Androgen Biosynthetic Defects Producing Male Pseudohermaphroditism
Authors
INTRODUCTION
Impairment of androgen biosynthesis may result from genetic anomalies in which a deletion or functional abnormality of a critical testicular or adrenal enzyme has occurred. These enzymatic deficiencies may occur at any point in the biosynthesis of androgens. The resulting absence or functional impairment of discrete enzymes gives rise to deficient androgen production, a buildup of precursors, and characteristic clinical syndromes. Four specific androgen-deficiency syndromes resulting in inadequately virilized males (male pseudohermaphrodites) and variable effects in females are described in this chapter. 5-α-Reductase deficiency is reviewed elsewhere. Four related conditions, Leydig cell hypoplasia, instability of multiple P-450 enzymes, Smith-Lemli-Opitz syndrome, and deficiency of steroidogenic factor-1 (SF-1) are reviewed as well.
NORMAL ANDROGEN METABOLISM
Androgens
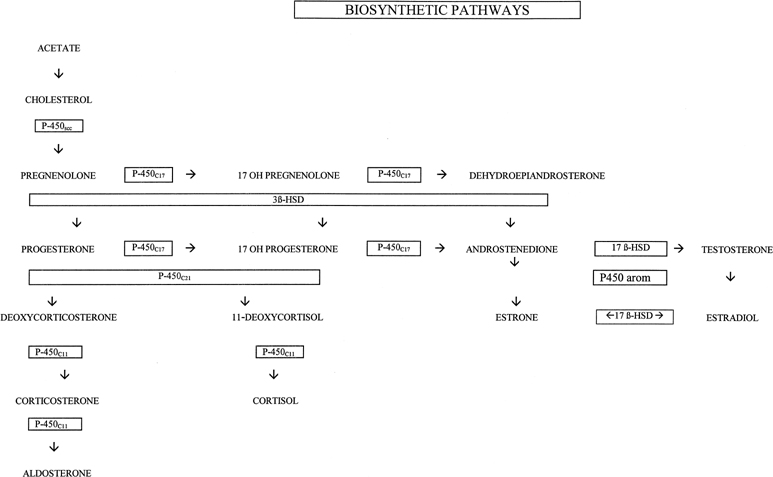
Androgens are chemically diverse compounds that by definition stimulate growth of tissues along the male reproductive tract.1 Most androgens are steroids; all have a unique binding affinity for the cytosolic androgen receptor. Androgen binding in the prostate produces several effects, including protein synthesis and growth of the prostate and seminal vesicles. Nitrogen retention is a well-known systemic effect of androgens. These sex steroids have critical roles in the formation of the male reproductive system in utero and in maintaining function in adult life. Androgens are synthesized from cholesterol in a sequence of enzymatically-controlled steps involving several intermediate products (Fig. 1). Each enzyme depends on the presence of a specific gene code for protein synthesis and formation of the respective gene.
{kind=link}
Testosterone is the most important androgen; it is biosynthesized in the Leydig cells in the testes and the stroma of the ovary. Testosterone is also produced in the adrenal cortex de novo and by conversion from metabolites in the liver, skin, and kidneys. Cholesterol for Leydig cell synthesis of testosterone may be secured from stored cellular cholesteryl ester or free cholesterol. Alternatively, it may be synthesized de novo from acetate through hydroxymethyl glutaryl coenzyme A (HMG CoA) reductase or derived from blood-borne cholesterol sources.2 A large pool of extracellular cholesterol, available to the testes, may be delivered as low-density lipoprotein (LDL). LDL serves as a ready source of cholesterol for testosterone biosynthesis in Leydig cells. Cholesterol for testosterone biosynthesis may be provided by this route following binding of the LDL protein (apoprotein B) to a high-affinity membrane receptor where it is internalized with the receptor by endocytotic vesicle formation. The vesicles then fuse with the lysosomes where proteolytic degradation of the LDL apoprotein moiety occurs, and free cholesterol is released into intracellular pools. The free cholesterol is then transported to mitochondria or sites of acylation to form cholesteryl ester stores, and the LDL receptor is then restored to the plasma membrane. Leydig cell mitochondria have the capacity to cleave the cholesterol sterol nucleus from the isocaproic acid side chain to produce pregnenolone. Pregnenolone is the precursor for all steroid synthesis in the testes and ovaries.
Testosterone production rate (total rate of entry) by various individual tissues is difficult to calculate but can be estimated by catheterization studies that permit determination of secretion rates, the amount of hormone secreted by the gland per unit of time (Table 1).3 Testosterone is bound to albumin and sex-steroid binding globulin (SSBG) or testosterone-estradiol binding globulin (TeBG) in plasma. TeBG is an 88,000 molecular weight polypeptide that is identical to the androgen-binding protein (ABP) produced in the testicular Sertoli cells but differs in oligosaccharide content. TeBG levels are increased by estrogen and thyroxine and decreased by androgens. Only 1–2% of testosterone in men is free or unbound, approximately 30% bound to TeBG, and 67% is bound to albumin but less avidly. The metabolic clearance rate of testosterone is correlated to the quantity of free and albumin-bound testosterone.4 It has been inferred that only the TeBG-bound fraction of testosterone is biologically unavailable. However, the biologic role of the TeBG bound fraction is not fully defined.
