This chapter should be cited as follows:
Pulei AN, Shatry A, et al., Glob Libr Women's Med
ISSN: 1756-2228; DOI 10.3843/GLOWM.409333
The Continuous Textbook of Women’s Medicine Series – Obstetrics Module
Volume 10
Common obstetric conditions
Volume Editor: Professor Sikolia Wanyonyi, Aga Khan University Hospital, Nairobi, Kenya
Chapter
Preterm Prelabor: Rupture of Membranes
First published: February 2021
Study Assessment Option
By answering four multiple-choice questions (randomly selected) after studying this chapter, readers can qualify for Continuing Professional Development points plus a Study Completion Certificate from GLOWM.
See end of chapter for details.

INTRODUCTION
Prelabor rupture of membranes (PROM), previously known as premature rupture of membranes, refers to spontaneous rupture of membranes at least 1 hour before the onset of uterine contractions. Preterm PROM (PPROM) refers to rupture of membranes before 37 weeks 0 days' gestation. PROM complicates 8–10% of all pregnancies. PPROM is associated with 30–40% of preterm deliveries and is the leading identifiable cause of preterm delivery. It occurs in about 1–3% of all pregnancies.1 PPROM can lead to significant perinatal morbidity associated with prematurity such as respiratory distress syndrome, neonatal sepsis, umbilical cord prolapse, placental abruption and fetal death.2 It contributes to about 20% of all perinatal deaths and is also associated with maternal morbidity. The pathogenesis and management of patients with PPROM are presented in this chapter in line with current evidence.
Terminology
Prolonged rupture of membranes is any rupture of membranes that persists for more than 24 hours and prior to the onset of labor
Previable premature rupture of membranes is rupture of membranes before viability limit, usually before 23 weeks. Complicates 0.1–0.7% of pregnancies.
Latent period is the time from membrane rupture until delivery
Expectant management: management of patients with the goal of prolonging gestation ('watchful waiting until delivery indication arises.
PATHOGENESIS
The etiology of PPROM is multifactorial. The final common pathway in the occurrence of PROM is disruption of fetal membranes. Fetal membranes are complex in structure with two components: the choriodecidua, which is relatively thick and cellular, and the amnion, which is thinner and stronger. The chorion and amnion are closely adherent consisting of several cell types, including epithelial cells, mesenchymal cells, and trophoblast cells, embedded in a collagenous matrix.3 The amnion accounts for approximately 20% of the thickness of the fetal membranes, but dominates the mechanical response of the fetal membranes.4 The physical integrity of these membranes maintains the pregnancy until term, and in a majority of women, they would only rupture after the onset of contractions or after artificial intervention during labor.
Rupture of the fetal membranes is precipitated by stretch forces acting upon biochemically mediated, pre-weakened fetal membranes.5 Fetal membranes weaken in late gestation as a result of biochemical changes involving extracellular matrix remodeling and apoptosis.6 The pre-weakening could also occur before term due to defective collagen, infections or other inflammatory processes. Acute inflammation is associated with increased proteolytic enzymes and activation of cytokines, which trigger the cascade of matrix breakdown.7 Hemorrhage in early pregnancy can cause membrane weakness as it also triggers the inflammatory cascade. Decidual hemorrhage or abruptio placenta results in decidual production of thrombin to initiate hemostasis. Like cytokines, thrombin has been demonstrated to induce dose-dependent weakening of the fetal membranes in vitro with concomitant remodeling and apoptosis which mimic that seen in the physiological weak zone of term fetal membranes.8 Increased mechanical stretch of fetal membranes may also result in loss of integrity and resultant rupture of membranes remote from term.9 Examples of conditions that could cause increased stretching of the membranes are twin gestation and polyhydramnions. Sac exposure due to isthmus–cervix incompetence may also result in PPROM, since the mechanical forces on the herniating membranes are higher, as they are concentrated on a small surface area. The herniated membranes are also exposed and have higher chance of infection.
RISK FACTORS
Although there appears to be no single etiology for PPROM, there are a number of risk factors that have been identified.10 Studies indicate that the presence of certain risk factors increase the possibility of PPROM occurrence compared with others. The factors that contribute to PPROM can be broadly classified as maternal, uteroplacental or fetal in origin (Table 1). The common factors at play include intrauterine infection, decidual hemorrhage (placental abruption), excessive uterine stretch, and maternal or fetal stress. These factors set off mechanisms that cause activation of factors and cascades that inhibit uterine quiescence which lead to PPROM.11,12
Maternal factors
|
Uteroplacental factors
|
Fetal factors
|
History of PPROM in a prior pregnancy has been a consistent risk factor for PPROM.10,11 The risk of recurrence is 16–32%, as compared with approximately 4% in women with a prior uncomplicated term delivery.14 Black women also have been shown to have increased the risk of PPROM due to the increased likelihood of placenta abruption compared to other ethnicities.15,16 Decreased collagen content is linked to it, as well as collagen vascular disorders like Ehlers-Danlos and sytemic lupus erythematosus.11 Factors resulting in uterine distension have been associated with PPROM including conditions such as multiple pregnancies and polyhydramnios. Other risk factors include chronic steroid therapy, anemia, abdominal trauma, smokers, illicit drug use, history of sexually transmitted infections, lower body mass index, procedures (cerclage and amniocentesis) and vaginal hemorrhage.
Invasive uterine procedures performed during pregnancy (such as amniocentesis, chorionic villus sampling, fetoscopy and cervical cerclage) can damage the membranes, causing them to leak, but these are rare causes of PPROM. Most cases of PPROM occur in otherwise healthy women without identifiable risk factors.11 Epidemiological and historical factors that are known not to be associated with PPROM include sexual intercourse, speculum examinations, maternal exercise and parity.13
CLINICAL FEATURES
Clinical history
Typically, a woman presents with a history of a large gush of fluid down the legs, followed by a steady trickle or a feeling of “wetness”. The color, consistency and smell are important factors to consider during history taking and examination. Other features typical in presence of chorioamnionitis include abdominal pain, fever, and a foul smelling vaginal discharge.
