallopian tubes in 10 patients. When this approach is unsuccessful, it is reasonable to recommend resection of the obstructed area and reanastomosis.
The use of tissue adhesive material, primarily fibrin glue, has been investigated for reanastomosis. The rabbit model showed both tubal patency and pregnancies.33 It also is possible to minimize the number of sutures to one or two when fibrin glue is used.34 Although this material has been studied in Europe, it has not been approved for use in the United States. Recently, Wiegerinck and associates described a laparoscopic technique assisted by a tubal splint, fibrin glue, and two 3 mm microclips with a 55% cumulative pregnancy rate.35
As trends toward shorter hospital stays for operative procedures continue, surgeons will seek methods to apply this philosophy to tubal surgery. Already accomplished is successful outpatient tubal reanastomosis in which 12 of 17 (71%) patients achieved pregnancy with mini-laparotomy.19
Laparoscopy has become an invaluable tool for the gynecologic surgeon. This technique can be applied to tubal reanastomosis. Gauwerky and Klose36 developed a working laparoscopic model with rat uterine horns and a pelvic trainer. They established patency in 18 of 20 horns with this technique.36 This technique was used in humans by Sedbon and colleagues.37 In this study, fibrin glue was used in a laparoscopic procedure to reapproximate previously ligated fallopian tubes.37 These studies provide the possibility of laparoscopic and outpatient procedures for tubal reanastomosis.
LAPAROSCOPIC TUBAL REANASTOMOSIS
Laparoscopic tubal reanastomosis can be accomplished using specialized instrumentation that is currently available. High-resolution monitors with three-chip cameras allow excellent visualization with proper magnification. Also currently available are 3-mm grasping instruments which allow grasping of 6.0–8.0 sutures. Fine microelectrodes with a tip diameter of 100–150 microns can be introduced laparoscopically for spot coagulation, thus decreasing peripheral tissue damage caused by larger electrodes. This method of tubal reanastomosis requires multiple trocar sites and advanced laparoscopic skills by both surgeon and assistant.
The first published case report of laparoscopic tubal reanastomosis involved the use of biologic glue with subsequent tubal patency by hysterosalpingogram.37 A later report described a series of 22 patients that underwent tubal reanastomosis laparoscopically using a two-stitch technique to reapproximate the muscularis and endosalpinx. Using this technique, Reich and colleagues38 described a 35% pregnancy rate, which was significantly lower than the laparotomy approach. Major criticisms of these attempts at laparoscopic tubal reanastomosis have been extreme deviation from microsurgical technique and obvious poor pregnancy results.
Most recently, however, it was demonstrated that laparoscopic tubal reanastomosis can be performed using standard microsurgical technique with a pregnancy rate comparable to that with the conventional open method.39, 40, 41, 42 Using a two-layer technique for anastomosis with 7-0 and 8-0 sutures through the laparoscope, Koh and Janik41 described a 71% pregnancy rate in 40 consecutive patients at 12 months follow-up. In their first 10 cases, the mean operating time for tubal reversal was 6 hours, with subsequent reduction to three hours.43 Using a very similar method of two-layer laparoscopic tubal reanastomosis, Yoon and associates42 described a 77.6% pregnancy rate in 49 patients. More recently, Yoon and associates reported on 202 cases with an 87.1% pregnancy rate.44
CRITICISMS OF TUBAL REVERSAL
Although tubal reversals have been shown to be possible via laparoscopy by very few individuals, there appear to be several shortcomings to this technique. First, very few reports are available with this procedure, and most report lower pregnancy rates than those achievable by other methods. Second, there appears to be no advantage in shortening length of hospital stay or time to return to work with this technique because similar results can be accomplished using mini-laparotomy.45
Finally, laparoscopic tubal reversal requires extensive laparoscopic experience which is not necessary with mini-laparotomy. Pregnancy rates are compromised during the 'learning curve' when trying to handle the entire procedure laparoscopically. Bissonnette and associates recently described a one suture technique which may make a laporoscopic approach easier to perform. Of 102 patients in this observational, prospective study, they reported a 65% pregnancy rate.46
Thus, at this time, laparoscopic tubal reanastomosis should be considered experimental until this technique can be replicated by most fertility surgeons with pregnancy outcomes equal to those achievable using the classical mini-laparotomy approach.
ROBOTIC ASSISTED TUBAL REANASTOMOSIS
The drawbacks of laparoscopic tubal reanastomosis, mainly increased learning curve and long operating times, have led investigators to evaluate the use of robotic assistance. The robotic system has been employed since 2000. The most popular robotic system is the Da Vinci Surgical system made by Intuitive Surgical, Sunnyvale, CA. The robotic arms handle the laparoscope and accessory microsurgical graspers. They are controlled by the surgeon via a console that is located in a corner of the operating room.