Table 1. Normal androgen metabolism
Metabolic Clearance Rate (1/24 hr/m2) | Plasma Concentration (ng/dL) | Production Rate (mg/24 hr) | Secretion Rate (mg/24 hr) | |||||
| Male | Female | Male | Female | Male | Female | Male | Female | |
Testosterone | 500 | 300 | 700 | 40 | 6–7 | 0.25–0.30 | 0.12 | |
Dihydrotestosterone | 400 | 200 | 30–55 | 20 | 0.30–0.39 | 0.06 | 0.25 | 0.02 |
Androstenedione | 1200 | 40–100 | 59–70 | 2.5 | 3.5 | 1.0 | 0.8–1.6 | |
Dehydroepiandrosterone | 1200–1600 | 400–480 | 8 | 0.3–3.0 | ||||
Testosterone may undergo several different metabolic fates. It may undergo aromatization to estradiol in adipose tissue, the pituitary gland, the brain, the breast, the liver, and the ovary. Alternatively, testosterone bioactivity may be amplified by conversion to dihydrotestosterone (DHT) in the cytoplasm by the enzyme 5-α-reductase. DHT, the most potent natural androgen, binds with greater affinity to the androgen receptor. DHT production occurs in the prostate gland, seminal vesicles, and skin. Conversely, testosterone exerts its effect in the muscle, kidney, and germinal epithelium without transformation to DHT.
DHT is bound to the cytoplasmic receptor where it is undergoes a temperature-dependent chromatin-mediated reaction. The messenger DNA generated by derepressed genes as a result of this union promotes specific protein synthesis in the cytoplasm. The enzyme 5-β-reductase may also act on testosterone and result in the formation of 5-β-DHT and other 5-β–reduced steroids, including etiocholanolone. These compounds have no significant effects on the reproductive tract but do stimulate red blood cell production in bone marrow. In the liver, androgens are conjugated with sulfates and glucuronides before biliary or renal excretion.
Androstenedione is also produced in Leydig cells, but it represents a small contribution to the overall androgen pool. It is a predominantly premenopausal androgen in women and is produced in roughly equal quantities in the gonads and the adrenals. It may be peripherally converted to testosterone by 17-β-hydroxysteroid oxidoreductase. It is an important precursor for estrogen biosynthesis in peripheral tissues in both sexes.
Dehydroepiandrosterone (DHEA) and its congener, dehydroepiandrosterone sulfate, are weak adrenal androgens that circulate in high concentrations but make minimal contributions to the overall androgenic milieu unless they are greatly elevated. Small amounts of DHEA may be converted to androstenedione and testosterone peripherally. DHEA sulfate is secreted by the adrenals in even larger amounts but is less efficiently converted to more active androgens.
Androgen Synthesis
Cholesterol is the primary substrate for androgen synthesis in both the adrenals and the gonads. The mitochondria of the adrenals, Leydig cells, ovarian stroma, and placenta are unique in possessing the ability to convert cholesterol to pregnenolone involving the mitochondrial cytochrome P-450scc 20,20-desmolase enzyme complex. These steps are regulated by adrenocorticotropic hormone (ACTH) in the adrenal and by luteinizing hormone (LH) in the ovary. An as yet unidentified trophic hormone from the anterior pituitary may also regulate adrenal androgen synthesis. After pregnenolone forms, it may be altered by 3-β-hydroxysteroid dehydrogenase isomerase to form progesterone and other compounds (steroids with their double bond shifted from the fifth and sixth carbons to the fourth and fifth position), or it may be processed without modifying the Δ5–3-β-ol to DHEA and androstenediol before finally being converted to testosterone. The Δ5 pathway predominates in estrogen synthesis, and the Δ4 pathway is used by the corpus luteum for progesterone and estradiol synthesis. Both pathways may be used in the synthesis of testosterone. The P-450scc complex, 3-β-hydroxysteroid dehydrogenase, and the 17-α-hydroxylase are present in both adrenal and sex steroids. Molecular cloning studies have demonstrated that the conversion of pregnenolone or progesterone to DHEA and androstenedione through 2-hydroxylation (17-α-hydroxylation) and cleavage (C17,20-lyase) steps is catalyzed by the same molecule, a single enzyme present in Leydig cell microsomes.5 Lyase (17,20-desmolase) and 17-β-hydroxysteroid oxidoreductase (17-β-hydroxysteroid dehydrogenase [17-β-HSD]) are present only in the gonads, and deficiencies of these enzymes singularly involve testosterone synthesis. The only reversible reactions in androgen biosynthesis are the reductions of androstenedione to testosterone and 19-hydroxyandrostenedione to 19-hydroxytestosterone. The equilibrium favors the synthesis of testosterone and estradiol, the most potent sex steroids, over the weaker 17 ketosteroids, androstenedione and estrone.
EMBRYOLOGIC ASPECTS OF SEXUAL DEVELOPMENT
Fetal gonads developed from anlagen present on the medioventral aspect of the urogenital ridge. Primordial germ cells migrate to this site to form the indifferent gonad. The gonads of male and female embryos are morphologically indistinguishable until approximately 6 weeks’ gestation, at which time organization of the testes occurs in males if the testes posses the critical elements of the Y chromosome. This process occurs about 43 days after conception and testicular tissue can be histologically recognized 7–8 weeks after conception or 9–10 gestational or menstrual weeks.
Appearance of the Sertoli cells and their organization of the surrounding cells into tubules is the first recognizable event in testicular differentiation. Sertoli cells and Leydig cells secrete hormones that are critical to subsequent male differentiation. Testosterone produced by the fetal Leydig cells is essential for the stabilization of the wolffian ducts and permits differentiation of vasa deferentia, epididymides, and seminal vesicles. Fetal Sertoli cells produce the glycoprotein anti-müllerian hormone (AMH), which diffuses locally and produces regression of the uterus and fallopian tubes.