Examination findings
An assessment of vital signs is necessary to rule out infection. Maternal tachycardia and elevated temperature are signs of infection as well as abdominal tenderness. Palpable fetal parts could be encountered due to reduced amniotic fluid. A sterile speculum examination is essential in patients with suspected PPROM. The examiner should look for pooling of liquor in the posterior fornix. The patient can be told to cough or perform Valsalva maneuver during the speculum exam if liquor is not obviously seen to trickle out of the cervical os. If there is no pooling, vaginal fluid should be obtained for the confirmatory tests discussed below. The pool can also be collected and sent for determination of fetal lung maturity, if the gestational age is greater than 32 weeks. The pooled liquor is collected into a specimen bottle, which is then taken to the laboratory. The test done depends on what is available. There are various tests for lung maturity such as lamellar body count undertaken by a standard hematology analyser, Lecithin/Sphingomyelin ratio done on paper chromatography and foam stability index among others.
During the speculum examination, the patient’s cervix should be assessed for cervical dilatation and for the presence of cord prolapse. Cervical secretions should also be sent for culture.
It is important to rule out possible differential diagnoses from both clinical history and examination. These may include leakage of urine (urinary incontinence); excessive vaginal discharge, such as physiological discharge or bacterial vaginosis; and cervical mucus (show) as a sign of impending labor.13
DIAGNOSIS
The diagnosis of PPROM is mainly clinical. The patient usually presents with a history of leakage of fluid vaginally. This should be followed by a sterile speculum examination to document rupture of membranes by visualization of amniotic fluid pooling in the posterior fornix or clear fluid flowing from the cervical canal. Laboratory tests can then be used to confirm the clinical diagnosis or to make the diagnosis when it is uncertain. Sonographic examination is also undertaken to assess amniotic fluid volume, identify the presenting part, estimate gestational age (if not previously performed), and estimate fetal weight. The specific confirmatory tests are discussed below.
Nitrazine paper test
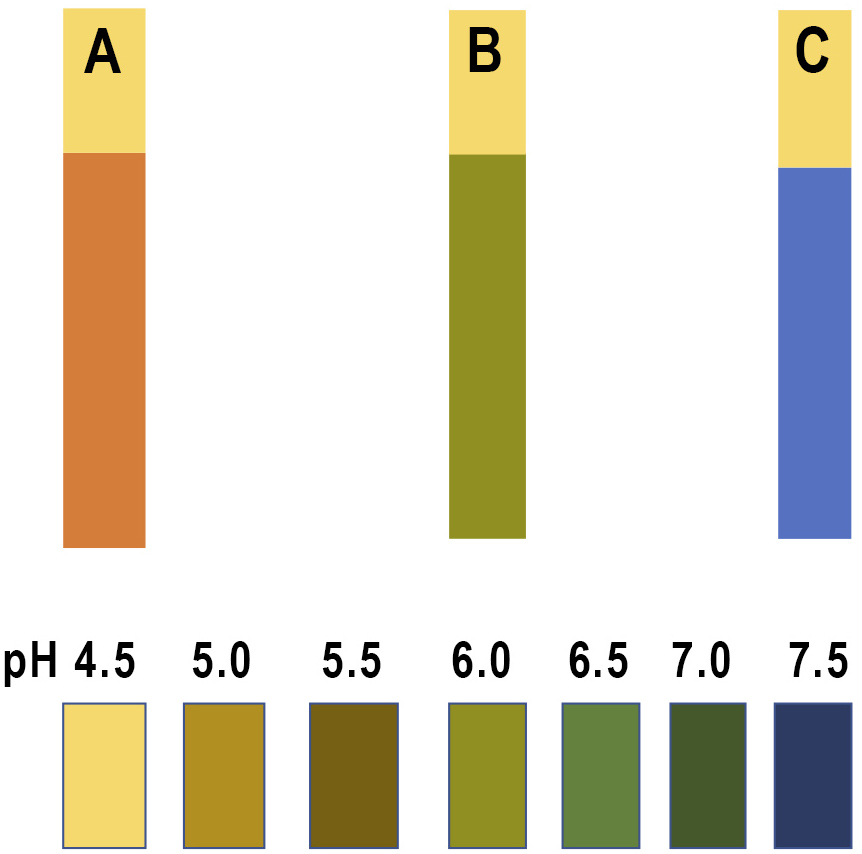
Nitrazine or phenaphthazine is a pH indicator dye. Amniotic fluid usually has a pH range of 7.0–7.3 compared with the normally acidic vaginal pH of 3.8–4.2 and the normal acidic pH of urine of 5.0–6.0.17 This test involves putting a drop of fluid obtained from the vagina onto paper strips containing nitrazine dye. The strips change color depending on the pH of the fluid. The strips will turn from yellow to blue if the pH is greater than 6.0 (Figure 1). A blue strip means it is more likely that the membranes have ruptured. False positive test results may occur with co-existent blood, semen, soap, or bacterial vaginosis, while false negatives may result from scanty amniotic fluid within the vaginal canal.
1
The nitrazine paper test: (A) normal; (B) bacterial vaginosis; (C) pregnant woman with premature rupture of membranes.
Arborization or ferning test
Fluid from the posterior vaginal fornix is swabbed onto a glass slide and allowed to dry for at least 10 minutes. Amniotic fluid produces a delicate ferning pattern, in contrast to the thick and wide arborization pattern of dried cervical mucus.18 Well-estrogenized cervical mucus or a fingerprint on the microscope slide may cause a false-positive fern test. False negatives may occur due to inadequate amniotic fluid on the swab or heavy contamination with vaginal discharge or blood.