The robotic system offers several advantages to the laparoscopic approach. Tying surgical knots with microsuture is performed more easily and is mastered more quickly. This is due to the utilization of a three dimensional field. This superb imaging quality also allows more precise movements that are needed to handle the small sutures, especially when applying knots. In a recent study, 26 cases of tubal reanastomosis performed by robotic assistance were compared to 41 cases of outpatient minilaparotomy by Rodgers et al.47 The mean hospitalization time, pregnancy, and ectopic rates were not significantly different in both groups. It was noted, however, that the actual surgical time and overall hospital costs were higher with the robotic assistance.
Although tubal reanastomosis can be elegantly performed by laparoscopy by a few extensively well trained individuals and can be performed by most gynecologists using robotic assistance, there are distinct disadvantages. Increased costs, increased surgical time, increased learning curve, and lack of availability of robotics to most gynecologists at this time will keep the minilaparotomy approach the most popular and sensible one.
CONCLUSIONS
As long as tubal sterilization remains popular as a form of birth control, there will be continued demand for tubal reversal. To perform this procedure efficiently and successfully, the physician must choose appropriate candidates and also must feel comfortable with microsurgical principles and technique. The surgical results of reanastomosis performed in this manner are excellent. Patients who are poor candidates for reanastomosis because of extensive tubal damage should be made aware of other options, including IVF and adoption.
REFERENCES
Association of Voluntary Surgical Contraception: The 1984 estimates of US sterilization: An extended picture. Association of Voluntary Surgical Contraception News 24:1, 1986 |
|
Destefano F, Greenspan JR, Ory HW et al: Demographic trends in tubal sterilization: United States 1970-1978. Am J Public Health 72: 480, 1982 |
|
Mosher WD: Reproductive impairments in the United States, 1965-1982. Demography 22: 415, 1985 |
|
Wilcox LS, Chu SY, Peterson HB: Characteristics of women who considered or obtained tubal reanastomosis: Results from a prospective study of tubal sterilization. Obstet Gynecol 75: 661, 1990 |
|
Diamond MP, Christianson CED, Daniell JF: Microsurgical reanastomosis of the fallopian tube: Increasingly successful outcome for reversal of previous sterilization procedures. South Med J 75: 443, 1982 |
|
Marcil-Grattin N, Duchesne C, St Germain-Roy S, Tulandi T: Profile of women who request reversal of tubal sterilization: Comparison with a randomly selected control group. Can Med J 138: 44, 1991 |
|
Ramsay IN, Russel SA: Who requests reversal of female sterilization? A retrospective study from a Scottish unit. Scott Med J 36: 44, 1991 |
|
Medical Research International Society for Assisted Reproductive Technology, the American Fertility Society: In vitro fertilization-embryo transfer (IVF-ET) in the United States: 1989 results from the IVF-ET registry. Fertil Steril 55:14, 1991 |
|
Trimbos-Kemper TC: Reversal of tubal sterilization in women over 40 years of age: A multicenter survey in the Netherlands. Fertil Steril 53: 575, 1990 |
|
Xue P, Fa Y: Microsurgical reversal of female sterilization: Long-term follow-up of 117 cases. J Reprod Med 34: 451, 1989 |
|
Rock JA, Guzick DS, Katz E et al: Tubal anastomosis: Pregnancy success following reversal of Falope ring or monopolar cautery sterilization. Fertil Steril 48: 13, 1987 |
|
Rogers BJ: The sperm penetration assay: Its usefulness reevaluated. Fertil Steril 43: 821, 1985 |
|
Burkman LJ, Coddington CC, Fraken DR et al: The hemizona assay (HZA): Development of a diagnostic test for the binding of human spermatozoa to the human hemizona pellucida to predict fertilization potential. Fertil Steril 49: 688, 1988 |
|
Shoupe D, Mishell DR Jr, Lacurra M et al: Correlation of endometrial maturation with four methods of estimating the day of ovulation. Obstet Gynecol 72: 88, 1989 |
|
Hill LM, Breckle R, Coulam CB: Assessment of human follicular development by ultrasound. Mayo Clin Proc 57: 176, 1982 |
|
Peters AJ, Lloyd RP, Coulam CB: Prevalence of out-of-phase endometrial biopsy specimens. Am J Obstet Gynecol 166: 1738, 1992 |