SRY (sex-determining region Y chromosome) is the major testicular determinant and it is located on the short arm of the Y chromosome near the distal Xp/Yp pseudoautosomal region (PAR).6, 7 The SRY gene consists of two open-reading frames and the pivotal sequence involves an high mobility group (HMG) box encompassing codons 18–32. Testicular differentiation is regulated by interrelations between SRY and various autosomal and X loci. At this time it is not clear whether ovarian differentiation occurs as a default or constitutive event or is directed by a specific gene product. In any event, the indifferent gonad develops into an ovary in the absence of a Y chromosome. This transformation occurs 50–55 days after conception.
The external genitalia are initially identical in both sexes and at 8 weeks are bipotential. Testosterone biosynthesis begins about day 63 and the development of male external genitalia ensues at 65–67 days’ gestation. This process is dependent on testosterone production, which peaks during the 16th week, declines by 20 weeks, and remains low after 24 weeks’ gestation. Testosterone secretion is regulated by human chorionic gonadotropin (hCG) during early pregnancy and fetal LH and hCG after 15 weeks’ gestation. Follicle-stimulating hormone (FSH) is necessary for growth and development of ovarian follicles. Virilization of external genitalia is accomplished by DHT produced by conversion of testosterone by Δ5-α-reductase. DHT produces growth of the genital tubercle; fusion of the urethral fold such that the urethra is enveloped by the corpus spongiosum with resultant phallic urethra; fusion of the labioscrotal swellings to form the scrotum; differentiation of the prostate; and inhibition of vesicovaginal septal development. Analogous to genital differentiation, either absence of the testes (or Leydig cells) or impairment of testosterone and subsequent DHT production or action, results in lack of virilization of the external genitalia. Appropriate stimuli during the critical periods of fetal development are essential for normal sexual differentiation. Aberrations during embryogenesis or steroidogenesis may result in various anomalies in sexual development.
ABNORMAL ANDROGEN SYNTHESIS SYNDROMES
Deficiencies of steroidogenic enzymes include a group of genetic conditions involving adrenocorticoid and gonadosteroid biosynthesis. All are inherited in an autosomal recessive mode. Complete or partial enzyme deficiencies with resultant blocks in steroid synthesis result in the accumulation of immediate precursors and a shift in steroidogenesis toward less impeded pathways. Partial deficiencies tend to present with a broad array of symptomatology whereas complete enzyme deficiencies are more likely to be associated with dramatic clinical presentations.
Androgen production is similar in both the adrenals and the gonads and deficiencies may affect both targets. The testes lack 21- and 11-β-hydroxylase and have limited aromatase activity; the major testicular androgens are testosterone and androstenedione.
The first three enzymes involved with androgen production, cholesterol-desmolase complex, 3-β-hydroxysteroid dehydrogenase deficiency, and 17-α-hydroxylase are involved with the production of both cortisol and testosterone and their deficiencies are typically associated with varying degrees of adrenal insufficiency and sexual ambiguity. 17-α-hydroxylase and 17,20 lyase are utilized only in the production of androgens and not for cortisol synthesis (Table 2). Individuals with these deficiencies present with sexual ambiguity only. An enzyme deficiency associated with abnormal androgen synthesis syndromes should be suspected in 46,XY individuals with sexual ambiguity and deficient levels of testosterone and its metabolites.
Table 2. Abnormal androgen synthesis syndromes
ACTH | Cholesterol Desmolase Complex Deficiency (Adrenal Lipoid Hyperplasia) ↑ | 3β-Hydroxysteroid Dehydrogenase Deficiency ↑ | 17 α-Hydroxylase Deficiency ↑ | 17,20-Desmolase Deficiency N | 17 β-Hydroxysteroid Dehydrogenase Deficiency N |
Progesterone | ↓ | ↓ | ↑ | ||
Testosterone | A | A | ↓ | ↓ | ↓ |
Androstenedione | ↓ | ↓ | ↓ | ↓ | (↑N) |
DHEA | ↓ | ↑ | ↓ | ↓ | N |
17-OH-progesterone | ↓ | ↓ | ↓ | ↑ | |
Aldosterone | ↓ | ↓ | ↓ | N | N |
Cortisol | ↓ | ↓ | ↓ | N | N |
17-ketosteroinds | A | ↑ | ↓ | ↓ | N |
17-OH-corticosteroinds | A | ↓ | ↓ | N | N |
Pregnanediol | A | ↓ | ↑ | ↑ |
|
Pregnanetriol | A | ↓ | ↓ | ↑ |
|
A, absent; N, normal; ↑ increased; ↓ decreased.
ACTH, adrenocorticotropic hormone; DHEA, dehydroepiandrosterone.
Recent advances in molecular genetics have greatly expanded our understanding of these disorders. Deficiencies of steroidogenetic enzymes may result from three types of genetic aberrations: point mutations, gene deletions or insertions, and gene conversions. Point mutations (single-base changes) are the most common type of gene conversion.
Congenital Adrenal Lipoid Hyperplasia
In 1955 Prader and Gurtner8 described a group of infants with severe adrenal insufficiency and massive amounts of cholesterol deposited in the adrenal cortex and gonads. Patients with a deficiency of cholesterol side-chain cleavage enzyme (P-450scc) lack the ability to metabolize cholesterol in the adrenals and develop large, yellow, foamy adrenal glands. The enzyme P-450sec initiates the steroidogenic pathway cleaving a 6-carbon side chain from cholesterol to produce pregnenolone. This rate-limiting step is regulated by ACTH, angiotensin II in the adrenal glands, and by gonadotropins in the gonads. Abnormalities of this enzyme are extremely rare and usually incompatible with life.