AmniSure
AmniSure is a rapid slide test that uses immunochromatography methods to detect trace amounts of placental alpha microglobulin-1 (PAMG-1) protein in vaginal fluid. The concentration of this protein in amniotic fluid is 1,000–10,000 times higher than in cervicovaginal fluid.19 Consequently, the presence of high concentrations of PAMG-1 in cervicovaginal fluid is considered evidence of rupture of membranes, and the threshold of the test for the diagnosis has been set at 5.0 ng/mL. AmniSure test is not expected to be positive when fetal membranes are intact since the concentration of PAMG-1 in cervical vaginal secretions is less than 0.25 ng/mL. The sensitivity and specificity of PAMG-1 test in the diagnosis PROM are 97.3% and 98.7%, respectively.20 One of the advantages of this test is the fact that it is not affected by semen or trace amounts of blood within the vaginal canal.
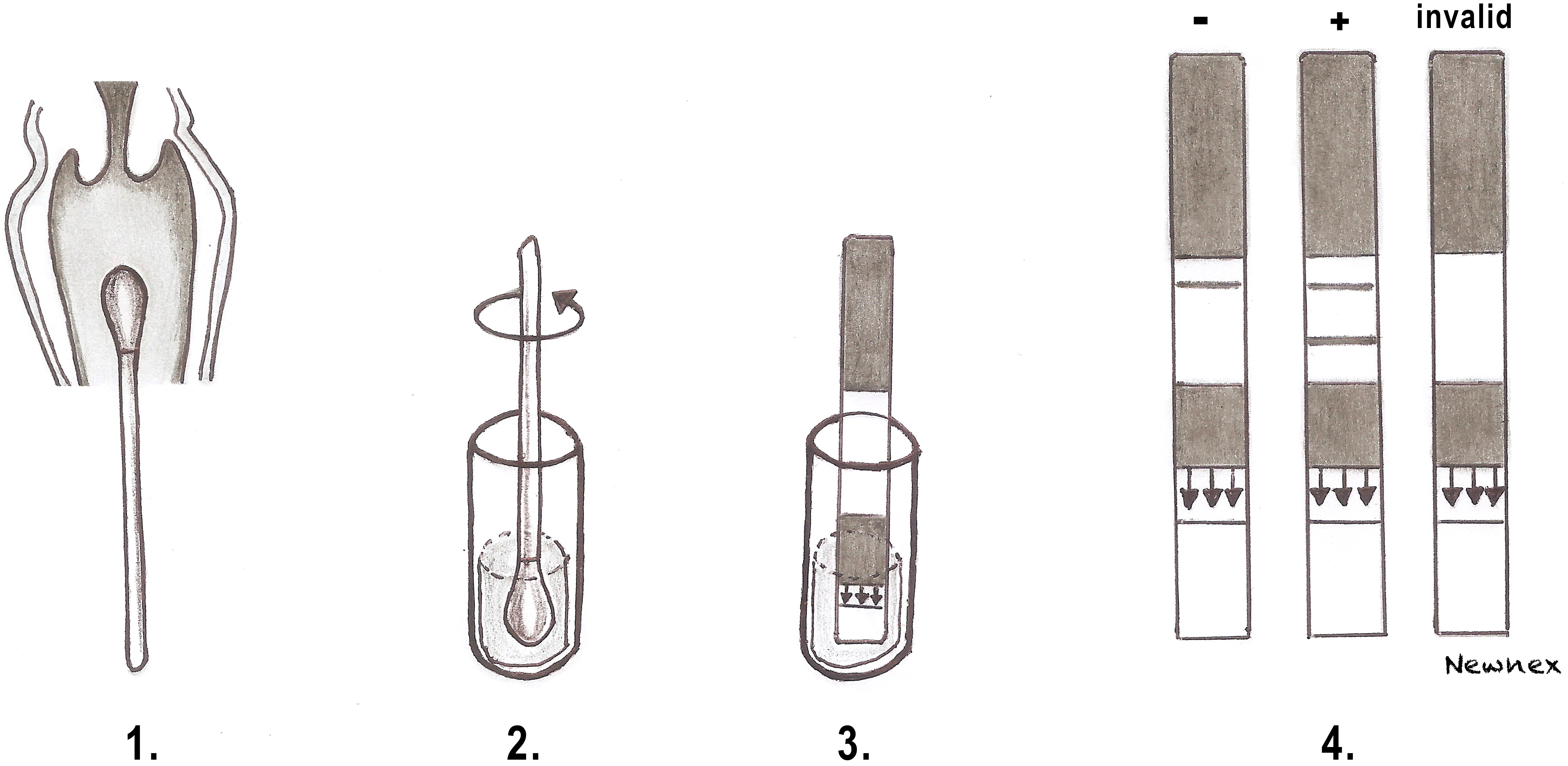
Steps in carrying out the AmniSure test:
- A sterile swab is inserted into the vagina for 1 minute, and then placed into a vial containing a solvent for 1 minute;
- AmniSure test strip is dipped into the vial;
- The test result is revealed by the presence of one or two lines within the next 5–10 minutes. One visible line means a negative result for amniotic fluid, two visible lines is a positive result, and no visible line is an invalid result (Figure 2).
2
Process of the AmniSure test. (1) A sterile swab is inserted into the vagina. (2) Swab is dipped in the vial with solvent. (3) AmniSure strip dipped into the solution. (4) Interpretation of the results.