|
Shangold M, Berkeley A, Gray J: Both midluteal serum progesterone levels and late luteal endometrial histology should be assessed in all infertile women. Fertil Steril 40: 627, 1983 |
|
Rock JA: Reconstruction of the fallopian tube. In Mattingly RF, Thompson JD (eds): TeLinde's Operative Gynecology, 6th ed, pp 381–410. Philadelphia, JB Lippincott, 1985 |
|
Silva PD, Schaper AM, Meisch JK, Schauberger CW: Outpatient reversal of tubal sterilization by a combined approach of laparoscopy and minilaparotomy. Fertil Steril 55: 696, 1991 |
|
Gomel V: Microsurgical reversal of female sterilization: A reappraisal. Fertil Steril 33: 587, 1980 |
|
Winston RML: The future of microsurgery in infertility. Clin Obstet Gynecol 5: 607, 1978 |
|
Hedon B, Wineman M, Winston RML: Loupes or microscope for tubal reanastomosis? An experimental study. Fertil Steril 34: 264, 1980 |
|
Diamond E: A comparison of gross and microsurgical techniques for repair of cornual occlusion in infertility: A retrospective study, 1968-1978. Fertil Steril 32: 370, 1979 |
|
Fayez JA, Suliman SO: Infertility surgery of the oviduct: Comparison between macrosurgery and microsurgery. Fertil Steril 37: 73, 1982 |
|
Winston RML: Microsurgical tubocornual anastomosis for reversal of sterilization. Lancet 1: 284, 1977 |
|
Gomel V: An odyssey through the oviduct. Fertil Steril 39: 144, 1983 |
|
Seiler JC: Factors influencing the outcome of microsurgical tubal ligation reversals. Am J Obstet Gynecol 146: 292, 1983 |
|
Henderson SR: The reversibility of female sterilization with the use of microsurgery: A report on 102 patients with more than one year of follow-up. Am J Obstet Gynecol 149: 57, 1984 |
|
Donnez J, Casans-Ronx F: Prognostic factors influencing the pregnancy rate after microsurgical cornual anastomosis. Fertil Steril 46: 1089, 1986 |
|
Hodari AA, Vihasiri S, Isaac AY: Reconstructive tubal surgery for midtubal obstruction. Fertil Steril 28: 620, 1977 |
|
Platia MP, Krudy AG: Transvaginal fluoroscopic recanalization of a proximally occluded oviduct. Fertil Steril 44: 704, 1985 |
|
Novy ML, Thurmond AS, Patton P: Diagnosis of cornual obstruction by transcervical fallopian tube cannulation. Fertil Steril 50: 434, 1988 |
|
Gauwerky JFH, Kubli F, Fursman WG: Morphology and fertility after reanastomosis of the rabbit fallopian tube with fibrin glue. Hum Reprod 3: 327, 1988 |
|
Rucker K et al: Tubal reanastomosis using a tissue adhesive. Hum Reprod 3: 185, 1988 |
|
Wiegerinck MA, Roukema M, Van Kessel PH, Mol BW. Human Reproduction. 20:2355, 2005. |
|
Gauwerky JF, Klose R: An experimental model for pelviscopy tubal anastomosis. Hum Reprod 5: 439, 1990 |
|
Sedbon E, Delajolineres JB, Boudouris O, Madelenat P: Tubal desterilization through exclusive laparoscopy. Hum Reprod 4: 158, 1989 |
|
Reich H, Glynn F, Parente C, Sekel L, Levie M: Laparoscopic tubal anastomosis. J Am Assoc Gynecol Laparosc 1: 16– 9, 1993 |
|
Sung HR, Yoon TK, Cha SH, Lee CN, Cha KY: Clinical experience with laparoscopic microsurgical tubal anastomosis. J Am Gynecol Laparosc 2: 52– 3, 1995 |
|
Koh CH: Microsurgical laparoscopic tubal resection and anastomosis: Technique and results. Referenas En Gynecologic Obstetrique September(Special Issue):102–4, 1995 |
|
Koh CH, Janik GM: Laparoscopic microsurgical tubal anastomosis: Results of 40 consecutive cases [Abstract 0–060]. Fertil Steril S31, 1996 |
|
Yoon TK, Sung HR, Cha SH, Lee NC, Kwang YC: Fertility outcome after laparoscopic microsurgical tubal anastomosis. Fertil Steril 67: 18– 22, 1997 |
|
Koh CH, Janik GM: Laparoscopic microsurgical tubal anastomosis. Obstetrics and Gynecology Clinics in North America 26:189, 1999. |
|
Yoon TK, Sung HR, Kang HG, Chu SH, Lee CN, Cha KY. Laparoscopic tubal anastomosis:fertility outcome in 202 cases. Fertil Steril 72:1121, 1999. |
|
Slowey MJ, Coddington CC: Microsurgical tubal anastomoses performed as an outpatient procedure by minilaparotomy are less expensive and as safe as those performed as an inpatient procedure. Fertil Steril 69: 492– 495, 1998 |
|
Bissonnette F, Lapensee L, Bouzayen R. Outpatient laparoscopic tubal anastomosis and subsequent fertility. Fertil steril. 72(3):549, 1999. |
|
Rodgers AK, Goldberg JM, Hammel JP, Falcone T. Tubal anastomosis by robotic compared with outpatient minilaparotomy. Obstetrics and Gynecology 109:1375, 2007. |