CYP11A is the gene that encodes for cytochrome P-450scc It has been cloned and localized to the long arm of chromosome 15, it is 20 kb long, and consists of 9 exons.9 In rabbits, homozygous CYP11A1 deletion adrenal lipoid hyperplasia consistently occurs. However, abnormalities in the CYP11A gene have never been observed in humans with congenital adrenal lipoid hyperplasia.10 The disorder in humans appears to be the result of perturbations of the gene encoding, steroidogenic acute regulatory protein (StAR). The StAR protein is responsible for delivery of precursors for cholesterol side chain cleavage. The term acute in the name refers to the rapid response to corticotropin stimulation to produce a 30-kd mitochondrial protein in adrenal cells. The StAR gene is 8-kb long and consists of 7 exons and has been mapped to 8P11.2.11
A variety of mutations has been reported.12 Approximately 100 cases have been reported and reflect preponderance among Japanese and Koreans. At least 15 different mutations have been reported. Eighty percent of affected Koreans and Japanese have the same mutant allele, Gln 258 (stop). Arg 182 Leu affects 78% of Arabs reported to have congenital adrenal lipoid hyperplasia.10
Adrenal insufficiency with low levels of cortisol, aldosterone, and androgens is the principal manifestation. Hyperpigmentation and respiratory distress occur in 25% of affected neonates. They present with failure to thrive, lethargy, vomiting, diarrhea, hypernatremia, hypokalemia, and hypertension. ACTH levels and plasma renin activity are elevated. Genetic males present with ambiguous or female external genitalia. Affected females have normal genitalia. All surviving infants have been assigned female gender identities. Successful treatment can be accomplished with glucocorticoids and mineralocorticoid replacement. Prophylactic orchiectomy should be performed on affected males, and all patients may benefit from estrogen therapy to initiate pubertal development at the appropriate time.
3-β-Hydroxysteroid Dehydrogenase Deficiency
Bongiovanni13 initially described this syndrome in 1962 as a variant of the adrenogenital syndrome (coincident adrenal disease and abnormal genital development). The syndrome results from a block in the conversion from the Δ5 to Δ4 pathways (see 3-β-HSD in Fig. 1). Previously, two enzymes, 3-β-hydroxysteroid dehydrogenase and Δ5,Δ4 isomerase were thought to be required for this reaction, but a single 45-kb protein has been identified with both dehydrogenase and isomerase activities which are inseparable.14 Moreover, 3-β-hydroxysteroid dehydrogenase is the only steroidogenic enzyme leading to the production of cortisol that does not depend on cytochrome P-450; it requires the cofactor nicotinamide-adenine dionucleotide oxidized (NAD+) and is a microsomal enzyme.
Human 3-β-hydroxysteroid dehydrogenase (both types I and II) has two isoenzymes and corresponding messenger RNA. These genes have been localized to the long arm of chromosome 1 in the P11–13 band15, 16 and both have four exons. Type II is expressed in gonads and adrenals. Mutations that produce both virilization and salt wasting have essentially abolished enzyme activity; mutations associated only with virilization are missense mutations with 1–10% of normal enzyme activity.17 The mutations producing the two phenotypes are scattered among all of the exons.
Two forms of 3-β-hydroxysteroid dehydrogenase deficiencies have been described. The classic, as originally described by Bongiovanni, is associated with complete block of 3-β-hydroxysteroid dehydrogenase activity, and the nonclassic with a partial deficiency. Patients with classic, 3-β-hydroxysteroid dehydrogenase deficiency present in infancy with severe sodium wasting and the outcome is fatal if early intervention is not undertaken. The adrenals and gonads are affected with resulting deficient production of glucocorticoids, mineralocorticoids, and sex steroids. Cortisol deficiency results in ACTH stimulation and congenital adrenal hyperplasia. Production of both androgens and estrogens is impaired and the major androgen produced is DHEA, which is responsible for incomplete virilization in males and partial virilization in females. Thus, 3-β-hydroxysteroid dehydrogenase is the only enzyme deficiency associated with both male and female pseudohermaphroditism. Diagnosis is established with elevated pregnenolone, DHEA, and ratios of Δ5/Δ4 steroids. In males, testes are usually palpable, with various degrees of hypospadias or incomplete pseudovagina hypospadias. Females may have clitoral enlargement and partial or complete labial fusion.
The nonclassic form of 3-β-hydroxysteroid dehydrogenase deficiency is associated with a partial deficiency and represents a less severe clinical presentation and is much more common than the classic presentation. The typical presentation of the nonclassic form is either premature pubarche or pubertal hyperandrogenism.18 Clinical presentation in females may be similar to polycystic ovarian syndrome with hirsutism, acne, menstrual irregularities, and infertility. Four biochemical criteria have been proposed for the diagnosis of nonclassic or late onset 3-β-hydroxysteroid dehydrogenase.19 After a 60-minute ACTH stimulation, patients should have an elevation greater than two standard deviations above the mean in 17-pregnenelone, DHEA, 17-pregnenelone:17-hydroxyprogesterone ratio, and 17-pregnenelone:cortisol ratio. Adrenal suppression with glucocorticoids is effective treatment when the diagnosis is established.