Actim PROM
This test is similar AmniSure but employs the identification of placental protein-12 also known as insulin-like growth factor binding protein-1 (IGFBP-1) in the vaginal fluid. This test has a positive predictive value (PPV) and negative predictive value (NPV) of 83.8% and 88.6%, respectively, in the diagnosis of PROM.
Transabdominal intrauterine injection of dye
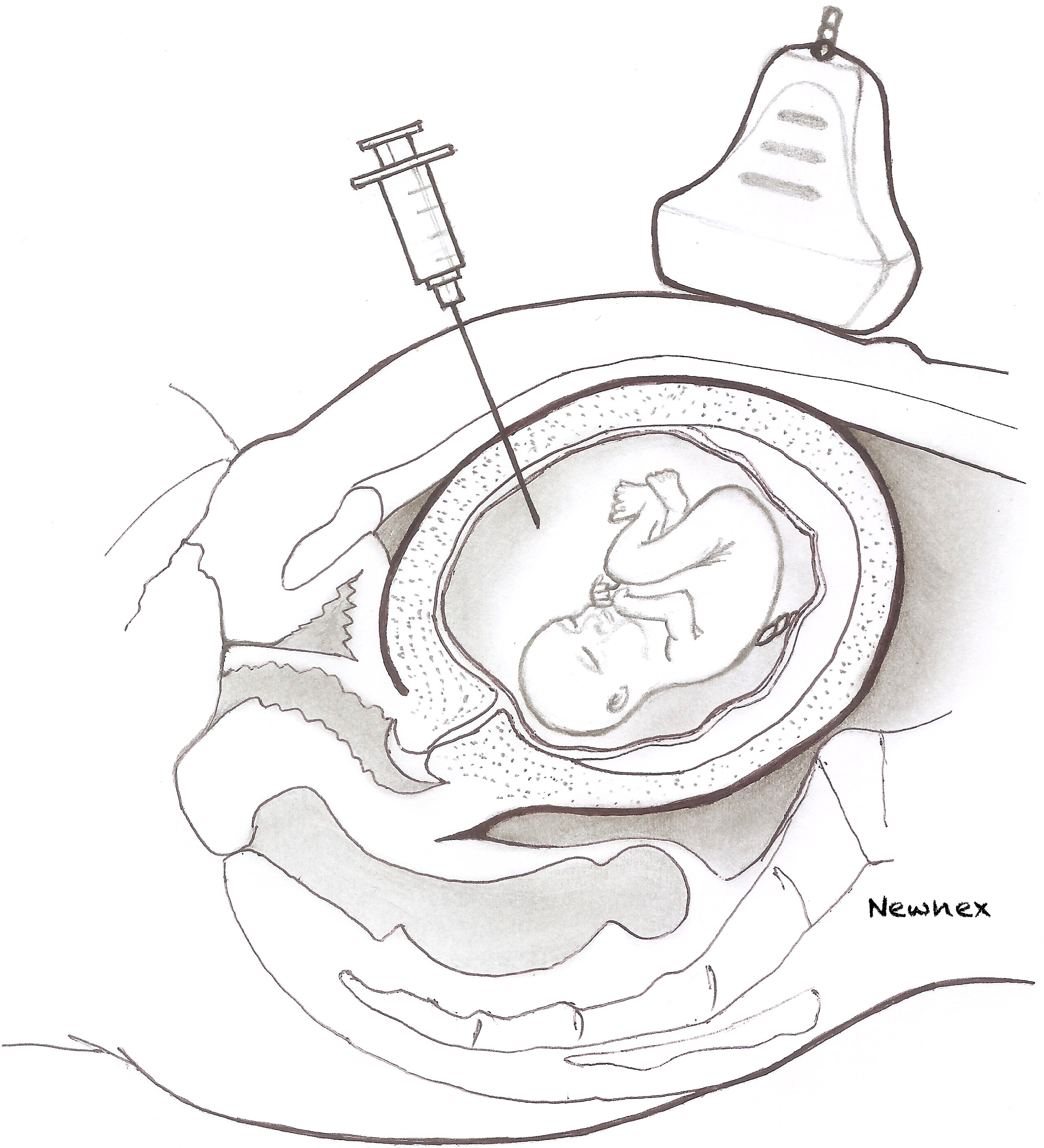
Amniocentesis is performed and indigo carmine dye instilled into the amniotic cavity, under ultrasound guidance. This procedure may be used to help in the diagnosis of rupture of membranes when the diagnosis remains difficult despite using the standard non-invasive methods (Figure 3).
3
Process of the transabdominal intrauterine injection of dye.
Fetal fibronectin
Fetal fibronectin is a protein produced in pregnancy that functions as a 'glue' attaching the chorion to the decidua. A negative fetal fibronectin result strongly supports absence of membrane rupture, but a positive result only indicates disruption of the interface between chorion and decidua, which can occur with intact membranes as in the case of preterm labor.21
Other tests
- An ultrasound examination to check for reduced amniotic fluid volume and for assessment of fetal well-being can also be undertaken to support the diagnosis or aid in management as well as to ascertain fetal dating if not already done previously;
- A full blood count to have a baseline white blood cell count is also performed since a new elevation of leukocyte count could be a sign of maternal infection. Other laboratory markers of infection include C-reactive protein (CRP) and procalcitonin;
- If the antenatal profile of the woman has not been previously undertaken, it would be prudent to perform;
- Amniosense is a pad commercially available in the UK, which looks like a panty liner, can detect the difference between urine and amniotic fluid by changing to a blue/green color when amniotic fluid is detected. This pad can be worn for up to 12 hours.
MANAGEMENT
A number of factors are considered where PPROM management is concerned. Some of the most important factors being gestational age and presence of infection. Other factors may include fetal status and well-being, fetal weight, maternal comorbidities, and presence of contractions or cervical dilation as well as availability of neonatal intensive care unit. Prematurity is the biggest concern in women with PPROM. Other complications include chorioamnionitis, oligohydramnions, necrotizing enterocolitis, cord compression, abruption placenta, respiratory distress syndrome, neurologic impairment and antepartum fetal death.10 In the absence of complications, management is centered on watchful waiting until 34 weeks, while in those beyond 34 weeks, delivery is considered after ascertainment of fetal lung maturity.
Management based on gestational age
In PPROM, there are several categories:
- 34–36 weeks
- 32–34 weeks
- 24–31 weeks
- Previable PROM at <24 weeks.
Gestational age: 34–36 weeks
This group, usually, has attained lung maturity. Studies show that there is no benefit in conservative management in this group.22 Prolonging the pregnancy may serve to increase the risk of infection in both the mother and the neonate. Antibiotics are therefore used for prophylaxis, including group B streptococcus prophylaxis as discussed later in this chapter. Upon membrane rupture, the patient possesses a risk of ascending infection.13 This should therefore be balanced against the risk of prematurity. It is essential to monitor both the mother and fetus closely to rule out all possibilities of ascending infection. This would include daily monitoring of vital signs such as temperature and pulse, and assessing for uterine tenderness and foul discharge. Other investigations may include a full blood count with differential blood count. PROM is not a contraindication to vaginal delivery and all other factors including fetal status and obstetric indications (obstetric hemorrhage or cord accidents) may be considered in determining the mode of delivery.
Gestational age 32–34 weeks
In this group, fetal lung maturity has to be confirmed before delivery is considered. Conservative management is considered where infection has been ruled out, both mother and fetus are stable and where lung maturity is yet to be established. There is no benefit in prolonging pregnancy where lung maturity is confirmed, and this only serves to increase the risk of infection. Where lung maturity is not confirmed, steroids are given, as well as antibiotic prophylaxis. Magnesium sulfate for neuroprotection is also considered. Close monitoring for infection to rule out evidence of chorioamnionitis is key.
Gestational age 24–31 weeks
Conservative management is strongly advised unless contraindicated, i.e. in presence of infection, hemorrhage and fetal compromise.10 Administration of corticosteroids to ensure fetal lung maturity, antibiotic prophylaxis and magnesium sulfate for neuroprotection are advised.23 Monitoring for contractions in anticipation of preterm birth, close monitoring for infection and fetal monitoring by ultrasound and cardiotocography are essential. Transfer to facilities with NICU services and the involvement of a neonatologist/pediatric team is important.
Previable PROM
Management in this scenario is highly individualized. Counselling of parents/families is important in ensuring that they are aware of the prognosis regardless of the interventions.
Even with prolongation of pregnancy and absence of infection, the fetus still has the risk of complications like Potter’s syndrome, chronic lung disease, neurologic abnormalities and cerebral palsy.10
MEDICAL MANAGEMENT IN PPROM
The three major aspects of medical management in PPROM include corticosteroid use, tocolysis, magnesium sulfate and antibiotics use.
Corticosteroid use for fetal lung maturity
Administration of corticosteroids has been made standard practice for lung maturation in preterm birth and evidence supports the continued use of a single course of antenatal corticosteroids to accelerate fetal lung maturation in women at risk.24 It has been shown that treatment with antenatal corticosteroids reduces the risk of perinatal death, neonatal death, intraventricular hemorrhage, respiratory distress syndrome, necrotizing enterocolitis, requirement for respiratory support and NICU admission, even with presence of advanced neonatal care.24
According to the World Health Organization, antenatal corticosteroid therapy is recommended for women at risk of preterm birth from 24 to 34 weeks of gestation provided that preterm birth is imminent, with accurate gestation dates and where maternal infection has been ruled out. This has to be in a setting where adequate care may be provided at childbirth and for the baby.25 According to this guideline, antenatal corticosteroid therapy is recommended in women with PPROM with no clinical signs of infection. Therefore its use is not recommended in women with features of chorioamnionitis.
Dexamethasone and betamethasone dosage
Betamethasone 12 mg given intramuscularly in two doses (once daily for 48 hours)
Dexamethasone 6 mg given intramuscularly in four doses (twice daily for 48 hours)26
A single repeat course of antenatal corticosteroid is recommended by WHO if preterm birth does not occur within a week after the initial dose, and a subsequent clinical assessment demonstrates that there is a high risk of preterm birth in the coming week.
Presence of diabetes mellitus should not be a contraindication to administration of steroids for lung maturation. Additional monitoring should be undertaken and glucose control maintained.25,26 Corticosteroid use at 34–36 weeks remains controversial but could be administered in cases of confirmed absence of fetal lung maturity.
PROPHYLACTIC ANTIBIOTIC THERAPY
In conservative management of PPROM, the use of antibiotics has been recommended as it prolongs latency (delays the onset of preterm labor) and improves neonatal outcomes as well as reduces the risk of maternal infection.10 In a review by Kenyon,27 the use of antibiotics following PPROM was associated with statistically significant reductions in chorioamnionitis and a reduction in the numbers of babies born within 48 hours and 7 days. The following markers of neonatal morbidity were reduced: neonatal infection, use of surfactant, oxygen therapy and abnormal cerebral ultrasound scan prior to discharge from hospital. The demonstrated delay in onset of labor may also allow sufficient time for effective prophylactic corticosteroids.