P-450c17:17-α-hydroxylase/17,20 lyase
Desmolase Deficiencies
This syndrome was initially reported by Biglieri and associates20 in 1966 in four 46,XX females and has subsequently been described in males presenting with ambiguous genitalia.21, 22 Steroid 17-α-hydroxylase/17,20-lyase (P-450c17) is a single-cytochrome-450 enzyme that catalyzes 17-α-hydroxylase and 17,20-lyase reactions in conjunction with NADPH-cytochrome P-450 reductase. It is expressed in the adrenal and gonads and is required for formation of sex hormones and glucocorticoids. Current evidence has definitively established the existence of a single P-450 C17 enzyme with two actions.23, 24 Defects in P-450c17 may be responsible for 17-hydroxylase, 17,20 lyase deficiencies or both. A single enzyme producing both 17-α-hydroxylase and 17,20 desmolase activity has created considerable nosologic and genetic confusion.25 Mutations have been observed with only altered 17,20 lyase function.26 Specific regions have been identified in the rat responsible for unique enzymatic activities.27
The human P-450c17 gene (CYP17) is a single copy gene localized to chromosome 10q24-25 with 8 exons.28, 29, 30 It contains 508 amino acids and has a molecular weight of approximately 57 kd. The gene has been completely analyzed and sequenced. Mutations have been found in the structural gene and regulatory sequences determining expression of gene CYP17. A number of missense mutations have been described usually ablating P-450c17 function.
P-450c17 is expressed in the adrenal gland and the gonads; deficiencies lead to inadequate cortisol and sex steroid production. ACTH is increased by the cortisol deficiency and the block at 17-α-hydroxylase promotes excessive production of 17-deoxysteroids, especially deoxycorticosterone (DOC), which has potent mineralocorticoid activity. Elevated mineralo-corticoid levels produce hypernatremia with low renin hypertension, hypokalemia, and metabolic alkalosis. Deficient sex steroids result in elevated gonadotropin levels.
Clinical presentation in males includes sexual ambiguity, which correlates with the severity of the block in P-450c17 activity and the resulting impairment in testosterone production. Testes may be intra-abdominal within the inguinal canal or within the labioscrotal folds. Inguinal hernias are a common accompaniment. Males typically have hypoplastic wolffian structures and females have normal but infantile müllerian structures. Most patients present at puberty with primary amenorrhea or delayed pubertal development.31 A few patients have been diagnosed in infancy, presenting with ambiguous genitalia and hypertension. Affected females are more likely to be hypertensive while 17-α-hydroxylase deficient males are more often normotensive.
Relevant laboratory findings include high serum levels of 17-deoxysteroids, progesterone, DOC, and corticosterone. Serum levels of 17-hydroxysteroids, including cortisol and DHEA, testosterone, and estrogens are undetectable. P-450c17 deficiency is treated with glucocorticoid suppression similar to therapy in patients with congenital adrenal hyperplasia. Hormone replacement therapy may be given at puberty to initiate secondary sexual development. Individuals with ambiguous genitalia undergo sex assignment at birth and may be raised as males if phallic development is adequate or may undergo phallic reduction and gonadectomy if not.
17-β-Hydroxysteroid Dehydrogenase Deficiency (17-Ketosteroid Reductase)
A defect in the last step of testosterone synthesis, the conversion on androstenedione to testosterone (see 17-β-HSD in Fig. 1), was first described by Neher and Khant in 1965.32 Several additional males, including siblings, have been described subsequently, having less compromise of virilization than those with other causes of impaired androgen synthesis.33, 34, 35, 36, 37, 38, 39 Some affected individuals are born and reared as females but undergo marked virilization at puberty, similar to men with 5-α-reductase deficiency. The disorder is rare but relatively common in certain populations such as among Arabs living in the Gaza strip.40
17-β-HSD is an NADPH-dependent microsomal enzyme that catalyzes the reversible reduction necessary to form testosterone from estrone. Five isozymes have been cloned that catalyze the oxydoreduction of androstenedione, testosterone, and DHT, estrone, and estradiol.41
The 17-β-HSD gene has been localized to chromosome 9. At least 14 mutations in the 17-β-HSD enzyme gene have been identified from different ethnic groups. Type 3 17-β-HSD isozyme consists of 11 exons and has its primary action in the gonads. Deficiency of this enzyme is associated with the form of male pseudohermaphroditism most frequently seen in Gaza. The most common mutation is a missense mutation in exon 3 that reduces enzyme activity to 15–20% of normal.42 Other mutations reported in additional populations involve all 11 exons and include frame shifts, splice junction alterations in addition to the most common missense mutations.
Males affected with the 17-β-HSD gene have normal wolffian structures but ambiguous genitalia. Phenotypic variability has been reported within families with the same homozygous mutation.43 Many have been raised as females but virilized at puberty and subsequently adopted a male gender role. Some develop gynecomastia. These individuals have elevated serum levels of androstenedione resulting from an inability to make testosterone, increased DHEA because of an inability to make Δ5 androstenediol, and high estrone levels resulting from an inability to convert to estradiol. At puberty, testosterone and estradiol levels are markedly decreased over normal values. Diagnosis is established by endocrine evaluation and mutation analysis.43
Treatment involves gonadectomy and estrogen supplementation at puberty for those raised as females. One individual with teratocarcinoma and metastasis has been reported.44 Individuals raised as males benefit from repair of the hypospadias and may require testosterone replacement. These individuals do not achieve spermatogenesis, and histologic examination in the postpubertal male reveals Leydig cell hypoplasia.