The choice and regimen of antibiotics are such that they cover for common pelvic pathogens.27 The NICE guideline in 2015, recommends offering women with PPROM oral erythromycin 250 mg 4 times a day for a maximum of 10 days or until the woman is in established labor, whichever is sooner.23 The National Institute of Child Health and Human Development (NICHD) Maternal-Fetal Medicine Units (MFMU) Network and ACOG 2018 recommend intravenous ampicillin 2 g every 6 hours and erythromycin 250 mg every 6 hours for 48 hours followed by oral amoxicillin 250 mg every 8 hours and erythromycin 333 mg every 8 hours for 5 days.28 Co-amoxiclav is associated with an increased risk of neonatal necrotizing enterocolitis and is therefore avoided.27,29 The ORACLE Children Study, evaluating children’s health at older ages, found that antibiotics seemed to have little effect on the health of children.30 Acceptable antibiotic dosages and duration are as illustrated in Table 2 below.
2
Acceptable antibiotic dosages and duration in PPROM.
Azithromycin 1 g orally upon admission, PLUS ampicillin 2 g intravenously every 6 hours for 48 hours, FOLLOWED BY amoxicillin 500 mg orally three times daily or 875 mg orally twice daily for an additional 5 days31 |
Ampicillin 2 g every 6 hours and erythromycin 250 mg every 6 hours for 48 hours followed by oral amoxicillin 250 mg every 8 hours and erythromycin 333 mg every 8 hours for 5 days29 |
A first generation cephalosporin such as cefazolin or cephalexin can be used for those with penicillin allergy in combination with a macrolide for those with low risk penicillin allergy. For those with high risk, clindamycin and a macrolide can be used for a total duration of 5 days31 |
Group B streptococcus prophylaxis
The use of intrapartum group B streptococcus (GBS) antibiotic prophylaxis in women with preterm PPROM who are test positive for GBS is recommended, even if the patient has previously received a course of antibiotics after PPROM.
TOCOLYSIS FOR INHIBITION OF PRETERM LABOR
Tocolytic use, although associated with longer overall latency with fewer births within 48 hours and 7 days, has no significant effect on perinatal mortality.32 The principal indication for tocolysis in the setting of PPROM is to delay delivery for 48 hours to allow administration of corticosteroids. Women most likely to benefit from use of a tocolytic drug are those who are in early preterm labor, requiring in utero transfer for NICU or for completion of steroid dose. As a rule, tocolytics should not be used for more than 48 hours. Tocolytics are contraindicated in patients who are in advanced labor (>4 cm dilation) or who have any findings suggestive of subclinical or overt chorioamnionitis.
WHO guideline recommends nifedipine as a preferred tocolytic agent for preterm labor for a brief interval to allow for steroid administration. Although betamimetics may be effective in tocolysis, it is not recommended due to higher risk of adverse effects.25 Regimens for tocolysis are as listed below.
Regimens for tocolysis
- Nifedipine an initial oral dose of 20 mg followed by 10–20 mg three to four times daily, adjust dose as per tocolytic effect for upto 48 hours
- Atosiban of an initial bolus dose of 6.75 mg over 1 minute, followed by an infusion of 18 mg/h for 3 hours, then 6 mg/h for up to 45 hours (to a maximum of 330 mg)
- Avoid use of multiple tocolytics due to adverse effects.
MAGNESIUM SULFATE FOR NEUROPROTECTION
Evidence supports the use of antenatal magnesium sulfate administration in women at risk of preterm birth as neuroprotection against cerebral palsy for the baby.33 The protective effects of magnesium sulfate on neurological complications are likely to be increased at earlier gestational ages.25
NICE recommends offering intravenous magnesium sulfate for neuroprotection of the baby to women between 24+0 and 29+6 weeks (and consideration for women at 30+0 and 33+6 weeks) of pregnancy who are in established preterm labor or having a planned preterm birth within 24 hours.23
Dosing regimens for magnesium sulfate neuroprotection
- Intravenous bolus of 4 g over 20 minutes, then 1 g/h until delivery or for 24 hours,23 whichever occurs first
- Intravenous bolus 4 g over 30 minutes as single dose
- Intravenous bolus 6 g over 20–30 minutes, followed by intravenous maintenance of 2 g/h.
*For women on magnesium sulfate, monitor for clinical signs of magnesium toxicity at least every 4 hours by recording pulse, blood pressure, respiratory rate and deep tendon (for example, patellar) reflexes and oliguria.
In summary, management of PPROM is largely influenced by gestational age (see Table 3). Conservative management is recommended until 34 weeks unless there are contraindications such as chorioamnionitis, fetal distress or active labor.
3
Summary of management of PPROM.
Gestational age | Management |
34 weeks or more | Proceed to delivery, by induction of labor or a by cesarean section if indicated Group B prophylaxis is recommended |
32–33 completed weeks | Expectant management unless fetal lung maturity is documented Group B streptococcus prophylaxis is recommended Corticosteroids should be administered Antibiotics to prolong latency |
21–31 completed weeks | Group B streptococcus prophylaxis is recommended Corticosteroids should be administered Antibiotics to prolong latency Magnesium sulfate should be administered incase delivery is imminent for neuroprotection |
Before 24 weeks | Patient counseling Induction of labor or expectant management Group B streptococcus prophylaxis is not recommended Corticosteroids are not recommended Antibiotics administration |
Complications
One of the most common complications of PPROM is early (premature) delivery. There exists an inverse relationship between the latent period, the time from membrane rupture until delivery, and the gestation at which PPROM occurs.34 A large study in Canada, United Kingdom and Australia demonstrated that slightly more than half of the women who had PPROM at 16–26 weeks' gestation had a latent period of 1 week with almost a quarter delivering after 4 weeks. In comparison, up to 95% of women with PROM near term had a latent interval of approximately 24 hours.35 There is a 3–4 fold risk in neonatal or perinatal mortality.36
Neonates who survive PPROM are often affected by numerous complications, both in utero and after delivery. The following are likely complications in utero malpresentation, oligohydramnios, intrauterine infection which occurs in 15–30% of women with preterm PROM and accounts for 3–20% of neonatal deaths, umbilical cord compression, umbilical cord prolapse and abruption placenta. Immediately after delivery a fetus is at risk of necrotizing enterocolitis, neurological impairment, intraventricular hemorrhage, respiratory distress syndrome which occurs in 10–40% of neonates, retinopathy of prematurity, patent ductus arteriosus, limb restriction deformities which complicate approximately 12% of preterm PROM, pulmonary hypoplasia which develops in 26% of preterm PROM prior to 22 weeks and fetal asphyxia.36,37,38,39,40,41 Infection, cord accident and other factors contribute to the 1–2% risk of intrauterine fetal demise (stillbirth) after preterm PROM.11,42
Potential maternal effects include, postpartum endometritis, chorioamnionitis and funisitis and septicemia in up to 33% of mothers, coagulopathy and delivery by cesarean section.36,43,44
PRACTICE RECOMMENDATIONS
- A woman presenting with a history of gush of fluid vaginally must have a sterile speculum examination to confirm the diagnosis of PROM. Digital cervical examinations should be avoided since they decrease the latent period and increase risk of infection without added clinical benefit.
- Antibiotics should be administered to patients with preterm PROM because they prolong the latent period and improve outcomes
- Corticosteroids should be given to patients with preterm PROM between 24 and 32 weeks’ gestation to decrease the risk of intraventricular hemorrhage, respiratory distress syndrome, and necrotizing enterocolitis.
- Long-term tocolysis is not indicated for patients with preterm PROM, although short-term tocolysis may be considered to facilitate maternal transport and the administration of corticosteroids and antibiotics.
- Multiple courses of corticosteroids and the use of corticosteroids after 34 weeks’ gestation are not recommended.
- When the diagnosis of chorioamnionitis is made, expeditious delivery should be done and intravenous antibiotics administered.
ACKNOWLEDGMENT
We are very grateful to Mongare Newnex Brian, a fifth year Medical student at the University of Nairobi, for the use of his artwork within this topic.
CONFLICTS OF INTEREST
Author(s) statement awaited.
Feedback
Publishers’ note: We are constantly trying to update and enhance chapters in this Series. So if you have any constructive comments about this chapter please provide them to us by selecting the "Your Feedback" link in the left-hand column.
REFERENCES
Simhan HN, Canavan TP. Preterm premature rupture of membranes: diagnosis, evaluation and management strategies. BJOG: An International Journal of Obstetrics and Gynaecology 2005;112(Suppl. 1):32–7. | |
F. Nili AA. Shams Ansari. Neonatal complications of premature rupture of membranes. Acta Medica Iranica 2003;41(3):175–9. | |
Parry S, Strauss JF, 3rd. Premature rupture of the fetal membranes. The New England Journal of Medicine 1998;338(10):663–70. | |
Oyen ML, Calvin SE, Landers DV. Premature rupture of the fetal membranes: is the amnion the major determinant? American Journal of Obstetrics and Gynecology 2006;195(2):510–5. | |
Kumar D, Moore RM, Mercer BM, et al. The physiology of fetal membrane weakening and rupture: Insights gained from the determination of physical properties revisited. Placenta 2016;42:59–73. | |
Moore RM, Mansour JM, Redline R, et al. The physiology of fetal membrane rupture: insight gained from the determination of physical properties, Placenta 2006;27(11–12):1037–51. | |
Guzick DS, Winn K. The association of chorioamnionitis with preterm delivery. Obstetrics and Gynecology 1985;65(1):11–6. | |
Moore RM, Schatz F, Kumar D, et al. Alpha-lipoic acid inhibits thrombin-induced fetal membrane weakening in vitro. Placenta 2010;31(10):886–92. | |
Joyce E, Diaz P, Tamarkin S, et al. In-vivo Stretch of Term Human Fetal Membranes. Placenta 2016;38:57–66. | |
Medina TM, Hill DA. Preterm premature rupture of membranes: diagnosis and management. Am Fam Physician 2006;73(4):659–64. | |
ACOG Practice Bulletin No. 80: premature rupture of membranes. Clinical management guidelines for obstetrician-gynecologists. Obstetrics and Gynecology 2007;109(4):1007–19. | |
Harger JH, Hsing AW, Tuomala RE, et al. Risk factors for preterm premature rupture of fetal membranes: a multicenter case-control study. American Journal of Obstetrics and Gynecology 1990;163(1 Pt 1):130–7. | |
Caughey AB, Robinson JN, Norwitz ER. Contemporary Diagnosis and Management of Preterm Premature Rupture of Membranes. Reviews in Obstetrics and Gynecology 2008;1(1):11–22. | |
Lee T, Carpenter MW, Heber WW, et al. Preterm premature rupture of membranes: risks of recurrent complications in the next pregnancy among a population-based sample of gravid women. American Journal of Obstetrics and Gynecology 2003;188(1):209–13. | |
Savitz DA, Blackmore CA, Thorp JM. Epidemiologic characteristics of preterm delivery: etiologic heterogeneity. American Journal of Obstetrics and Gynecology 1991;164(2):467–71. | |
Shen TT, DeFranco EA, Stamilio DM, et al. A population-based study of race-specific risk for placental abruption. BMC Pregnancy and Childbirth 2008;8:43. | |
Seeds AE, Hellegers A. Acid-base determinations in human amniotic fluid throughout pregnancy. American Journal of Obstetrics & Gynecology 1968;101(2):257–60. | |
Ferron M, Bilodeau R. Amniotic fluid crystallization test for ruptured membranes. Canadian Medical Association Journal 1963;89(21):1064. | |
Petrunin DD, Griaznova IM, Petrunina, Iu A, Tatarinov, Iu S [Immunochemical identification of organ specific human placental alphal-globulin and its concentration in amniotic fluid]. Akusherstvo i Ginekologiia 1977(1):62–4. | |
Abdelazim IA, Makhlouf HH. Placental alpha microglobulin-1 (AmniSure test) versus insulin-like growth factor binding protein-1 (Actim PROM test) for detection of premature rupture of fetal membranes. The Journal of Obstetrics and Gynaecology Research 2013;39(6):1129–36. | |
Eriksen NL, Parisi VM, Daoust S, et al. Fetal fibronectin: a method for detecting the presence of amniotic fluid. Obstetrics and Gynecology 1992;80(3 Pt 1):451–4. | |