Leydig Cell Hypoplasia
Patients with Leydig cell hypoplasia present with a decreased response of the Leydig cells to luteinizing hormone. Patients with this syndrome may present with variable findings ranging from frankly ambiguous genitalia to normal male genitalia with micropenis. A recent study of three affected brothers with a mild form of Leydig cell hypoplasia revealed a homozygous missense mutation resulting in a substitution of a lysine residue for an isoleucine residue at position 625 of the receptor.45 Studies showed a correlation between the severity of clinical presentation and overall receptor signal capacity, a combination of cell-surface expression and coupling efficiency.
Instability of Multiple P-450 Enzymes
A 6-month old, 46,XY infant was described with genital ambiguity and multiple enzyme defects, including 17-α-dehydroxylase, 21-hydroxylase, and 17,20-desmolase in 1985. Peterson and associates46 suggested a new form of male pseudohermaphroditism, postulating that multiple adrenal biosynthetic abnormalities arose as a consequence of an abnormality of the cytochrome P-450 system. Enzymes involved in adrenal biosynthesis include both mitochondrial and cytoplasmic P-450 enzymes.47
Smith-Lemli-Opitz Syndrome
Smith-Lemli-Opitz Syndrome (SLO) is a relatively common (1:10,000) autosomal recessive syndrome affecting 46,XY individuals with variable expression ranging from hypospadias to male pseudohermaphrodism.48 Of the two types described, hypospadias is the most common abnormality identified with type I SLO. Type II SLO has been associated with ambiguous external genitalia and even frank sex reversal.49 A mutation of the gene whose enzyme converts 17-hydroxycholesteral to cholesterol has been implicated in type I and type II.50, 51 The most common associated molecular abnormality is an exon-intronic splicing defect. Maternal serum estriol levels are low to nondetectable in pregnancy. Dehydropregnanetriol and dehydro-estriol are detectable in maternal serum and urine during affected pregnancies. These compounds are not detectable in normal pregnancies, making antenatal testing for SLO feasible, and treatment with a high cholesterol diet has been considered.52
Deficiency of Steroidogenic Factor-1
Steroidogenic factor-1 (SF-1) is an orphan nuclear receptor encoded by the FTZ1 gene located on 9q33 and translated into a zinc finger protein. It is considered to be an orphan receptor because no ligand has yet been identified. Prior to identification of human cases, disruption of FTZ1 in mice (knockout) was observed to disrupt adrenal and gonadal development as well as hypothalamic and pituitary gonadotrophic tissue.53, 54 On the basis of the mice studies, it was predicted that mutations in human FTZ1 would produce abnormal SF-1 receptors and lead to significant abnormalities of sexual development.
Achermann55 described the first human case of SF-1 deficiency caused by mutant FTZ-1. The affected 46,XY individual demonstrated primary adrenal failure, female genitalia, streak gonads, and normal müllerian-derivative responsive hormones. After appropriate studies were completed to exclude congenital adrenal lipoid hypoplasia, the proband was demonstrated to be heterozygous for a 2bp substitution in FTZ-1 at codon 35. SF-1 is believed to regulate repression of AMH. The presence of normal müllerian structures in the reported patient despite genital and gonadal abnormalities supports such a role for SF-1.
GENERAL MANAGEMENT
Although medical care for these patients is straightforward, the profound anxiety that these patients and their families experience necessitates that they be treated with great sensitivity. Ideally, sex assignment should be made in the delivery room, but this is not always possible. In these situations, it may be preferable to tell the parents that the infant’s genitalia are 'not completely formed' and gender identity assignment may have to await testing. Early assessment of electrolyte status is also a critical feature of the preliminary evaluation.
Most individuals with abnormalities of testosterone synthesis will be successfully raised as females. Among 46,XY infants with anomalies more severe than fourth degree hypospadias (urethra at the base of phallus), they are unlikely to have adequate male sexual function and should be raised as females. Orchiectomy should be performed in all 46,XY individuals raised as females to prevent malignant transformation of intra-abdominal testes and potential virilization at puberty with incomplete blocks. A few 46,XY individuals with more subtle genital ambiguity can be reared as males with appropriate reconstructive surgery; sexual maturation can be induced with androgens at puberty. It is unlikely that any such individuals will be fertile.
Diagnosis must be confirmed by appropriate endocrine and cytogenetic studies before instituting therapy and other forms of male pseudohermaphroditism must be excluded from the differential diagnosis. In particular, individuals with 5-α-reductase deficiency should be identified and spared sex reassignment because they may expect to function as fertile males after puberty.
Ultimately, the evaluation of individuals with abnormal androgen synthesis and metabolism and ambiguous genitalia is clinical. Although DNA testing of other family members may be helpful in assessing risk to their children, DNA testing has not been proven to be clinically useful in establishing the diagnosis. Associated gene abnormalities have been too heterogeneous with too many point mutations to permit definitive diagnosis by DNA testing alone.