Naef RW, Albert JR, Ross EL, et al. Premature rupture of membranes at 34 to 37 weeks' gestation: aggressive versus conservative management. American Journal of Obstetrics & Gynecology 1998;178(1):126–30. | |
National Institute for Health and Care Excellence (NICE) guideline, Preterm labour and birth, 2015. | |
Roberts D, Brown J, Medley N, et al. Antenatal corticosteroids for accelerating fetal lung maturation for women at risk of preterm birth. The Cochrane Database of Systematic Reviews 2017;3:Cd004454. | |
World Health Organisation, WHO recommendations on interventions to improve birth outcomes, 2015. | |
No RG-tG. 7: Antenatal Corticosteroids to Reduce Neonatal Morbidity and Mortality. London: RCOG, 2010. | |
Kenyon S, Boulvain M, Neilson JP. Antibiotics for preterm rupture of membranes. The Cochrane Database of Systematic Reviews 2013(12):Cd001058. | |
Mercer BM, Miodovnik M, Thurnau GR, et al. Antibiotic therapy for reduction of infant morbidity after preterm premature rupture of the membranes. A randomized controlled trial. National Institute of Child Health and Human Development Maternal-Fetal Medicine Units Network. JAMA 1997;278(12):989. | |
ACOG Practice Bulletin No. 199: Use of Prophylactic Antibiotics in Labor and Delivery. Committee on Practice Bulletins-Obstetrics. Obstet Gynecol 2018;132(3):e103. | |
Marlow N, Bower H, Jones D, et al. The ORACLE Children Study: educational outcomes at 11 years of age following antenatal prescription of erythromycin or co-amoxiclav. Archives of Disease in Childhood Fetal and Neonatal Edition 2017;102(2):F131–5. | |
Duff P, Lockwood CJ, Barss VA. Preterm prelabor rupture of membranes. UpToDate. Topic 6754 Version 112.0, 2018. | |
Mackeen AD, Seibel-Seamon J, Muhammad J, et al. Tocolytics for preterm premature rupture of membranes. The Cochrane Database of Systematic Reviews 2014(2):Cd007062. | |
Doyle LW, Crowther CA, Middleton P, et al. Magnesium sulphate for women at risk of preterm birth for neuroprotection of the fetus. The Cochrane Database of Systematic Reviews 2009(1):Cd004661. | |
Melamed N, Hadar E, Ben-Haroush A, et al. Factors affecting the duration of the latency period in preterm premature rupture of membranes. The journal of maternal-fetal & neonatal medicine: the official journal of the European Association of Perinatal Medicine, the Federation of Asia and Oceania Perinatal Societies, the International Society of Perinatal Obstet, 2009;22(11):1051–6. | |
Hannah ME, Ohlsson A, Farine D, et al. Induction of labor compared with expectant management for prelabor rupture of the membranes at term. TERMPROM Study Group. The New England Journal of Medicine 1996;334(16):1005–10. | |
ACOG practice bulletin. Premature rupture of membranes. Clinical management guidelines for obstetrician-gynecologists. Number 1, June 1998. American College of Obstetricians and Gynecologists. International Journal of Gynaecology and Obstetrics: the official organ of the International Federation of Gynaecology and Obstetrics, 1998;63(1):75–84. | |
Mercer BM. Preterm premature rupture of the membranes. Obstetrics and Gynecology 2003;101(1):178–93. | |
Smith CV, Greenspoon J, Phelan JP, et al. Clinical utility of the nonstress test in the conservative management of women with preterm spontaneous premature rupture of the membranes. The Journal of Reproductive Medicine 1987;32(1):1–4. | |
Cox SM, Leveno KJ. Intentional delivery versus expectant management with preterm ruptured membranes at 30–34 weeks' gestation. Obstetrics and Gynecology 1995;86(6):875–9. | |
Ananth CV, Savitz DA, Williams MA. Placental abruption and its association with hypertension and prolonged rupture of membranes: a methodologic review and meta-analysis. Obstetrics and Gynecology 1996;88(2):309–18. | |
Gonen R, Hannah M, Milligan J. Does prolonged preterm premature rupture of the membranes predispose to abruptio placentae? Obstetrics and Gynecology 1989;74(3 Pt 1):347–50. | |
Mercer BM, Arheart KL. Antimicrobial therapy in expectant management of preterm premature rupture of the membranes. Lancet (London, England) 1995;346(8985):1271–9. | |
Beydoun SN, Yasin SY. Premature rupture of the membranes before 28 weeks: conservative management. American Journal of Obstetrics and Gynecology 1986;155(3):471–9. | |
Garite TJ, Freeman RK. Chorioamnionitis in the preterm gestation. Obstetrics and Gynecology 1982;59(5):539–45. |
Online Study Assessment Option
All readers who are qualified doctors or allied medical professionals can automatically receive 2 Continuing Professional Development points plus a Study Completion Certificate from GLOWM for successfully answering four multiple-choice questions (randomly selected) based on the study of this chapter. Medical students can receive the Study Completion Certificate only.
(To find out more about the Continuing Professional Development awards programme CLICK HERE)