REFERENCES
Kochakian CD: Definition of androgens and protein of anabolic steroids. Pharmacol Ther B 1:149, 1975 |
|
Brown MS, Kovanen PT, Goldstein JL: Receptor mediated uptake of lipoprotein-cholesterol and its utilization for steroid synthesis in the adrenal cortex. Recent Prog Horm Res 35:215, 1979 |
|
Kirschner MA, Jacobs JB: Combined ovarian and adrenal vein catheterization to determine the site(s) of androgen over-production in hirsute women. J Clin Endocrinol Metab 33:199, 1971 |
|
Vermulen A, Stoica T, Verdonek L: The apparent free testosterone concentration, an index of androgenicity. J Clin Endocrinol Metab 29:1470, 1969 |
|
Miller WL: Molecular biology of steroid hormone synthesis. Endocr Rev 9:295, 1988 |
|
Gubbay J, Collignon J, Koopman P, et al: A gene mapping to the sex-determining region of the mouse Y chromosome is a member of a novel family of embryonically expressed genes. Nature 346:245, 1990 |
|
Sinclair AH, Berta P, Palmer MS, et al: A gene from the human sex-determining region encodes a protein with homology to a conserved DNA-binding motif. Nature 345:240, 1990 |
|
Prader A, Gurtner HP: Das Syndrom des Pseudo-hermaphroditismus masculinus bei kongenitaler nebennierenrinden Hyperplase ohne androgen Uberproduktion. Helv Pediatr Acta 12:509, 1955 |
|
Chung BC, Matteson KJ, Voutilainen R, et al: Human cholesterol side-chain cleavage enzyme, P-450scc: cDNA cloning, assignments of the gene to chromosome 15 and expression in the placenta. Proc Natl Acad Sci USA 82:8962, 1986 |
|
Lin D, Gitelman SE, Saenger P, et al: Normal genes for the cholesterol side chain cleavage enzyme, P-450scc, in congenital lipoid adrenal hyperplasia. J Clin Invest 88:1955, 1991 |
|
Bose HS, Sugawara T, Strauss JF III, et al: The pathophysiology and genetics of congenital lipoid adrenal hyperplasia. International Congenital Lipoid Adrenal Hyperplasia Consortium. N Engl J Med 335:1870, 1996 |
|
Rose HS, Sugawara T, Strauss JF, et al: The pathophysiology and genetics of congenital lipoid adrenal hyperplasia. International congenital lipoid adrenal hyperplasia consortium N Engl J Med 335:1870, 1996 |
|
Bongiovanni AM: Androgenital syndrome with deficiency of 3-beta hydroxysteroid dehydrogenase. J Clin Invest 41:2086, 1962 |
|
Lorence MC, Murray BA, Trant JM, et al: Human 3 beta-hydroxysteroid dehydrogenase/D5® 4 isomerase from placenta; expression in non-steroidogenic cells of a protein that catalyzes the dehydrogenation/isomerization of C21 and C19 steroids. Endocrinology 126:2493, 1990 |
|
Lorence MC, Corbin CJ, Kamimura N, et al: Structural analysis of the gene encoding human 3 beta-hydroxysteroid dehydrogenase/D5® 4 isomerase. Molec Endocrinol 4:1850, 1990 |
|
Berube D, Luu-The V, Lachance Y, et al: Assignment of the human 3 beta-hydroxysteroid dehydrogenase gene (HSD beta 3) to the p 13 band of chromosome 1. Cytogenet Cell Genet 52:199, 1989 |
|
Simard J, Sanchez R, Durocher F, et al: Structure-function relationships and molecular genetics of the 3 beta-hydroxysteroid dehydrogenase gene family. J Steroid Biochem Mol Biol 55:489, 1995 |
|
Temeck JW, Pang S, Nelson C, et al: Genetic defects of steroidogenesis in premature pubarche. J Clin Endocrinol Metab 64:609, 1987 |
|
Pang S, Lerner AJ, Stoner E, et al: Late-onset adrenal steroid 3 beta-hydroxysteroid dehydrogenase deficiency. I. A cause of hirsutism in pubertal and postpubertal women J Clin Endocrinol Metab 60:428, 1985 |
|
Biglieri EG, Herron MA, Brust N: 17-hydroxylation deficiency in man. J Clin Invest 45:1946, 1966 |
|
Heremans GFP, Moolenaar AJ, vanGelderen HH: Female phenotype in a male child due to a 17 alpha-hydroxylase deficiency. Acta Dis Child 51:721, 1976 |
|
New MI: Male pseudohermaphroditism due to a 17 alpha-hydroxylase deficiency. J Clin Invest 49:1930, 1970 |
|
Bradshaw KD, Waterman MR, Couch RT, et al: Characterization of complimentary deoxyribonucleic acid for human adrenocortical 17 alpha-hydroxylase: A prove for analysis of 17 alpha-hydroxylase deficiency. Mol Endocrinol 1:348, 1987 |
|
Zuber MX, Simpson ER, Waterman MR: Expression of bovine 17 alpha-hydroxylase cytochrome P-450 cDNA in nonsteroidogenic (cos1) cells. Science 234:1258, 1986 |
|
Nebert DW, Nelson DR, Adesnik M, et al: The P-450 superfamily: Updated listing of all genes and recommended nomenclature for the chromosomal loci. DNA 8:1, 1989 |
|
Geller DH, Auchus RJ, Mendonea BB, et al: The genetic and functional basis of isolated 17,20-lyase deficiency. Nat Genet 17:201, 1997 |
|
Kitamura M, Buczko E, Dufau ML: Dissociation of hydroxylase and lyase activities by site-directed mutagenesis of the rat P-450 17 alpha. Mol Endocrinol 5:1373, 1991 |
|
Kagimoto M, Winter JSD, Kagimoto K, et al: Structural characterization of normal mutant human steroid 17 alpha-hydroxylase genes: Molecular basis of one example of combined 17 alpha-hydroxylase/17,20-lyase deficiency. Mol Endocrinol 2:564, 1988 |
|
Pigato-Leonard J, Miller WL: Cloning and sequence of the human gene for P-450c21. DNA (steroid 17 alpha-hydroxylase/17,20-lyse): Similarity with the gene for P-450c21 DNA 6:439, 1987 |
|
Matteson KJ, Picado-Leonard J, Chung C-C, et al: Assignment of the gene for adrenal P-450c17 (steroid 17 alpha-hydroxylase/17,20-lyse) to human chromosome 10. J Clin Endocrinol Metab 63:789, 1986 |
|
Chantilis SJ, Bradshaw KD: Clinical and molecular aspects of steroidogenic enzyme deficiencies. Reprod Genet 5:81, 1994 |
|
Neher R, Khant FW: Gonadal steroid biosynthesis in vitro in four cases of testicular feminization: Androgens in normal and pathologic conditions. p 130, International Congress Series No. 101. Amsterdam, Excerpta Medica, 1965 |
|
Saez JM, Morera AM, de Peretti E, et al: Familial male pseudohermaphroditism with gynecomastia due to testicular 17-ketosteroid reductase defect (compared to a case of terminal feminization). J Clin Endocrinol Metab 34:598, 1972 |
|
Givens JR, Wiser WL, Summit RT, et al: Familial male pseudohermaphroditism without gynecomastia due to deficient testicular 17-ketosteroid reductase activity. N Engl J Med 291:938, 1974 |
|
Goebelsmann U, Horton R, Mestman JM, et al: Male pseudohermaphroditism due to testicular 17 beta-hydroxysteroid dehydrogenase deficiency. J Clin Endocrinol Metab 36:867, 1973 |
|
Pittaway DE, Andersen RN, Givens JR: Deficient 17-hydroxysteroid oxidoreductase activity in testes from a male pseudohermaphrodite. J Clin Endocrinol Metab 43:457, 1976 |
|
Knorr D, Bidlingmaier F, Engelhardt D: Reifenstein syndrome, a 17-beta-hydroxysteroid-oxyoreductase deficiency. Acta Endocrinol 173:37, 1973 |
|
Imperato-McGinley J, Peterson RE, Stoller R, et al: Male pseudohermaphroditism secondary to 17 beta-hydroxysteroid dehydrogenase deficiency: Gender role change with puberty. J Clin Endocrinol Metab 49:391, 1979 |
|
Mendonca B, Inacio M, Arnhold IVP, et al: Male pseudohermaphroditism due to 17β-hydroxysteroid dehydrogenase 3 deficiency. Medicine 79:299, 2000 |
|
Rosler A, Belanger A, Labria P: Mechanisms of androgen production in male pseudohermaphroditism due to 17 beta-hydroxysteroid dehydrogenase deficiency. J Clin Endocrinol Metabol 75:733, 1992 |
|
Zhu YS, Katz MD, Imperato-McGinley J: Natural potent androgens: Lesions from human genetic models. Baillieres Clin Endocrinol Metab 12:83, 1998 |
|
Andersson S, Geissler WM, Wu L, et al: Molecular genetics and pathophysiology of β-hydroxysteroid dehydrogenase 3 deficiency. J Clin Endocrin Metab 81:130, 1996 |
|
Boehmer ALM, Brinkmann AO, Sandkuljl LA, et al: 17β-hydroxysteroid dehydrogenase 3 deficiency: Diagnosis, phenotypic variability, population genetics, and worldwide distribution of ancient and de novo mutations. J Clin Endocr Metab 84:4713, 1999 |
|
Balducci R, Toscano V, Write F, et al: Familial male pseudohermaphroditism with gynecomastia due to 17 beta-hydroxysteroid dehydrogenase deficiency. A report of three cases Clin Endocrinol 23:439, 1985 |
|
Martens JW, Verhoef-Post M, Abelin N, et al: A homozygous mutation in the luteinizing hormone receptor causes partial Leydig cell hypoplasia: Correlation between receptor activity and phenotype. Mol Endocrinol 12:775, 1998 |
|
Peterson RE, Imperato-McGinley J, Gautier T, et al: Male pseudohermaphroditism due to multiple defects in steroid-biosynthetic microsomal mixed function oxidase.A new variant of congenital of adrenal hyperplasia N Engl J Med 313:1182, 1985 |
|
Miller WL, Levine LS: Molecular and clinical advances in congenital adrenal hyperplasia. J Pediatr 11:1, 1987 |
|
Ryan AK, Bartlett K, Clayton P, et al: Smith-Lemli-Opitz syndrome: A variable clinical and biochemical phenotype. J Med Genet 35:558, 1998 |
|
Curry CRJ, Carey JC, Holland JS, et al: Smith-Lemli-Opitz syndrome–type II. Multiple congenital anomalies with male pseudohermaphroditism and frequent early lethality Am J Med Genet 26:45, 1987 |
|
Tint GS, Irons M, Elias ER, et al: Defective cholesterol biosynthesis associated with the Smith-Lemli-Opitz syndrome. N Engl J Med 330:107, 1994 |
|
Tinit GS, Batta AK, Xu G, et al: The Smith-Lemli-Opitz syndrome: A potentially fatal birth defect caused by a block in the last enzymatic step in cholesterol biosynthesis. Subcell Biochem 28:117, 1997 |
|
Bradley L, Palomaki GE, Knight GJ, et al: Levels of unconjugated estriol and other maternal serum markers in pregnancies with Smith-Lemli-Opitz (RSH) syndrome fetuses. Am J Med Genet 82:355, 1999 |
|
Parker KL, Schimmer BP: Steroidogenic factor 1: A key determinant of endocrine development and function. Endocr Rev 18:361, 1997 |
|
Luo X, Ikeda Y, Parkee KL: A cell-specific nuclear receptor is essential for adrenal and gonadal development and sexual differentiation. Cell 77:481, 1994 |
|
Acherman JC, Ito M, Ito M, et al: A mutation in the gene encoding steroidogenic factor-1 causes XY sex reversal and adrenal failure in humans. Nat Genet 22:125, 1999 |